Browse information
Latest Articles
Support
For Professionals
Search
Treatment
Home
Archive by Category "Treatment"
Treatment
Are all your medicines still helping? A guide to polypharmacy and medication reviews
by GAtherton
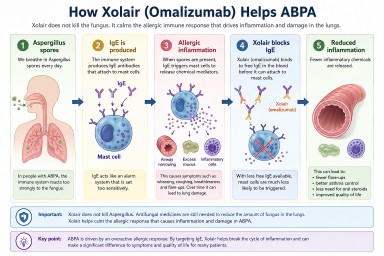
Why Can an Asthma Drug Help ABPA? Understanding Xolair (Omalizumab)
by GAtherton
Vaccinations for People Living with Aspergillosis
by GAtherton
Understanding Antibiotics: A Guide for People Living with Aspergillosis and Bronchiectasis
by GAtherton
Trying a New Diet? A Guide for People with Aspergillosis
by GAtherton
Loosen and Clear Mucus: Practical Self-Help Techniques for People with Aspergillosis
by GAtherton
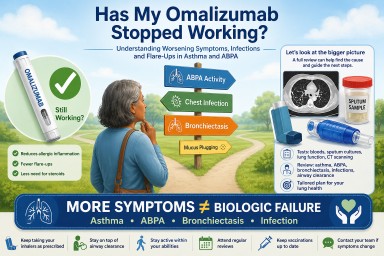
Has My Omalizumab Stopped Working? Understanding Worsening Symptoms, Infections and Flare-Ups in Asthma and ABPA
by GAtherton
Healthy Eating Should Not Feel Like Punishment
by GAtherton
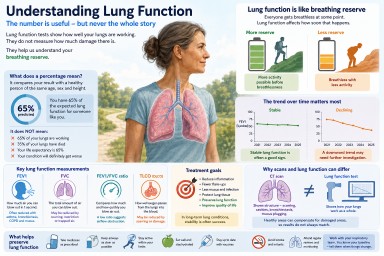
Understanding Lung Function in Aspergillosis and Asthma
by GAtherton
The Power of Keeping a Health Diary When You Have Aspergillosis
by GAtherton
1
2
3
…
22