Many people living with…
by GAtherton
Print out or share…
Mask Type Who Might Use……
If you live with asthma and…
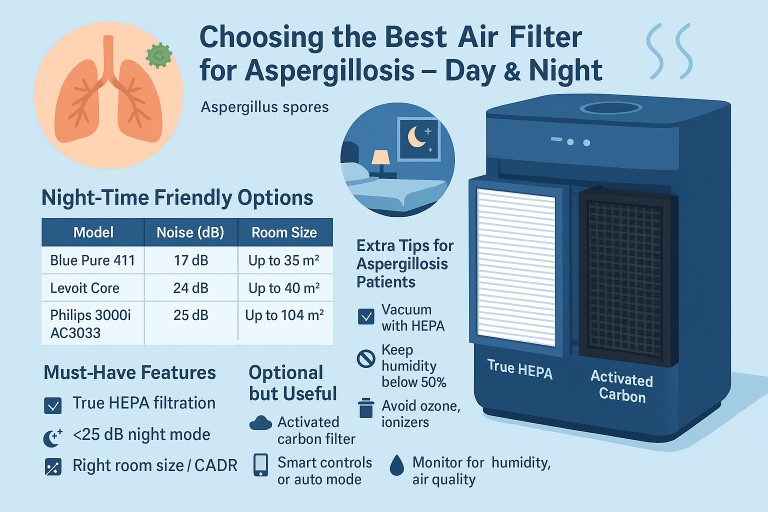
Living with aspergillosis…
Expert Information for…