How doctors diagnose allergic reactions to Aspergillus in the lungs
Key points
- This page explains how doctors diagnose allergic diseases caused by Aspergillus, rather than Aspergillus infection.
- The best-known allergic form is allergic bronchopulmonary aspergillosis (ABPA).
- Another related condition is severe asthma with fungal sensitisation (SAFS).
- In allergic disease, the main problem is an exaggerated immune reaction to Aspergillus, rather than fungal growth directly damaging tissue.
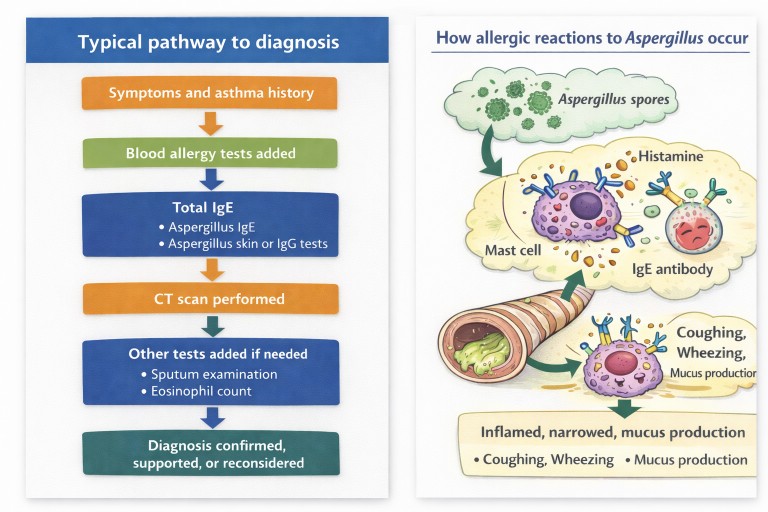
- Diagnosis usually depends on a combination of symptoms, asthma history, blood tests, imaging, and sometimes sputum tests.
- The most important tests often include total immunoglobulin E (IgE), Aspergillus-specific IgE, eosinophil count, and a computed tomography (CT) scan.
Who is this page for? Patients, carers, general practitioners, and non-specialists who want to understand how allergic Aspergillus diseases are diagnosed.
Please note: This page is about allergic Aspergillus disease. Diagnosis of Aspergillus infection, such as chronic pulmonary aspergillosis (CPA), uses a different emphasis and is best covered separately.
What is allergic Aspergillus disease?
Aspergillus is a group of moulds commonly found in the environment. Most people breathe in Aspergillus spores regularly without becoming unwell.
In some people, however, the immune system becomes over-sensitive to Aspergillus. Instead of ignoring the spores, it reacts strongly. This reaction can cause airway inflammation, mucus production, coughing, wheezing, and worsening asthma symptoms.
Unlike Aspergillus infection, where the fungus itself is growing and causing damage, allergic Aspergillus disease is mainly driven by the body’s immune response.
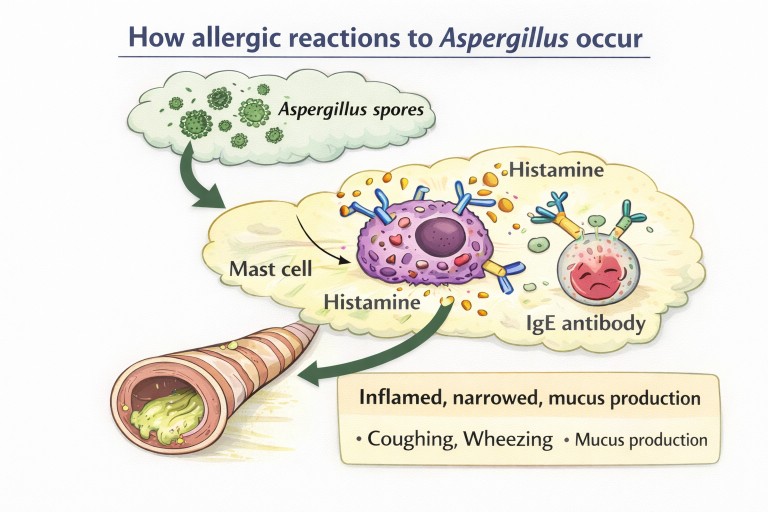
Why allergic reactions to Aspergillus happen
Allergic Aspergillus disease usually happens in people who already have an underlying airway condition, especially asthma or sometimes cystic fibrosis or bronchiectasis.
In these conditions, mucus may build up in the airways and spores may remain there longer than usual. The immune system may then become sensitised to Aspergillus and start to recognise it as a threat.
Once sensitisation has happened, breathing in Aspergillus spores can trigger an allergic response involving:
- immunoglobulin E (IgE)
- mast cells
- eosinophils
- release of inflammatory chemicals
- airway swelling, narrowing, and mucus production
This is why many patients develop symptoms such as wheeze, cough, chest tightness, increased mucus, and repeated flare-ups.
Main allergic Aspergillus conditions
Allergic bronchopulmonary aspergillosis (ABPA)
Allergic bronchopulmonary aspergillosis (ABPA) is the best-known allergic Aspergillus condition. It usually occurs in people with asthma or cystic fibrosis, although it can occasionally appear in other settings too.
In ABPA, the immune system reacts strongly to Aspergillus in the airways. This can lead to:
- worsening asthma
- cough
- thick mucus or mucus plugs
- breathlessness
- recurrent chest flare-ups
- bronchiectasis over time
Severe asthma with fungal sensitisation (SAFS)
Severe asthma with fungal sensitisation (SAFS) refers to patients with severe asthma who are sensitised to fungi such as Aspergillus, but who do not meet the full criteria for ABPA.
These patients may still have significant fungal-driven airway inflammation, but the pattern is not the same as classic ABPA.
How doctors diagnose allergic Aspergillus disease
Doctors usually diagnose allergic Aspergillus disease by combining several different types of evidence:
- symptoms and history, especially asthma history
- blood tests showing allergic sensitisation
- blood tests showing the degree of allergic activity
- computed tomography (CT) scan findings
- sometimes sputum findings
The overall aim is to show that:
- the patient is sensitised to Aspergillus
- the immune system is reacting strongly enough to cause disease
- the lungs show changes that fit that diagnosis
- other explanations do not fit better
Blood tests
Blood tests are central to diagnosing allergic forms of aspergillosis.
Total immunoglobulin E (IgE)
Total IgE is a measure of overall allergic immune activity. In ABPA, it is often substantially raised. It helps show that a strong allergic process may be taking place.
Aspergillus-specific immunoglobulin E (IgE)
This test measures whether the immune system has made IgE antibodies specifically against Aspergillus. A positive result shows that the immune system recognises Aspergillus as an allergen.
Aspergillus-specific immunoglobulin G (IgG)
Aspergillus IgG may also be measured. It can help support the overall picture, although it is not as specific for allergic disease as Aspergillus-specific IgE. It is often more associated with chronic infection, so the result has to be interpreted carefully.
Eosinophil count
Eosinophils are white blood cells involved in allergic inflammation. Many patients with ABPA have raised eosinophils, although not all do. Steroid treatment can also reduce the eosinophil count, which may affect interpretation.
Skin allergy testing
Some patients have a skin prick test using Aspergillus allergen. If the immune system is sensitised, a small raised itchy bump appears at the skin test site.
This can provide useful evidence of sensitisation, although many centres now rely more on blood tests.
Computed tomography (CT) scans and imaging
A computed tomography (CT) scan helps doctors look for airway changes that support the diagnosis.
Findings may include:
- central bronchiectasis
- mucus plugging
- airway wall thickening
- patchy collapse or inflammation in some areas of lung
These findings do not prove ABPA on their own, but they can strongly support the diagnosis when the blood tests and history fit.
Sputum tests
Sputum may sometimes show:
- Aspergillus growth
- mucus plugs
- eosinophils
However, the presence of Aspergillus in sputum does not on its own prove allergic disease. It has to be interpreted alongside the patient’s symptoms, allergy tests, and scans.
Diagnostic criteria for allergic bronchopulmonary aspergillosis (ABPA)
Doctors usually diagnose ABPA using a combination of features rather than a single test. Depending on the guideline used, these may include:
- asthma or cystic fibrosis
- evidence of Aspergillus sensitisation, usually Aspergillus-specific IgE
- a raised total IgE
- supportive findings such as raised eosinophils
- CT scan changes such as central bronchiectasis or mucus plugging
Not every patient has every feature, and some patients sit somewhere between clear-cut categories. That is why doctors look at the whole pattern.
Why several tests are often needed
No single test can diagnose allergic Aspergillus disease on its own.
For example, a raised total IgE shows allergic activity, but not necessarily that Aspergillus is the cause. A positive Aspergillus-specific IgE shows sensitisation, but not necessarily that the patient has ABPA. A CT scan may show bronchiectasis, but bronchiectasis has many causes.
Doctors therefore combine the evidence:
- Do the symptoms fit?
- Is there asthma or another predisposing airway condition?
- Is there clear Aspergillus sensitisation?
- Are the allergic markers sufficiently raised?
- Do the scans show changes that support the diagnosis?
When several of these line up, the diagnosis becomes much more reliable.
Common questions patients ask
If Aspergillus is common in the air, why do only some people develop allergic disease?
Only some people become sensitised. Underlying asthma, airway disease, genetic factors, and repeated exposure may all contribute.
Is allergic bronchopulmonary aspergillosis (ABPA) the same as infection?
No. In ABPA, the main problem is the immune reaction to Aspergillus. In infection, the fungus itself is growing in a way that causes direct disease.
Can someone have both allergy and infection?
Yes, in some circumstances, a person may have overlapping problems, which can make diagnosis more complicated.
Why are eosinophils important?
Eosinophils are part of the allergic inflammatory response. A raised eosinophil count can support the diagnosis, although it is not present in every patient and can be lowered by steroid treatment.
When to seek medical advice
Seek medical advice if you have:
- worsening asthma control
- frequent chest flare-ups
- persistent cough or thick mucus
- wheezing that is getting worse
- unexplained breathlessness
- new mucus plugging or bronchiectasis on imaging
Earlier diagnosis can help reduce inflammation and may help prevent longer-term airway damage.
References
- Agarwal R, Chakrabarti A, Shah A, et al. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis and related mycoses.
- Patterson KC, Strek ME. Allergic bronchopulmonary aspergillosis. Proceedings of the American Thoracic Society.
- Reviews on severe asthma with fungal sensitisation (SAFS), Aspergillus sensitisation, eosinophilic airway disease, and fungal allergy in asthma may also be helpful for a fuller professional companion page.