Treatment

Exercise and Aspergillosis: How Physical Activity Can Improve Breathing, Strength and Wellbeing
Last reviewed: June 2026 Key…
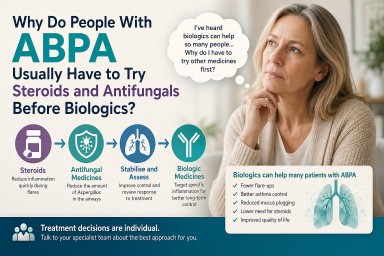
Why Do People With ABPA Usually Have to Try Steroids and Antifungals Before Biologics?
Last reviewed: June 2026…


Last reviewed: June 2026 Key…
Last reviewed: June 2026…