When to suspect it, when to…
by GAtherton
Estimated prevalence 1–2% in…
It’s quite possible for…
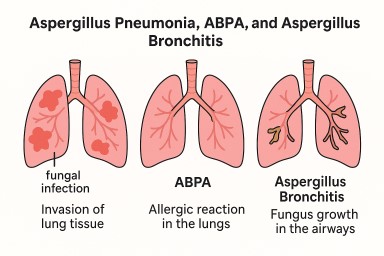
What is it? Aspergillus…
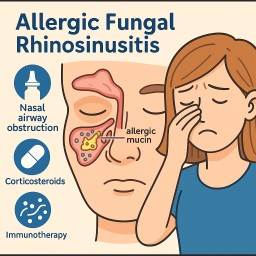
(Also called Allergic Fungal…
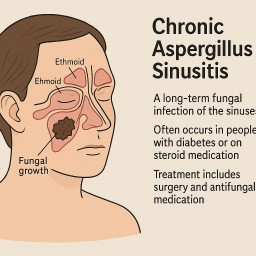
(Chronic invasive and…
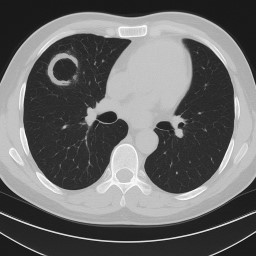
Aspergilloma (Fungal Ball in…