Originally published: 8 July 2026
Last reviewed: 8 July 2026
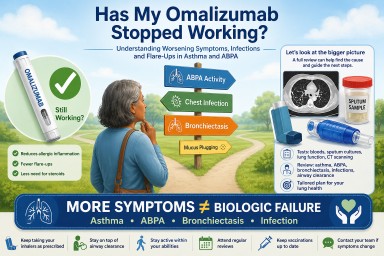
Many people diagnosed with Allergic Bronchopulmonary Aspergillosis (ABPA) are surprised when their specialist suggests Xolair (omalizumab).
“I thought Xolair was an asthma medication. How can it possibly help a fungal lung disease?”
It is a very reasonable question.
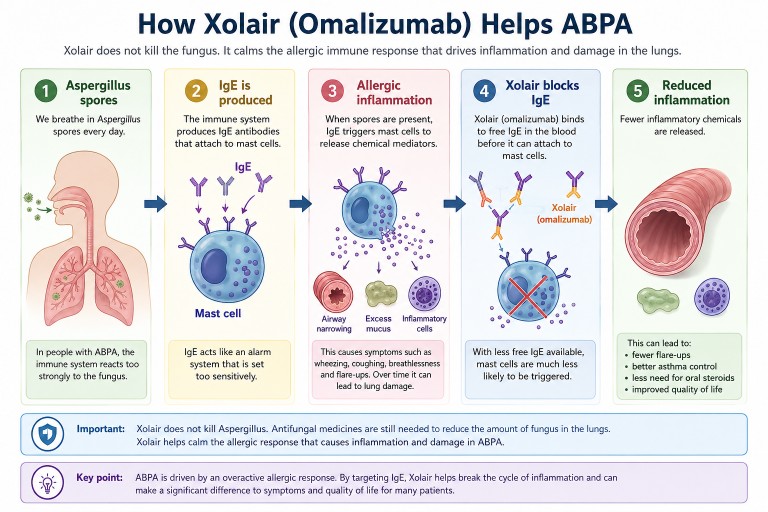
The answer is that ABPA is not simply an infection caused by Aspergillus. It is an allergic lung disease in which the immune system overreacts to the presence of Aspergillus in the airways.
Xolair does not kill the fungus. Instead, it helps calm the allergic immune response that drives many of the symptoms of ABPA.
Key Points
- Xolair (omalizumab) is a biologic medicine originally developed for severe allergic asthma.
- Many people with ABPA also have severe allergic asthma.
- Omalizumab targets IgE, an antibody involved in allergic inflammation.
- In the UK, omalizumab is usually prescribed through NHS severe asthma pathways, not because ABPA itself is a licensed indication.
- Treating severe allergic asthma can also improve ABPA because the two conditions share important allergic immune pathways.
- Biosimilar versions of omalizumab are now becoming available, which may make biologic treatment more accessible for eligible patients.
Understanding ABPA
Everyone breathes in Aspergillus spores every day.
For most people, this causes no illness. In people with ABPA, however, the immune system reacts too strongly. Instead of ignoring the spores, it launches an exaggerated allergic response.
This can cause:
- airway inflammation
- wheezing
- coughing
- breathlessness
- excessive mucus production
- repeated flare-ups
- gradual lung damage if poorly controlled.
In many patients, the allergic response causes more problems than the fungus itself.
That is why doctors may treat both the amount of fungus in the airways and the immune system’s overreaction to it.
What Does IgE Have To Do With ABPA?
One of the key parts of allergic disease is an antibody called Immunoglobulin E, usually shortened to IgE.
Think of IgE as part of the body’s allergy alarm system.
In ABPA, the immune system produces IgE against Aspergillus. This can trigger immune cells to release chemicals that cause allergic inflammation. These chemicals narrow the airways, increase mucus production and attract other inflammatory cells, including eosinophils.
Doctors often measure total IgE because it is important in diagnosing and monitoring ABPA.
How Does Xolair Work?
Xolair (omalizumab) is a biologic medicine. Biologics are targeted treatments designed to block specific parts of the immune system.
Omalizumab attaches to free IgE antibodies before they can trigger the allergic cascade.
As a result:
- allergic inflammation may be reduced
- asthma symptoms may improve
- flare-ups may become less frequent
- some patients may be able to reduce oral steroid treatment
- quality of life may improve.
Xolair does not kill Aspergillus.
Instead, it reduces the body’s excessive allergic response to the fungus.
Why Was I Offered An Asthma Drug?
This is one of the most common questions patients ask.
Although ABPA is a distinct condition, many people with ABPA also have severe allergic asthma. The two conditions share many of the same allergic immune pathways, particularly those involving IgE.
In the UK, omalizumab is not currently licensed specifically for ABPA.
Many patients receive omalizumab because they meet NHS eligibility criteria for severe allergic asthma. When the allergic asthma improves, the ABPA may also improve because both conditions are driven by overlapping allergic inflammation.
In other words, the treatment is not aimed at killing Aspergillus. It is aimed at reducing the allergic inflammation that contributes to both severe asthma and ABPA.
Why Can’t Everyone With ABPA Have Xolair?
This is an important question.
In the NHS, access to omalizumab is usually based on nationally agreed eligibility criteria for licensed conditions such as severe allergic asthma. A diagnosis of ABPA alone does not usually make someone eligible for omalizumab treatment.
This does not mean omalizumab cannot help some people with ABPA. It means that NHS prescribing is guided by licensing, NICE recommendations, commissioning arrangements and clinical judgement.
Your respiratory specialist will consider your asthma severity, ABPA history, IgE levels, previous treatments, steroid exposure, flare-up frequency and overall health when deciding whether a biologic medicine may be appropriate.
Why Aren’t Antifungal Drugs Enough?
Antifungal medicines such as itraconazole or voriconazole reduce the amount of Aspergillus growing in the airways.
However, reducing the fungus does not always completely switch off the allergic immune response.
Different treatments target different parts of the disease:
| Treatment | Main purpose |
|---|---|
| Antifungal medicines | Reduce the amount of Aspergillus |
| Corticosteroids | Reduce widespread inflammation |
| Biologics such as omalizumab | Target specific allergic pathways |
| Airway clearance | Help remove mucus from the lungs |
These treatments often work together rather than replacing one another.
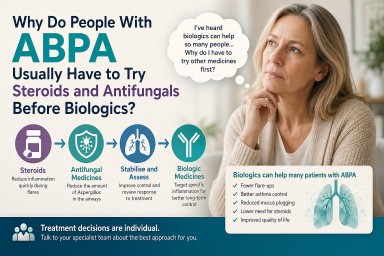
Why Have Steroids Been Used For So Long?
For many years, oral corticosteroids such as prednisolone have been a main treatment for ABPA.
Steroids are often effective at controlling inflammation quickly, but prolonged or repeated courses can cause significant side effects, including:
- weight gain
- diabetes
- osteoporosis
- cataracts
- mood changes
- increased infection risk
- adrenal suppression or adrenal insufficiency.
One reason biologics are important is that they may help some suitable patients reduce their need for long-term oral steroids under specialist supervision.
Does Xolair Help Everyone?
No.
Some patients experience major improvements. Others notice more gradual changes. A small number may gain little benefit and may be better suited to a different biologic medicine.
Published studies and specialist-centre experience suggest that some patients with ABPA treated with omalizumab may experience:
- fewer exacerbations
- better asthma control
- reduced oral steroid requirements
- improved quality of life.
Because ABPA is relatively uncommon, much of the evidence comes from case series, observational studies, smaller trials and systematic reviews rather than the very large trials often performed for common diseases.
Why Isn’t Xolair Licensed Specifically For ABPA?
This can be confusing for patients.
Being “not licensed for ABPA” does not necessarily mean there is no evidence that omalizumab can help. It means that the medicine has not gone through the formal licensing process for ABPA as a specific indication.
Licensing a medicine for a new condition usually requires large, expensive clinical trials. ABPA is a relatively uncommon disease, which makes such studies difficult to organise and fund.
There is also less commercial incentive now that omalizumab biosimilars are becoming available. No single manufacturer may have a strong reason to fund large registration trials for an additional ABPA indication.
As a result, the scientific evidence and clinical experience have grown faster than the formal licensing process.
Why Is Omalizumab Back In The News?
Omalizumab itself is not new. It has been used for severe allergic asthma for more than twenty years.
What is new is the increasing availability of biosimilar omalizumab.
Biosimilars are highly similar versions of an existing biologic medicine. They must show comparable quality, safety and effectiveness before approval.
This matters because biologic medicines are expensive. Increased competition from biosimilars is expected to reduce costs over time.
Lower costs may improve access for patients who meet NHS eligibility criteria and may also increase research interest in biologic treatment for conditions such as ABPA.
It is important not to overpromise: biosimilars do not automatically mean that everyone with ABPA will be offered omalizumab. NHS access will still depend on eligibility criteria, clinical assessment and local pathways.
Are There Other Biologics?
Yes.
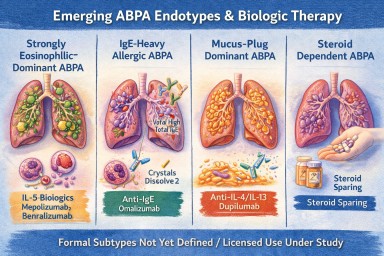
Omalizumab was the first biologic widely used in allergic asthma and has been used in selected patients with ABPA. Newer biologics target different parts of the allergic inflammatory pathway.
Depending on an individual’s disease pattern, specialists may consider medicines such as:
- mepolizumab
- benralizumab
- dupilumab
- tezepelumab.
Research is continuing to determine which patients are most likely to benefit from each biologic.
Questions You May Wish To Ask Your Specialist
- Why do you think omalizumab is appropriate for me?
- Am I being considered for this because of severe allergic asthma, ABPA, or both?
- How long before we know whether it is working?
- Will I still need antifungal treatment?
- Could this help reduce my oral steroid dose?
- What side effects should I watch for?
- Would another biologic be more suitable for my type of inflammation?
The Bottom Line
Xolair (omalizumab) was originally developed for severe allergic asthma, but it can also help some people with ABPA because ABPA is strongly driven by allergic immune inflammation.
In the NHS, omalizumab is usually prescribed through severe asthma pathways rather than because ABPA itself is a licensed indication.
It is not an antifungal drug and it is not a cure for ABPA. Instead, it is part of a modern treatment approach that may include antifungal medicines, airway clearance, corticosteroids, monitoring and biologic therapy in selected patients.
With biosimilar omalizumab becoming available and newer biologics continuing to emerge, treatment options for severe allergic lung disease are changing. For people living with ABPA, this is an important and rapidly developing area of care.
Related Articles
- Understanding Biologic Treatments for Aspergillosis
- ABPA: A Complete Patient Guide
- Understanding Steroids, Cortisol, ACTH and Adrenal Suppression
- Can Biologics Reduce the Need for Steroids?