How doctors work out whether Aspergillus is truly causing infection
Key points
- This page is about Aspergillus infection diagnostics, not allergic conditions such as allergic bronchopulmonary aspergillosis (ABPA), severe asthma with fungal sensitisation (SAFS), or simple fungal allergy.
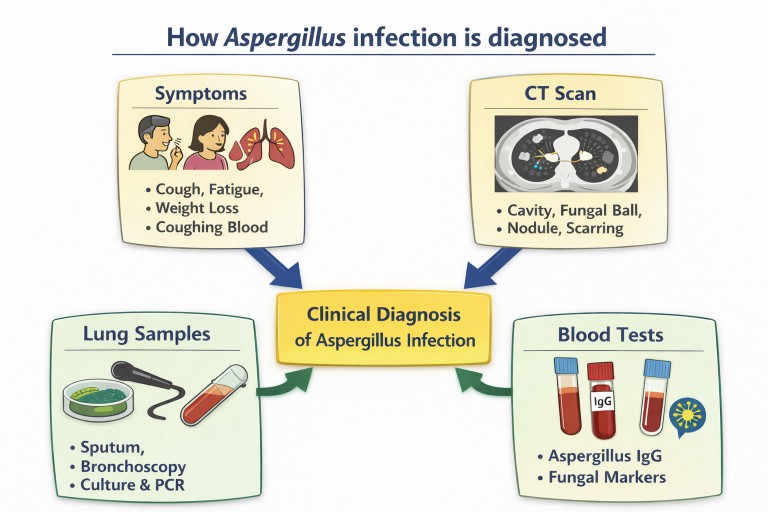
- Doctors usually diagnose Aspergillus infection using a combination of symptoms, scans, laboratory tests, and clinical judgement.
- No single test is perfect. Results need to be interpreted in context.
- Important tests include computed tomography (CT) scans, sputum or bronchoscopy samples, fungal culture, polymerase chain reaction (PCR), antigen tests, and Aspergillus immunoglobulin G (IgG).
- Newer approaches increasingly try to detect parts of the fungus itself, such as fungal DNA or fungal cell wall molecules, rather than only measuring the body’s immune response.
- These newer approaches may help make diagnosis faster, earlier, and more accurate.
Who is this page for? Patients, carers, general practitioners, and non-specialists who want to understand how Aspergillus infections are diagnosed.
Please note: This article explains diagnosis of infection. Tests used mainly for allergic disease are important too, but are best covered separately because the questions doctors are asking are different.
Why diagnosis matters
Aspergillus is a group of common moulds found widely in the environment. We all breathe in tiny Aspergillus spores regularly. In most people, this causes no problem. In some people, however, Aspergillus can grow in the lungs or in existing lung cavities and cause infection.
Getting the diagnosis right matters because treatment decisions depend on it. Antifungal medicines can be very important, but they can also have side effects, interact with other medicines, and may not be needed if Aspergillus is only present in a harmless or less harmful way. Doctors therefore try to answer a very specific question: is Aspergillus really causing disease here, or is it simply present?
Infection is not the same as allergy
This page is specifically about diagnosing Aspergillus infection in the lungs.
That is different from diagnosing allergic disease caused by Aspergillus, where the main problem is an over-active immune response rather than fungal growth causing tissue damage. Allergic conditions include allergic bronchopulmonary aspergillosis (ABPA) and severe asthma with fungal sensitisation (SAFS).
In infection, doctors are looking for evidence that Aspergillus is actually growing, persisting, or damaging tissue. This may include conditions such as:
- chronic pulmonary aspergillosis (CPA)
- aspergilloma (a fungal ball)
- Aspergillus nodules
- subacute invasive aspergillosis
- some other chronic or invasive forms of Aspergillus lung infection
The tests sometimes overlap, but the emphasis is different. That is why it makes sense to keep infection diagnostics and immune or allergy diagnostics in separate articles.
Why diagnosing Aspergillus infection can be difficult
Diagnosing Aspergillus infection is rarely as simple as doing one test and getting a definite yes-or-no answer.
There are several reasons for this:
- Aspergillus is common in the environment, so finding it in a sample does not always mean it is causing illness.
- Symptoms such as cough, tiredness, weight loss, sputum production, breathlessness, and coughing up blood are not specific to aspergillosis.
- Lung changes seen on scans, such as cavities or nodules, can have many possible causes, including prior tuberculosis, non-tuberculous mycobacterial disease, bacterial infection, inflammatory disease, or cancer.
- Some tests detect the body’s immune response, but immune responses vary greatly between patients.
- Some patients are immunosuppressed, which means they may not generate the “expected” test result even when infection is present.
Because of all this, diagnosis usually depends on weighing several pieces of evidence together.
How doctors put the picture together
Doctors usually build the diagnosis from four broad types of information:
1. Symptoms and history
They ask what symptoms are present, how long they have been there, whether they are getting worse, and whether the patient has underlying lung disease or risk factors such as a weakened immune system.
2. Imaging
A computed tomography (CT) scan gives detailed pictures of the lungs and is often central to diagnosis.
3. Lung samples
Sputum, bronchoscopy samples, or sometimes tissue samples may be tested to look for Aspergillus directly.
4. Blood tests
These may look for antibodies, fungal markers, or other evidence supporting infection.
The more these different pieces line up, the more confident the diagnosis becomes.
Computed tomography (CT) scans
A computed tomography (CT) scan is one of the most important tools in diagnosing Aspergillus infection. It shows far more detail than a standard chest X-ray and can reveal patterns that raise suspicion of specific forms of aspergillosis.
A CT scan may show:
- lung cavities
- a fungal ball within a cavity
- nodules
- areas of scarring
- thickened airway walls
- bronchiectasis
- features suggesting chronic inflammation or progressive damage
A scan is extremely useful, but it cannot by itself prove that Aspergillus is the cause. A cavity, for example, may have been caused by another disease and then secondarily colonised by Aspergillus. That is why the scan has to be interpreted alongside the rest of the evidence.
Samples from the lungs
Whenever possible, doctors prefer to test material coming from the lungs themselves.
This may include:
- sputum coughed up by the patient
- bronchoalveolar lavage (BAL) fluid collected during bronchoscopy
- occasionally a tissue biopsy
A bronchoscopy involves passing a thin flexible camera into the airways. This allows doctors to look inside the bronchial tree and to wash a small area with sterile fluid, which is then collected for testing. These samples may give clearer information than blood tests alone because they come from the site where infection may be happening.
Fungal culture
Fungal culture means trying to grow Aspergillus from sputum, BAL fluid, or another sample in the laboratory.
This can be helpful because it may:
- show that live fungus is present
- identify the Aspergillus species
- allow antifungal susceptibility testing to look for resistance
However, culture also has important weaknesses. Aspergillus can be hard to grow, and culture may be negative even when infection is genuinely present. So a negative culture does not rule out disease.
Polymerase chain reaction (PCR) testing
Polymerase chain reaction (PCR) looks for Aspergillus genetic material. Instead of trying to grow the fungus, it asks whether fungal DNA is present in the sample.
PCR can often be faster and more sensitive than culture. It may detect Aspergillus when culture is negative.
But PCR has its own limitations:
- it may detect very small amounts of fungal DNA
- it may detect dead fungal material rather than active growth
- it does not always clearly distinguish colonisation from infection
So PCR is a very useful tool, but it still needs clinical interpretation.
Antigen tests
Antigen tests look for molecules that come from the fungus itself. This is an important step toward more direct diagnosis.
One of the best-known examples is galactomannan, a component of the Aspergillus cell wall. Galactomannan can sometimes be measured in:
- bronchoalveolar lavage (BAL) fluid
- blood, especially in certain invasive settings
Another test, beta-D-glucan, measures a fungal cell wall component found in many fungi. This means it is less specific for Aspergillus, but it can still provide supportive evidence in the right setting.
These tests matter because they aim to detect fungal material rather than waiting for visible growth in the lab.
Blood tests
In chronic forms of aspergillosis, one of the most useful blood tests is Aspergillus immunoglobulin G (IgG).
This test does not detect the fungus directly. Instead, it measures part of the body’s longer-term immune response to Aspergillus. In a patient with the right symptoms and CT scan findings, a raised Aspergillus IgG can strongly support a diagnosis of chronic pulmonary aspergillosis (CPA).
However, blood antibody tests are not perfect:
- some people produce stronger responses than others
- some immunosuppressed patients may not produce much antibody at all
- a positive result still needs to be interpreted with scans and other findings
So Aspergillus IgG is often very helpful, but it is usually one part of the diagnostic puzzle rather than a standalone answer.
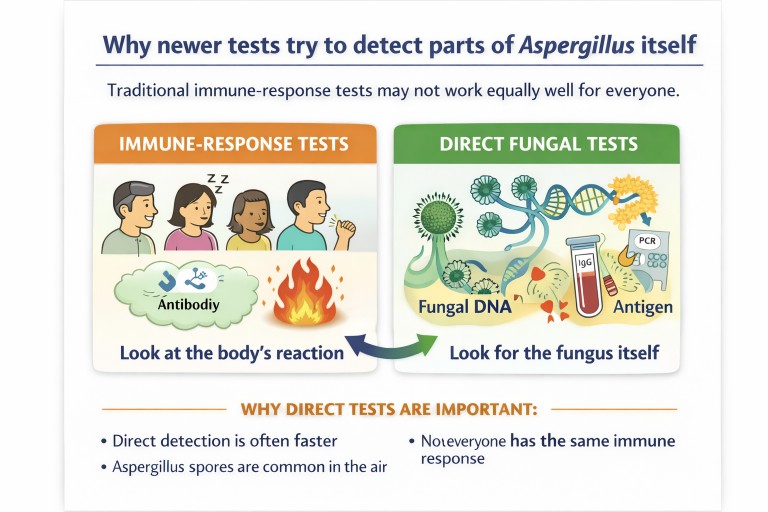
Why try to detect the fungus itself?
This is one of the most important ideas in newer fungal diagnostics.
Many traditional tests look at how the immune system responds to Aspergillus. That can be useful, but it has limitations. Different people respond differently. Some patients mount a strong immune response. Others mount a weak one. Some are too immunosuppressed to produce a strong signal at all.
For that reason, newer tests increasingly try to detect:
- fungal DNA
- fungal cell wall components
- molecules released during fungal growth
- in the future, possibly chemicals in the breath linked to fungal metabolism
These approaches may be closer to direct evidence that the fungus is really present and active.
A simple analogy
Imagine you are trying to work out whether someone has broken into a house.
An immune-response test is a bit like asking the neighbours whether they heard something suspicious. Their answer may help, but it depends on whether they were awake, paying attention, and interpreting the sound correctly.
A direct fungal test is more like finding muddy footprints, fingerprints, or a dropped tool inside the house. It is more direct evidence that the intruder was really there.
In the same way, detecting Aspergillus DNA or fungal cell wall molecules can sometimes tell us more directly that Aspergillus is present than measuring the body’s response alone.
Emerging and future diagnostic tests
Research in fungal diagnostics is moving quite quickly. Several newer approaches are especially promising.
Rapid molecular platforms
These aim to detect fungal DNA more quickly and consistently, sometimes within hours rather than days.
Lateral flow tests
These are simple rapid tests designed to detect fungal molecules in a way that may eventually be practical at or near the point of care.
Next-generation sequencing
This technique can look for genetic material from many organisms at once. In future, it may help make sense of complex infections where Aspergillus is only one part of the picture.
Breath-based tests
Researchers are exploring whether Aspergillus produces distinctive chemicals that can be detected in the breath. If reliable, this could one day provide a much less invasive way to help screen for infection.
Faster resistance detection
As antifungal resistance becomes more important, there is growing interest in tests that can identify resistance markers directly from patient samples rather than waiting for full culture results.
Why several tests are often needed
No single test answers every question.
A CT scan may suggest aspergillosis, but it cannot prove Aspergillus is the cause. A sputum sample may show Aspergillus, but not prove it is causing damage. A blood test may support chronic infection, but not show where the fungus is or whether it is active now.
Doctors therefore usually ask:
- Do the symptoms fit?
- Does the CT scan fit?
- Is Aspergillus detectable in lung samples?
- Do the blood tests support infection?
- Are there better alternative explanations?
Diagnosis is strongest when several lines of evidence point in the same direction.
Common questions patients ask
If Aspergillus is found in my sputum, does that mean I definitely have an infection?
No. Because Aspergillus is common in the environment, it may appear in sputum without being the main cause of illness. Doctors usually need scan findings and other tests as well.
Why can diagnosis take so long?
Some fungal tests take time, especially culture. Also, doctors often need to fit together symptoms, scans, repeat samples, and blood tests before they can be confident.
Why do I need a CT scan if my sputum already showed Aspergillus?
The CT scan helps show whether there is a pattern of lung damage that fits aspergillosis. It helps distinguish simple presence from disease.
Why might I need a bronchoscopy?
A bronchoscopy can obtain better samples directly from the lungs, especially if sputum tests are unclear or if the diagnosis remains uncertain.
Why are newer direct tests so important?
Because they may detect the fungus more directly and more quickly. That could mean earlier diagnosis, more confidence, and better-targeted treatment.
When to seek medical advice
Seek medical advice if you have symptoms such as:
- persistent cough
- worsening breathlessness
- coughing up blood
- unexplained weight loss
- ongoing tiredness with worsening lung symptoms
- recurrent chest infections
- a new cavity, nodule, or unexplained abnormality on lung imaging
This is particularly important if you already have bronchiectasis, chronic obstructive pulmonary disease (COPD), previous tuberculosis, sarcoidosis, or an immune problem.
References
- Denning DW, Cadranel J, Beigelman-Aubry C, Ader F, Chakrabarti A, Blot S, Ullmann AJ, Dimopoulos G, Lange C; European Society for Clinical Microbiology and Infectious Diseases and European Respiratory Society. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J. 2016 Jan;47(1):45-68. doi: 10.1183/13993003.00583-2015. PMID: 26699723.
- Patterson TF, Thompson GR 3rd, Denning DW, Fishman JA, Hadley S, Herbrecht R, Kontoyiannis DP, Marr KA, Morrison VA, Nguyen MH, Segal BH, Steinbach WJ, Stevens DA, Walsh TJ, Wingard JR, Young JA, Bennett JE. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016 Aug 15;63(4):e1-e60. doi: 10.1093/cid/ciw326. Epub 2016 Jun 29. PMID: 27365388; PMCID: PMC4967602.
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015 Mar;70(3):270-7. doi: 10.1136/thoraxjnl-2014-206291. Epub 2014 Oct 29. PMID: 25354514.