A Complete Guide for Patients…
by GAtherton
Many people living with…
Print out or share…
Mask Type Who Might Use……
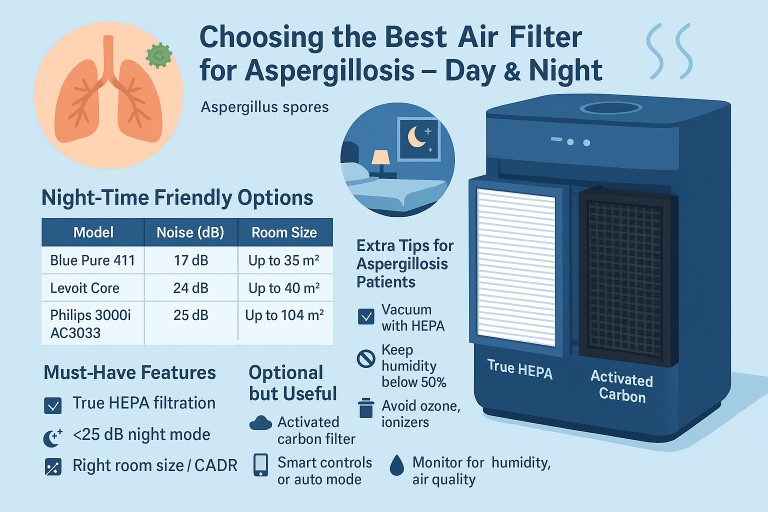
If you live with asthma and…
Living with aspergillosis…
Expert Information for…