Browse information
Latest Articles
Support
For Professionals
Search
adrenal-insufficiency
Home
Posts Tagged "adrenal-insufficiency"
adrenal-insufficiency
Understanding Steroids, Cortisol, ACTH and Adrenal Suppression in Aspergillosis
by GAtherton
Hydrocortisone dosing in adrenal insufficiency
Why adrenal insufficiency can…
by GAtherton
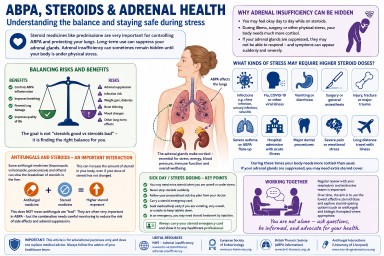
**Adrenal Insufficiency & Steroid Tapering:
A Complete Patient Guide**…
by GAtherton