
How to Join Our Microsoft Teams Meetings - Troubleshooting

(For patients, carers and external guests)
You do not need a Microsoft account to join.
Most people can join easily using their internet browser.
✅ The Easiest Way to Join (Laptop or Desktop)
-
Click the meeting link we sent you.
-
When prompted, choose:
“Continue in this browser”
(You do NOT need to download Teams.) -
Type your name.
-
Click Join now.
-
If asked, allow access to your microphone and camera.
Please wait in the lobby until we admit you.
📱 Joining on a Phone or Tablet
-
Tap the meeting link.
-
If you already have the Microsoft Teams app, it will open automatically.
-
If not, you can download the free Teams app from your app store.
-
Enter your name and join.
Phones often work even if laptops have problems.
⚠️ If You Are Asked to Sign In
You do not need to sign into Microsoft.
If you see a sign-in screen:
-
Look for “Join as guest”
-
Or close the page and reopen the link
-
Or choose “Continue in this browser”
Avoid signing in with a work or NHS account unless you are sure it allows external meetings.
🔧 If It Doesn’t Work on Your Laptop
Try one of these:
-
Open the link in a Private / Incognito window
-
Try a different browser (Chrome or Edge usually work best)
-
Make sure you are not already signed into multiple Microsoft accounts
If you are using a work or NHS laptop, security settings may block external meetings. In that case:
👉 Try your personal laptop or your phone.
🎤 Audio & Camera Tips
-
If your microphone does not work, leave the meeting and rejoin.
-
If you prefer, you can turn your camera off.
-
You can also use the chat box to type questions.
📞 Still Having Trouble?
If you cannot join:
-
Try using your phone instead.
-
Or contact us before the meeting and we will help where we can.
Health effects: why aspergillosis patients are higher-risk
This page explains what damp and mould can do to the lungs and how to recognise patterns that suggest your home is contributing to symptoms.
How damp buildings can affect the lungs
Damp homes can increase exposure to airborne particles including fungal spores and fragments. For many people this causes irritation; for people with chronic lung disease it can trigger significant exacerbations.
- Worsening cough, wheeze, breathlessness
- Increased mucus and reduced airway clearance
- More frequent chest infections / antibiotic courses
- Allergic-type reactions in sensitised individuals
Why aspergillosis and severe airways disease are different
If you have Aspergillus-related disease or severe asthma/bronchiectasis, your airways may react strongly to fungal material and irritants. Some patients also require systemic or inhaled corticosteroids, which can increase susceptibility to infections and complicate symptom control.
Important nuance: a damp home does not automatically “cause” aspergillosis, but it can be a powerful driver of persistent symptoms and repeated flares.
Patterns that support a housing contribution
- Time-and-place pattern: symptoms worsen at home and improve when away (even partially).
- Multi-person effects: more than one household member develops respiratory/allergic symptoms.
- Post-disturbance worsening: symptoms worsen after “repairs” or “remediation”.
- Escalating medication use: increased reliever inhaler/nebuliser use, repeated steroid bursts, more antibiotics.
Simple symptom timeline template (copy/paste)
Keeping a short, factual timeline helps clinicians and councils understand risk.
Date(s): Where damp/mould is present: What changed (rain event, leak, repair work, return after decant): Symptoms (breathlessness/wheeze/cough/fever/skin/eyes/nose): Medication change (inhalers, steroids, antibiotics): Healthcare use (GP/A&E/hospital): Improves when away from home? (yes/no, how quickly):
What to ask your clinician to document
- Diagnosis (e.g., Chronic pulmonary aspergillosis, allergic bronchopulmonary aspergillosis, asthma, bronchiectasis)
- That symptoms are consistent with environmental triggers or worsened by damp/mould exposure (they do not need to prove causation)
- Any vulnerability factors (steroid use, immunosuppression, reduced lung function)
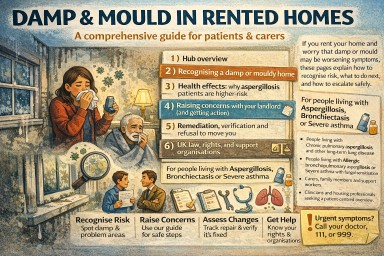
Damp, mould and aspergillosis in rented homes (UK)
A comprehensive guide for patients and carers. If you rent your home and worry that damp or mould may be worsening symptoms, these pages explain how to recognise risk, what to do next, and how to escalate safely.
Who this guide is for
- People living with Chronic pulmonary aspergillosis and other long-term lung disease.
- People living with Allergic bronchopulmonary aspergillosis or Severe asthma with fungal sensitisation.
- Carers, family members, and support workers.
- Clinicians and housing professionals seeking a patient-centred overview.
The key message
A damp home does not automatically cause aspergillosis. However, damp and mould can:
- worsen airway inflammation and symptoms
- trigger exacerbations in asthma/bronchiectasis
- increase allergic-type reactions in sensitised people
- make it harder to stabilise symptoms even with optimal treatment
This hub focuses on practical steps: recognising risk early, communicating effectively, understanding remediation quality, and using UK escalation routes.
How to use this hub
- Start with Recognising a damp home to build an evidence base.
- Read Health effects to understand patterns that support an environmental contribution.
- Use Landlord communications to push for a safe plan, not cosmetic fixes.
- Check Remediation & refusal to move if you’re being pressured to return.
- Use Law & support for UK rights and escalation routes.
Important safety note
If you have severe breathlessness, chest tightness, wheeze, or features of anaphylaxis (for example lip/tongue swelling, throat tightness, collapse), seek urgent medical help. If you are repeatedly attending A&E with symptoms that seem worse at home, tell clinicians you are concerned about damp/mould exposure.
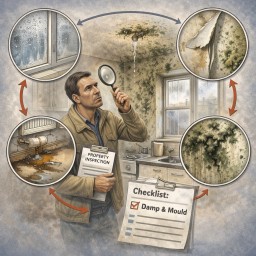
Recognising a damp or mouldy home
Many high-risk exposures occur before mould is obvious. This page helps you identify early signs and start documenting evidence.
Early warning signs (often missed)
- Condensation on windows most mornings
- Cold, clammy walls or cupboards; wardrobes that feel “damp”
- Persistent musty odour (especially when returning home)
- Peeling wallpaper, bubbling paint, cracking plaster
- Recurring black staining on silicone/grout
- Swollen skirting boards, warped flooring, rusting fittings
High-risk hidden locations
- Behind wardrobes/sofas on external walls
- Inside cupboards on outside walls
- Under sinks, behind washing machines, around toilets/baths
- Window reveals, behind curtains/blinds
- Loft hatches and boxed-in pipework
Common causes (useful when speaking to landlords)
- Water ingress (doors/windows, defective seals, roof, gutters, downpipes)
- Plumbing leaks (slow leaks behind walls or under floors)
- Ventilation failures (broken/weak extract fans, blocked vents)
- Cold bridging and persistent condensation in poorly insulated areas
- Previous flooding/leaks with inadequate drying
Quick evidence checklist (10 minutes)
- Take dated photos of any mould, staining, peeling paint, wet patches.
- Photograph likely sources: door thresholds, window seals, gutters if visible, extractor fans, vents.
- Write down where the smell is strongest and when it’s worst (after rain, in winter, after showers).
- Start a brief symptom note (see Page 3) and keep everything in one folder.
- Report the issue in writing to your landlord/agent and keep screenshots/confirmation.
What not to do (for safety)
- Do not scrape or disturb mouldy plasterboard or insulation yourself.
- Do not rely on bleach-only cleaning as a “solution” (it may not address underlying moisture or embedded contamination).
- Do not accept repeated “paint over and close the ticket” approaches without a cause-and-fix plan.

Your rights, the law, and UK support organisations
Key legal frameworks (plain English)
- Fitness for human habitation: rented homes must be safe and fit to live in. Damp and mould can make a home unfit.
- Local council enforcement: councils can inspect and require action where hazards exist (including damp and mould).
- Social housing (England): stronger timeframes and duties apply for significant damp/mould hazards.
Note: housing law differs across England, Scotland, Wales, and Northern Ireland. Health risks are consistent UK-wide, but escalation routes can vary by nation.
Escalation pathway (practical)
- Landlord/agent (in writing): report damp/mould + request an evidence-based plan (Page 4 templates).
- Formal complaint: ask for escalation to stage 2 / senior review.
- Environmental Health (local council): request inspection for damp/mould hazards if unresolved.
- Ombudsman/regulator route: for social housing complaints after internal process.
- Independent housing advice: Shelter or Citizens Advice can help with wording and next steps.
UK support organisations (start here)
- Shelter (England) — housing rights and escalation support.
- Shelter Scotland
- Shelter Cymru (Wales)
- Housing Rights (Northern Ireland)
- Citizens Advice — practical support and signposting.
- Housing Ombudsman — complaints for social housing providers (after the landlord complaints process).
What you do not need to prove
- You do not need a blood test “proving mould exposure”.
- You do not need to name a specific fungal species.
- You do not need the landlord’s contractor to agree with you.
What matters is credible evidence of a hazard plus a plausible link to health deterioration (especially with clinically vulnerable occupants).
Suggested “resources” box for this hub
These are authoritative starting points you can list at the end of each page (optional):
- UK Government: Damp and mould — health risks and guidance
- UK Government: Awaab’s Law guidance (England, social rented sector)
- UK Government: Fitness for Human Habitation — tenant guide
- UK Parliament: Damp and mould — tenant briefing (England)
- Housing Ombudsman: Damp and mould spotlight report
- Asthma + Lung UK (health advice and support)

Remediation, verification, and refusal to move you
If remediation is done but symptoms persist or worsen, the key question becomes: has the home been demonstrated to be safe to occupy?
What “good remediation” should include
- Cause fixed: leak/ingress/defect repaired, not just cleaned.
- Drying: adequate drying time and moisture checks.
- Material decisions: water-damaged porous materials removed where needed.
- Safe work: dust/spore spread controlled (important for medically vulnerable households).
- Verification: documented checks that work is complete and the home is safe.
Red flags (“bad remediation”)
- Paint over staining or “mould spray” only
- No drying plan, no moisture measurements
- No documentation of what was removed/replaced
- Work that creates dust without protection/containment
- Refusal to provide any meaningful post-remediation checks
If symptoms worsen after remediation
Worsening symptoms can occur if contaminated materials were disturbed or if damp persists behind walls/floors. This is a strong indicator that the hazard may not be resolved.
Actions:
- Document symptoms and healthcare visits (Page 3 template).
- Ask landlord for written evidence of safety and remediation details.
- Request escalation to Environmental Health if unresolved.
If the landlord refuses to move you (decant)
Use this framing:
- The issue is not “repairs completed” — it is safety and health risk.
- Ask: “What evidence shows the home is safe to occupy?”
Template request for temporary alternative accommodation
Subject: Request for temporary alternative accommodation (health risk / damp and mould) Hello [Name/Team], Despite remediation work, we are experiencing ongoing damp/mould concerns and worsening health symptoms in a clinically vulnerable household. Please provide written evidence that the home is safe to occupy, including: - confirmation the moisture source has been resolved, - evidence of drying/moisture checks, - what materials were removed/replaced, - what post-remediation checks were completed. Given the uncertainty around safety and the health impacts, we are requesting temporary alternative accommodation until the property can be demonstrated to be safe to occupy. Kind regards, [Name]
If you return “under protest”
If you have no alternative but to return, keep it in writing:
We are returning to the property due to lack of alternative accommodation. We do not accept that the damp/mould hazard has been resolved and will continue to document health impacts and seek independent assessment.
How to raise damp and mould with your landlord (and get action)
Your aim is to secure a safe, evidence-based plan: fix the cause, dry properly, remediate safely, and confirm the home is safe to occupy.
Principles that prevent “cosmetic fixes”
- Source control: stop the leak/ingress/defect.
- Drying: dry building fabric, not just the air.
- Safe remediation: remove/clean contaminated materials appropriately.
- Verification: show the home is safe to occupy.
How to report effectively
- Report in writing (email/portal) and keep everything.
- Attach dated photos and a brief symptom timeline.
- Use health-focused language: “damp and mould hazard”, “medical vulnerability”, “safe to occupy”.
- Ask for timescales, named contact, and written findings.
Template email (copy/paste)
Subject: Damp and mould hazard – urgent investigation and repair plan (health impact) Hello [Landlord/Housing Officer/Letting Agent], I am reporting ongoing damp and/or mould at [address], affecting [rooms/locations]. This has been present since [date] and appears linked to [water ingress/leak/condensation/ventilation failure]. We have clinically vulnerable occupants in the household, including [brief: chronic lung disease / aspergillosis / severe asthma / bronchiectasis], and symptoms are worsening. Please confirm in writing: 1) the inspection date and who will attend, 2) the findings (including likely cause), 3) the repair and drying plan (including timeframes), 4) what remediation will be undertaken (not just surface cleaning/painting), 5) how you will confirm the property is safe to occupy once works are completed. Thank you, [Name] [Phone]
If you are told it is “lifestyle” or “just condensation”
You can reply calmly:
Thank you. We are doing reasonable ventilation and heating measures. However, the pattern and location suggest a building/ventilation defect that requires investigation and repair. Given medical vulnerability in the household, we need a written plan that addresses the underlying cause and confirms the home is safe to occupy.
When to escalate early
- Repeated failed repairs, or mould returns quickly
- Visible mould plus long-term damp patches
- Health deterioration, repeated GP/A&E attendances
- Pressure to accept repainting/bleach-only cleaning
See Page 6 for UK escalation routes and support organisations.
Trials, systematic reviews, and state-of-the-science reviews from ~2016–2026 on damp housing, mould, and health
Executive summary (what 10 years of evidence consistently shows)
1) Damp and mouldy housing is a causal driver of respiratory disease
-
Strong, repeated associations with asthma incidence, asthma exacerbations, wheeze, chronic cough, and poorer lung function, especially in children.
-
Effects persist across countries, climates, and housing systems.
-
Evidence is strongest for asthma and allergic respiratory disease, but extends to bronchitis, infections, and symptom burden in people with existing lung disease.
2) Health effects are dose-related, not binary
-
Risk increases with extent, persistence, and visibility of dampness/mould (patch size, odour, condensation, repeated water damage).
-
No safe threshold has been identified → “any dampness matters.”
3) Mental health impacts are now well-established
-
Damp and mould exposure is associated with depression, anxiety, stress, sleep disturbance, and reduced wellbeing.
-
Pathways are both biological (inflammation, immune activation) and psychosocial (lack of control, stigma, housing insecurity).
4) Children are disproportionately affected
-
Strong paediatric evidence links damp homes to asthma development, poorer asthma control, and higher healthcare use.
-
Early-life exposure appears particularly important.
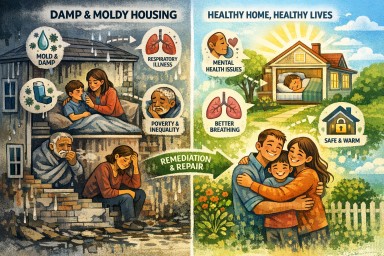
5) Damp housing is a marker of structural inequality
-
Concentrated in low-income, overcrowded, poorly maintained, or privately rented housing.
-
Acts as a health inequality amplifier, not just an environmental exposure.
6) Remediation works—but prevention works better
-
Interventions that fix the building (leaks, insulation, ventilation) improve symptoms.
-
Education alone is insufficient if the housing defect remains.
Thematic synthesis of the literature
1. Respiratory health (strongest evidence base)
Consistent findings across reviews (2016–2025):
-
Dampness and mould exposure increases:
-
Asthma onset in children
-
Asthma severity and exacerbations
-
Wheeze, cough, breathlessness
-
-
Associations hold even after adjusting for smoking, socioeconomic status, and outdoor pollution.
Key insight
Damp housing is not merely an “asthma trigger” — it is a risk factor for developing disease, especially in childhood.
2. Childhood lung health (very strong, clinically relevant)
-
Paediatric reviews emphasise that clinicians routinely see children whose symptoms are driven or sustained by housing conditions.
-
Poor housing undermines:
-
Controller medication effectiveness
-
Self-management plans
-
Long-term lung development
-
Clinical implication
Asking about housing conditions should be as routine as asking about pets or smoking in paediatric respiratory clinics.
3. Mental health and wellbeing (rapidly strengthening evidence)
Recent state-of-the-science reviews conclude:
-
Damp and mould exposure is associated with:
-
Depression
-
Anxiety
-
Psychological distress
-
-
Effects persist even when respiratory disease is accounted for.
Mechanisms proposed
-
Chronic inflammation and immune signalling
-
Sleep disruption
-
Loss of control and “housing stress”
-
Fear for children’s health
Important shift
Damp housing is no longer viewed as purely a respiratory issue—it is a whole-person health exposure.
4. Measurement and exposure assessment (important but imperfect)
What works reasonably well
-
Visual inspection and standard dampness indices
-
Structured questionnaires (especially for asthma cohorts)
-
ERMI (Environmental Relative Moldiness Index) as a research tool
What does NOT yet exist
-
A clinically agreed safe exposure threshold
-
A single test that rules exposure in or out
Consensus
Absence of a perfect test does not mean absence of harm.
5. Built environment, ventilation, and remediation
Clinical trials and housing intervention studies show:
-
Improved ventilation and moisture control:
-
Reduces indoor humidity
-
Improves reported physical and mental health
-
-
Poorly executed energy efficiency measures can worsen damp if ventilation is not addressed.
Critical point
“Warmth without ventilation” is a known failure mode.
6. Housing as a social determinant of health
Major public health frameworks now explicitly define healthy housing as:
-
Warm
-
Dry
-
Well-ventilated
-
Free from mould and toxins
-
Secure and accessible
Shift in framing
Damp housing is not an individual lifestyle issue—it is a system-level health determinant.
What the evidence does not support (important for countering misinformation)
-
No convincing evidence that:
-
“Detox” supplements treat mould exposure
-
Binding agents reverse health effects
-
Genetic susceptibility alone explains illness without exposure
-
-
Evidence strongly favours environmental remediation, not biomedical “workarounds”.
Implications for practice, policy, and patient support
For clinicians
-
Ask about damp and mould explicitly.
-
Document housing conditions when symptoms are unexplained or refractory.
-
Support patients with letters or reports—this is evidence-based advocacy, not speculation.
For public health & housing services
-
Damp housing remediation is preventive medicine.
-
Children’s respiratory health and mental health outcomes justify investment.
For patients
-
Symptoms are not imagined.
-
The problem is the building, not personal failure.
-
Improvement often requires structural change, not just treatment escalation.
Bottom line (10-year consensus)
Damp and mouldy housing causes avoidable disease, worsens inequality, and undermines medical care.
Fixing homes is one of the most effective—and underused—public health interventions available.
References
-
Bentley R, Mason K, Jacobs D, Blakely T, Howden-Chapman P, Li A, Adamkiewicz G, Reeves A.
Housing as a social determinant of health: a contemporary framework. Lancet Public Health. 2025;10(10):e855–e864. doi:10.1016/S2468-2667(25)00142-2. PMID: 40953578. -
Moorcroft C, Whitehouse A, Grigg J.
Damp and mouldy home: impact on lung health in childhood. Archives of Disease in Childhood. 2025;110(6):419–421. doi:10.1136/archdischild-2023-326035. PMID: 39814530. -
Gatto MR, Mansour A, Li A, Bentley R.
A state-of-the-science review of the effect of damp- and mold-affected housing on mental health. Environmental Health Perspectives. 2024;132(8):086001. doi:10.1289/EHP14341. PMID: 39162373. -
Patti MA, Henderson NB, Phipatanakul W, Jackson-Browne M.
Recommendations for clinicians to combat environmental disparities in pediatric asthma. Chest. 2024;166(6):1309–1318. doi:10.1016/j.chest.2024.07.143. PMID: 39059578. -
Punyadasa D, Adderley NJ, Rudge G, Nagakumar P, Haroon S.
Self-reported questionnaires to assess indoor home environmental exposures in asthma patients: a scoping review. BMC Public Health. 2024;24:2915. doi:10.1186/s12889-024-20418-8. PMID: 39434085. -
Kozajda A, Miśkiewicz E.
Exposure to bioaerosol in the residential environment. Medycyna Pracy. 2024;75(6):545–560. doi:10.13075/mp.5893.01508. PMID: 39688367. -
Vesper SJ.
The development and application of the Environmental Relative Moldiness Index (ERMI). Critical Reviews in Microbiology. 2025;51(2):285–295. doi:10.1080/1040841X.2024.2344112. PMID: 38651788. -
Nabaweesi R, Hanna M, Muthuka JK, Samuels AD, Brown V, Schwartz D, Ekadi G.
The built environment as a social determinant of health. Primary Care. 2023;50(4):591–599. doi:10.1016/j.pop.2023.04.012. PMID: 37866833. -
Grant TL, Wood RA.
The influence of urban exposures and residence on childhood asthma. Pediatric Allergy and Immunology. 2022;33(5):e13784. doi:10.1111/pai.13784. PMID: 35616896. -
Coulburn L, Miller W.
Prevalence, risk factors and impacts related to mould-affected housing: an Australian integrative review. International Journal of Environmental Research and Public Health. 2022;19(3):1854. doi:10.3390/ijerph19031854. PMID: 35162876. -
Wimalasena NN, Chang-Richards A, Wang KI, Dirks KN.
Housing risk factors associated with respiratory disease: a systematic review. International Journal of Environmental Research and Public Health. 2021;18(6):2815. doi:10.3390/ijerph18062815. PMID: 33802036. -
Ali SH, Foster T, Hall NL.
The relationship between infectious diseases and housing maintenance in Indigenous Australian households. International Journal of Environmental Research and Public Health. 2018;15(12):2827. doi:10.3390/ijerph15122827. PMID: 30545014. -
Wolkoff P.
Indoor air humidity, air quality, and health – an overview. International Journal of Hygiene and Environmental Health. 2018;221(3):376–390. doi:10.1016/j.ijheh.2018.01.015. PMID: 29398406. -
Mendell MJ, Kumagai K.
Observation-based metrics for residential dampness and mold with dose–response relationships to health: a review. Indoor Air. 2017;27(3):506–517. doi:10.1111/ina.12342. PMID: 27663473. -
Francisco PW, Jacobs DE, Targos L, Dixon SL, Breysse J, Rose W, Cali S.
Ventilation, indoor air quality, and health in homes undergoing weatherization: a randomized trial. Indoor Air. 2017;27(2):463–477. doi:10.1111/ina.12325. PMID: 27490066. -
Barnes CS, Horner WE, Kennedy K, Grimes C, Miller JD.
Home assessment and remediation. Journal of Allergy and Clinical Immunology: In Practice. 2016;4(3):423–431.e15. doi:10.1016/j.jaip.2016.01.006. PMID: 27157934. -
Chew GL, Horner WE, Kennedy K, Grimes C, Barnes CS, Phipatanakul W, Larenas-Linnemann D, Miller JD.
Procedures to assist health care providers to determine when home assessments for potential mold exposure are warranted. Journal of Allergy and Clinical Immunology: In Practice. 2016;4(3):417–422.e2. doi:10.1016/j.jaip.2016.01.013. PMID: 27021632. -
Vesper S, Wymer L.
The relationship between Environmental Relative Moldiness Index values and asthma. International Journal of Hygiene and Environmental Health. 2016;219(3):233–238. doi:10.1016/j.ijheh.2016.01.006. PMID: 26861576.
Invitation: Patient & Carer Discussion on Living with ABPA. New type of treatment.
🕙 10:00am, Thursday 12th
Get details on how to join us by clicking on the link below and choosing Thursday 12th Patients Support Meeting - you will be sent a link to the meeting via email.
https://outlook.office.com/book/[email protected]/
We are inviting people living with Allergic Bronchopulmonary Aspergillosis (ABPA), and those who care for them, to take part in an open, informal online discussion with argenx, a research-focused biotechnology company.
argenx would like to listen directly to patients and carers to better understand what day-to-day life with ABPA is really like. There is no need to prepare anything in advance — you are welcome simply to listen, or to share as much or as little as you feel comfortable.
They are particularly interested in hearing about:
-
Patients’ and carers’ journeys living with ABPA
-
Which symptoms are most burdensome in everyday life (for example breathlessness, cough, fatigue, thick mucus or mucus plugs)
-
Where current treatments fall short from a patient or carer perspective
-
What would make patients or carers feel motivated or reassured about taking part in a future clinical trial of a new ABPA therapy
The purpose of this conversation is to help researchers design future studies that reflect what matters most to patients, including which outcomes are meaningful and how trials can be made more patient-friendly.
📅 Date: Thursday 12th
🕙 Time: 10:00am
💬 Format: Open, informal discussion
📝 Preparation: None required
If you are living with ABPA, or care for someone who is, and would be interested in attending, please let us know.
A short explainer: what is ARGX-118?
argenx is developing an investigational (research-stage) treatment called ARGX-118. It is not yet a licensed medicine and is not currently available outside of research studies.
In ABPA, many people experience very thick, sticky mucus and mucus plugs that block airways and contribute to breathlessness, cough, and flare-ups. Research has shown that this mucus can sometimes contain microscopic crystals formed from proteins released by certain white blood cells involved in allergic inflammation. These crystals can make mucus denser and harder to clear.
ARGX-118 is designed to target and break down these crystals, with the aim of making mucus less thick and easier to clear from the lungs. This is a different approach from current treatments, which mainly focus on suppressing inflammation (such as steroids or biologics) or reducing fungal burden (antifungal medicines).
Because ARGX-118 is still in early development, we do not yet know how effective it will be, who might benefit most, or how it would fit alongside existing treatments. That is exactly why argenx wants to hear from patients and carers now — to understand real-world symptoms, treatment gaps, and what would genuinely matter if a future clinical trial were developed.
👉 Attending this meeting does not commit you to any trial and will not affect your care. It is simply an opportunity to share experiences and help shape future research, if you wish.
Systemic fungal infections: why speed, diagnosis and stewardship matter
Systemic fungal infections — including aspergillosis, candidiasis, cryptococcosis, mucormycosis and pneumocystis pneumonia — are medical emergencies. When diagnosis or treatment is delayed, mortality rises sharply. This comprehensive review brings together current understanding of how these infections arise, why they are so difficult to diagnose, and what is needed to improve outcomes.
Why fungal infections are often missed
Unlike many bacterial infections, systemic fungal infections can be hard to confirm quickly. Fungal organisms are often present in low numbers, may be released intermittently into the bloodstream, and can be difficult to grow in standard cultures. As a result, no single test is usually sufficient, and clinicians often need a combination of imaging, cultures, antigen tests, molecular tests (PCR), and histopathology.
Because delay can be fatal, antifungal treatment is frequently started on clinical suspicion alone — especially in critically ill or immunocompromised patients. The paper emphasises that this approach is often necessary, but it must be paired with a clear diagnostic strategy.
Antifungal stewardship: knowing when to stop
A central message of the paper is that diagnostic tests are just as important for stopping treatment as for starting it. Antifungal drugs can be toxic, interact with many other medicines, and drive antifungal resistance if used unnecessarily.
The authors stress that:
-
Diagnostic results should be actively reviewed
-
Antifungal therapy should be stopped or stepped down if infection is not supported by evidence
-
This approach protects patients and preserves antifungal effectiveness
Antifungal resistance is a growing threat
Antifungal resistance is no longer rare. The review highlights:
-
Azole resistance in Aspergillus, including cryptic species
-
Rising resistance in several Candida species
-
The global spread of multidrug-resistant Candida auris
Because of this, the authors recommend that all clinically relevant fungal isolates are identified to species level and tested for antifungal susceptibility wherever possible. Making assumptions about drug sensitivity is increasingly unsafe.
Aspergillosis: a broad spectrum of disease
The paper clearly outlines the many forms of aspergillosis, ranging from:
-
Allergic disease (such as allergic bronchopulmonary aspergillosis)
-
Chronic pulmonary aspergillosis, often in people with underlying lung damage
-
Subacute and acute invasive disease, particularly in immunocompromised or critically ill patients
Importantly, the review notes that aspergillosis is not limited to severely immunocompromised people. Chronic and subacute forms often occur in individuals with structural lung disease who are otherwise immunocompetent.
Climate change and emerging fungal risks
One of the most forward-looking sections of the paper addresses how climate change and natural disasters are altering fungal disease patterns. Rising environmental temperatures, flooding, storms and environmental disruption are:
-
Increasing exposure to environmental fungi
-
Enabling fungi to adapt to higher temperatures
-
Contributing to outbreaks after natural disasters and trauma
-
Expanding fungal diseases into new geographic regions
The authors argue that fungal infections must be considered part of future public health and healthcare resilience planning.
Key take-home messages
-
Systemic fungal infections are time-critical medical emergencies
-
Diagnosis usually requires multiple tests, not a single result
-
Early antifungal treatment is often necessary — but must be reviewed
-
Diagnostics are essential for safe antifungal stewardship
-
Antifungal resistance is a real and growing problem
-
Climate change is reshaping fungal epidemiology and risk
Free access to the full article
Elsevier has provided free access to the full paper for a limited time (no registration required):
👉 https://authors.elsevier.com/a/1mZqR4qdNoJLH2
🗓️ Available until 28 March 2026
This article is recommended reading for patients wanting a deeper understanding of fungal disease, as well as clinicians, microbiology teams, and healthcare planners.