Browse information
Latest Articles
Support
For Professionals
Search
omalizumab
Home
Posts Tagged "omalizumab"
omalizumab
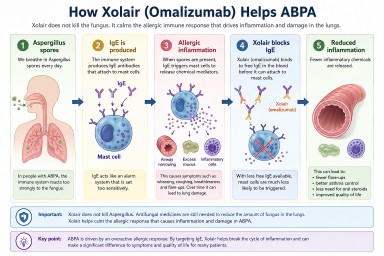
Why Can an Asthma Drug Help ABPA? Understanding Xolair (Omalizumab)
by GAtherton
🌿 Biologics when ABPA and CPA overlap: What Patients Need to Know
Understanding how they work,…
by GAtherton
🌿 ABPA: Infection, Allergy, Biologics, and What It All Means for You
A calm, supportive guide for…
by GAtherton
Omalizumab: how does it help relieve ABPA?
Omalizumab (Xolair) is a…
by GAtherton