by GAtherton
People living with Allergic…
A calm, supportive guide for…
Many people living with…
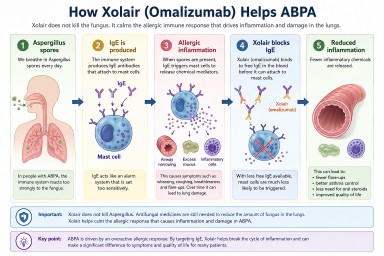
Many people with allergic…
Many patients with Allergic…
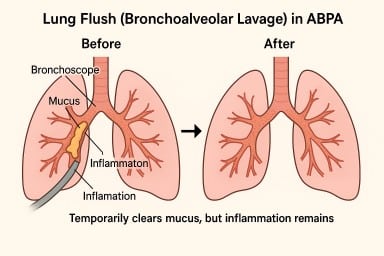
A lung flush (also called a…
Many patients with ABPA,…
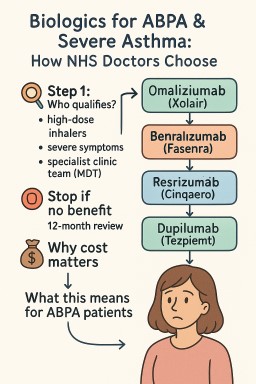
Biologics are modern…
Print out or share…