How Aspergillus infections and allergic Aspergillus diseases are treated, monitored, and managed over time
Key points
- Management of aspergillosis includes treatment, monitoring, supportive care, and long-term follow-up.
- The right approach depends on the type of disease: Aspergillus infection is managed differently from allergic Aspergillus disease.
- Infection is usually managed with antifungal medicines, and sometimes procedures or surgery.
- Allergic disease is usually managed by controlling inflammation and the immune response, often alongside asthma or airway treatment.
- Management often needs regular review because medicines can cause side effects, drug interactions, and resistance problems, and the disease may change over time.
- Many patients need a long-term plan rather than a single short course of treatment.
Who is this page for? Patients, carers, general practitioners, and non-specialists who want to understand how aspergillosis is managed.
Please note: This page covers the wider management of aspergillosis, not just medicines. It includes treatment, monitoring, procedures, supportive care, and self-management.
What “management” means in aspergillosis
Management of aspergillosis includes much more than prescribing a medicine. It usually involves a combination of diagnosis, treatment, monitoring, supportive care, and long-term follow-up.
Some people need only a limited period of treatment. Others need a longer-term plan aimed at keeping the disease stable, reducing symptoms, preventing complications, and improving quality of life.
That is why management is often a better word than treatment. It reflects the fact that care may need to be adjusted over time.
Why management differs between types of aspergillosis
Aspergillosis is not one single disease. It is a group of conditions caused by the fungus Aspergillus.
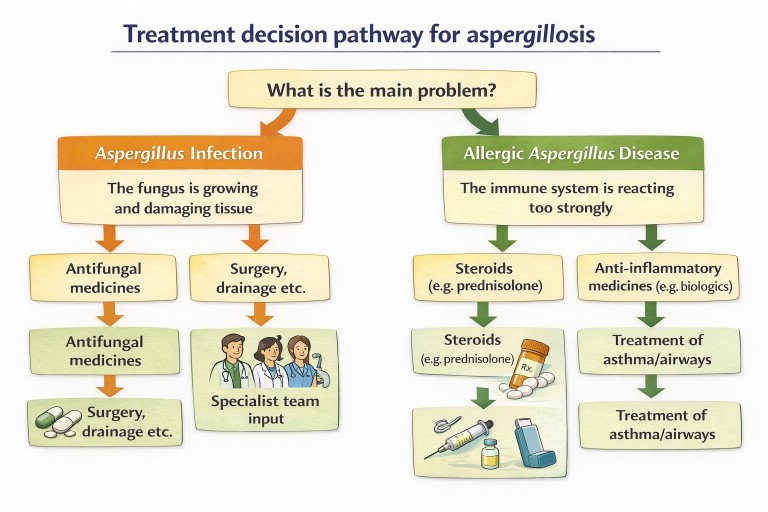
The two broad categories are:
- Aspergillus infection – where the fungus is growing in the lungs, airways, cavities, or tissues.
- Allergic Aspergillus disease – where the immune system is reacting too strongly to Aspergillus.
Because the underlying problem is different, the management is different too.
In infection, the aim is usually to reduce or stop fungal growth. In allergic disease, the aim is to reduce harmful inflammation and control the immune response.
Managing Aspergillus infection
The main treatment for Aspergillus infection is usually antifungal medicine. These medicines either stop the fungus growing or damage essential parts of the fungal cell.
The exact plan depends on the type of infection. Examples include:
- chronic pulmonary aspergillosis (CPA)
- aspergilloma
- Aspergillus nodules
- invasive aspergillosis
- other chronic or invasive Aspergillus infections
Some infections need long-term treatment over many months. Others need shorter intensive treatment, especially in hospital settings. In some cases, doctors may decide to monitor rather than treat immediately, particularly if findings are stable and symptoms are limited.
Antifungal medicines
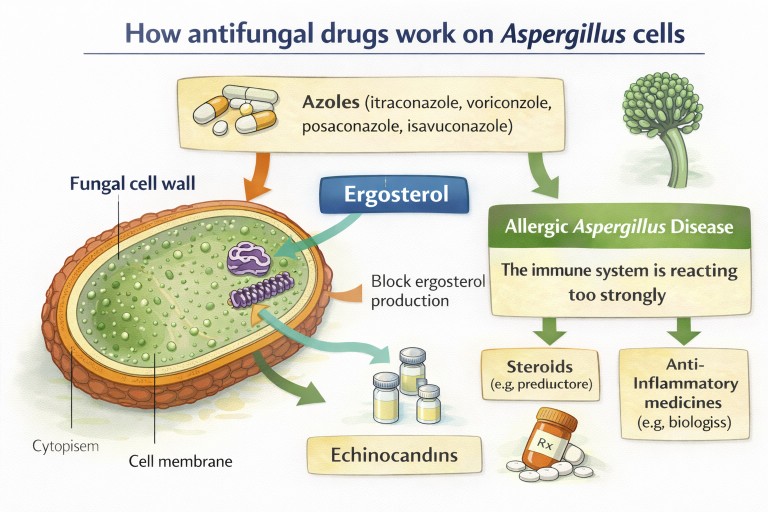
The most commonly used medicines for many forms of aspergillosis are from the azole group.
Itraconazole
Itraconazole is often used for chronic forms of aspergillosis and is sometimes also used in allergic disease to reduce the fungal burden in the airways.
Voriconazole
Voriconazole is widely used for more serious infection, especially invasive aspergillosis. It can be very effective, but it may also cause side effects and drug interactions that need careful monitoring.
Posaconazole
Posaconazole may be used when other azole medicines are not suitable, are not tolerated, or when resistance is suspected or confirmed.
Isavuconazole
Isavuconazole is a newer azole that is increasingly used in invasive disease and may be better tolerated by some patients.
Amphotericin B
Amphotericin B, usually given in hospital, is a powerful antifungal medicine often reserved for serious infection or special situations.
Echinocandins
Echinocandins are another class of antifungal drugs. They are more commonly used in hospital and may be part of treatment in selected patients.
How antifungal medicines work
Antifungal drugs work by targeting structures or processes that fungal cells need in order to survive.
- Azoles interfere with production of ergosterol, an important part of the fungal cell membrane.
- Amphotericin B binds to the fungal membrane and damages it.
- Echinocandins interfere with fungal cell wall production.
Because these drugs target fungal biology, they can slow growth, weaken the fungus, or kill it, depending on the drug, the organism, and the clinical situation.
Monitoring treatment
Antifungal treatment often needs careful monitoring. This is important because the dose may need adjusting, some drugs interact with other medicines, and side effects can occur.
Doctors may monitor:
- symptoms and quality of life
- blood levels of the antifungal medicine
- liver function tests
- kidney function in some cases
- repeat scans
- blood markers or antibody levels in selected situations
Monitoring helps clinicians judge whether treatment is helping, whether drug exposure is adequate, and whether side effects are developing.
Monitoring and long-term follow-up
Many forms of aspergillosis are long-term conditions. Even when symptoms improve, doctors usually continue to monitor patients over time to make sure the disease remains stable and treatment remains safe.
Follow-up care may involve regular clinic appointments, blood tests, scans, and review of symptoms.
Why monitoring is important
Monitoring helps doctors to:
- check whether treatment is working
- detect disease progression early
- identify medication side effects
- adjust drug doses if needed
- detect antifungal resistance
- decide when treatment can be reduced or stopped
Symptoms doctors may monitor
Patients are often asked about changes in:
- breathlessness
- cough and mucus production
- fatigue and exercise tolerance
- chest discomfort
- coughing up blood
- frequency of chest infections
Blood tests
Blood tests are often used to monitor both the disease and the treatment.
Depending on the condition, doctors may check:
- drug levels of antifungal medicines
- liver function tests
- kidney function
- inflammatory markers
- Aspergillus antibody levels, such as Aspergillus immunoglobulin G (IgG), in selected patients
- allergy markers such as total immunoglobulin E (IgE) in allergic disease
Imaging
Computed tomography (CT) scans are often repeated during follow-up.
Imaging can show:
- whether cavities are stable or changing
- whether fungal balls are growing
- whether inflammation has improved
- whether new lung problems have appeared
Sputum testing
In some patients, sputum samples are tested periodically to look for:
- Aspergillus growth
- bacterial infections
- changes in fungal susceptibility to antifungal medicines
Long-term outlook
The course of aspergillosis varies between individuals. Some patients remain stable for many years with appropriate treatment and monitoring. Others experience periods of improvement followed by flare-ups.
Surgery and other procedures
Medicines are not the only management option. In some situations, surgery or other procedures may be considered.
Examples include:
- removal of an aspergilloma causing repeated bleeding
- removal of an isolated fungal nodule
- drainage or other procedures in selected cases
- bronchial artery embolisation to help control severe coughing up blood
Surgery is not suitable for everyone. The risks and benefits depend on the location of disease, how much lung reserve a patient has, other medical problems, and how severe the symptoms are.
Managing allergic Aspergillus disease
In allergic Aspergillus disease, the main problem is not usually tissue invasion by the fungus. Instead, it is the immune reaction that causes trouble.
This means management often focuses on:
- reducing allergic inflammation
- improving asthma or airway control
- reducing mucus plugging
- sometimes reducing fungal burden in the airways as well
Corticosteroids
Corticosteroids are commonly used to damp down inflammation in conditions such as allergic bronchopulmonary aspergillosis (ABPA). They can be very effective, but long-term use can cause important side effects.
Antifungal therapy in allergic disease
Some patients with allergic disease are also treated with antifungal medicines. In this setting, the aim is often to reduce the amount of Aspergillus in the airways and therefore reduce the allergic stimulus.
Biologic therapies
Biologic therapies are increasingly important in severe asthma and some cases of ABPA. These drugs target specific parts of the immune system involved in allergic inflammation.
Examples include:
- omalizumab – targets immunoglobulin E (IgE)
- mepolizumab – targets interleukin-5 (IL-5)
- benralizumab – targets the interleukin-5 receptor
- dupilumab – targets interleukin-4/interleukin-13 pathways
These medicines may help reduce flare-ups, improve asthma control, and reduce reliance on oral steroids in selected patients.
Supportive care
Many patients benefit from supportive care alongside their main therapy. This part is easy to overlook, but it can make a major difference to symptoms and day-to-day life.
Supportive care may include:
- airway clearance techniques
- inhalers for asthma or chronic obstructive pulmonary disease (COPD)
- bronchiectasis management
- treatment of bacterial co-infection if present
- pulmonary rehabilitation
- nutritional support in selected patients
- monitoring for coughing up blood, worsening breathlessness, or medication side effects
Environmental exposure and lifestyle
Because Aspergillus is a common environmental fungus, many patients ask whether reducing exposure can help manage their condition.
It is impossible to avoid Aspergillus completely, but some practical measures may help reduce heavy exposure:
- avoiding activities that generate large amounts of mould spores, such as handling compost, rotting leaves, or heavily mouldy material
- using an appropriate protective mask if exposure cannot be avoided
- addressing damp or mould problems in the home
- maintaining good ventilation indoors
- avoiding staying in mouldy environments where possible, especially for people with asthma, chronic lung disease, or weakened immunity
These steps do not replace medical treatment, but they may reduce repeated exposure that could worsen symptoms in some patients.
Drug interactions and antifungal resistance
Drug interactions
Azole antifungal medicines can interact with many other medicines. This is one reason why careful review and monitoring are so important.
Interactions may occur with drugs such as:
- some statins
- some anticoagulants
- certain antibiotics
- transplant medicines
- steroids
- other drugs metabolised through the liver
Patients should always tell their clinical team about all prescribed medicines, over-the-counter products, and supplements.
Antifungal resistance
Some Aspergillus strains are resistant to azole antifungal drugs. Resistance may be present before treatment starts or may become more obvious when a patient does not respond as expected.
Where possible, laboratories may perform susceptibility testing on clinically relevant Aspergillus isolates. This helps doctors decide whether the current antifungal is likely to work.
Managing flare-ups or deterioration
Aspergillosis management sometimes needs to change because symptoms worsen or scans show progression.
Possible warning signs include:
- increasing cough or sputum
- worsening breathlessness
- new or increased coughing up blood
- weight loss
- increasing fatigue
- declining asthma control
When this happens, doctors may need to reassess the situation with repeat imaging, sputum testing, blood tests, medication review, or a change in treatment plan.
Multidisciplinary care
Complex aspergillosis is often best managed by a multidisciplinary team. Depending on the patient’s situation, this may include:
- respiratory physicians
- infectious diseases specialists
- clinical microbiology or mycology laboratories
- radiologists
- pharmacists
- physiotherapists
- specialist nurses
- thoracic surgeons or interventional radiologists in selected cases
This team approach is particularly helpful when patients have overlapping conditions such as bronchiectasis, severe asthma, chronic obstructive pulmonary disease (COPD), non-tuberculous mycobacterial disease, or significant medication problems.
Self-management and living with aspergillosis
Patients also play an important role in management. Good self-management does not replace specialist care, but it can make a real difference.
Important areas include:
- taking medicines as prescribed
- reporting side effects early
- keeping track of symptoms and flare-ups
- using airway clearance techniques if advised
- pacing activity and managing fatigue
- attending follow-up appointments and blood tests
- asking for help if mental wellbeing is affected by long-term illness
For many people, successful management means finding a way to live as fully as possible while keeping the disease under the best control that is realistically achievable.
How doctors choose the best management plan
Doctors do not choose management based on the name of the disease alone. They also consider:
- the exact form of aspergillosis
- how severe it is
- whether the disease is stable or progressing
- lung health and other medical conditions
- immune status
- possible drug interactions
- the chance of side effects
- whether antifungal resistance is likely
- what the patient can realistically tolerate and manage
In more complex cases, these decisions are often best made in a specialist setting or through a multidisciplinary team discussion.
Specialist services in the United Kingdom
Patients in the United Kingdom with complex or difficult-to-manage aspergillosis may be referred to the
National Aspergillosis Centre (NAC) in Manchester.
The National Aspergillosis Centre is based at the North West Lung Centre at Wythenshawe Hospital,
part of Manchester University NHS Foundation Trust. The service was commissioned by the NHS to provide specialist expertise in the diagnosis and management of aspergillosis, particularly chronic pulmonary aspergillosis (CPA).
Visit the National Aspergillosis Centre website.
The centre provides:
- specialist assessment and long-term management of chronic pulmonary aspergillosis and related diseases
- diagnostic expertise and access to specialised fungal laboratory testing
- multidisciplinary review of complex cases
- advice and guidance to clinicians across the UK
- support for research and development of new antifungal treatments and diagnostics
Patients are usually referred to the centre by their respiratory physician or another hospital consultant.
Many patients continue to receive most of their care locally, with specialist advice provided by the National Aspergillosis Centre when needed.
Common questions patients ask
How long does management last?
It varies. Some people need treatment for weeks or months, while others need much longer-term management with monitoring and adjustment over time.
Do antifungal medicines cure aspergillosis?
Sometimes they can clear infection, but in many chronic conditions the aim is to control the disease, improve symptoms, and prevent worsening.
Why is monitoring so important?
Because antifungal drug levels, side effects, drug interactions, and disease progression can all affect whether management is safe and effective.
Why are steroids used if Aspergillus is a fungus?
In allergic disease, the main problem is often the immune reaction rather than direct fungal damage. Steroids are used to calm that inflammation.
Can someone need both antifungal treatment and anti-inflammatory treatment?
Yes. Some patients have overlapping problems and may need a combination approach.
When to seek medical advice
Seek medical advice if you develop:
- worsening breathlessness
- persistent fever
- coughing up blood
- severe fatigue or loss of appetite
- possible medication side effects such as jaundice or new visual or neurological symptoms
- new wheeze, chest tightness, or worsening asthma control
Early review can help doctors decide whether management needs to be changed, intensified, reduced, or monitored more closely.
References
- Patterson TF, Thompson GR 3rd, Denning DW, Fishman JA, Hadley S, Herbrecht R, Kontoyiannis DP, Marr KA, Morrison VA, Nguyen MH, Segal BH, Steinbach WJ, Stevens DA, Walsh TJ, Wingard JR, Young JA, Bennett JE. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016 Aug 15;63(4):e1-e60. doi: 10.1093/cid/ciw326. Epub 2016 Jun 29. PMID: 27365388; PMCID: PMC4967602.
- Denning DW, Cadranel J, Beigelman-Aubry C, Ader F, Chakrabarti A, Blot S, Ullmann AJ, Dimopoulos G, Lange C; European Society for Clinical Microbiology and Infectious Diseases and European Respiratory Society. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J. 2016 Jan;47(1):45-68. doi: 10.1183/13993003.00583-2015. PMID: 26699723.
- Ullmann AJ, Aguado JM, Arikan-Akdagli S, Denning DW, Groll AH, Lagrou K, Lass-Flörl C, Lewis RE, Munoz P, Verweij PE, Warris A, Ader F, Akova M, Arendrup MC, Barnes RA, Beigelman-Aubry C, Blot S, Bouza E, Brüggemann RJM, Buchheidt D, Cadranel J, Castagnola E, Chakrabarti A, Cuenca-Estrella M, Dimopoulos G, Fortun J, Gangneux JP, Garbino J, Heinz WJ, Herbrecht R, Heussel CP, Kibbler CC, Klimko N, Kullberg BJ, Lange C, Lehrnbecher T, Löffler J, Lortholary O, Maertens J, Marchetti O, Meis JF, Pagano L, Ribaud P, Richardson M, Roilides E, Ruhnke M, Sanguinetti M, Sheppard DC, Sinkó J, Skiada A, Vehreschild MJGT, Viscoli C, Cornely OA. Diagnosis and management of Aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin Microbiol Infect. 2018 May;24 Suppl 1:e1-e38. doi: 10.1016/j.cmi.2018.01.002. Epub 2018 Mar 12. PMID: 29544767.
- Agarwal R, Sehgal IS, Muthu V, Denning DW, Chakrabarti A, Soundappan K, Garg M, Rudramurthy SM, Dhooria S, Armstrong-James D, Asano K, Gangneux JP, Chotirmall SH, Salzer HJF, Chalmers JD, Godet C, Joest M, Page I, Nair P, Arjun P, Dhar R, Jat KR, Joe G, Krishnaswamy UM, Mathew JL, Maturu VN, Mohan A, Nath A, Patel D, Savio J, Saxena P, Soman R, Thangakunam B, Baxter CG, Bongomin F, Calhoun WJ, Cornely OA, Douglass JA, Kosmidis C, Meis JF, Moss R, Pasqualotto AC, Seidel D, Sprute R, Prasad KT, Aggarwal AN. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses. Eur Respir J. 2024 Apr 4;63(4):2400061. doi: 10.1183/13993003.00061-2024. PMID: 38423624; PMCID: PMC10991853.