clinician explainer
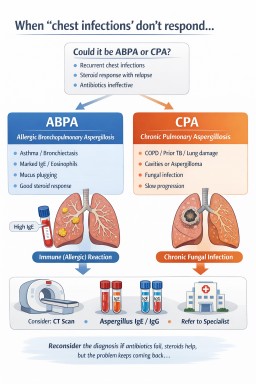
When ‘chest infections’ don’t respond: when to suspect ABPA or CPA (Clinical perspective)
Patients presenting with…
When ‘chest infections’ don’t respond: when to suspect ABPA or CPA (Patient guide)
Patients presenting with…
Patients presenting with…
Patients presenting with…