Travelling with Aspergillosis: A Comprehensive Guide to Safe and Stable Travel
This guide is for people living with:
- Chronic Pulmonary Aspergillosis (CPA)
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Severe asthma (including fungal sensitisation)
- Bronchiectasis
- Fibrotic or structurally abnormal lung disease
Most people with stable disease can travel successfully. The goal is not restriction — it is risk reduction through preparation, environmental awareness, and early action if symptoms change.
Contents
- 1. Understanding Travel Risk in Aspergillosis
- 2. Coordinating With Your Medical Team
- 3. Assessing Stability Before Travel
- 4. Choosing a Destination: Environmental Determinants
- 5. Regional Risk Patterns Explained
- 6. Air Pollution & AQI Monitoring
- 7. Heat, Humidity & Hydration Physiology
- 8. Travel Insurance & Disclosure
- 9. Medication Planning & Contingency Prescriptions
- 10. Specific Considerations for Azole Antifungals
- 11. Air Travel: Physiology & Fit-to-Fly
- 12. Cabin Dryness & Post-Flight Irritation
- 13. Travelling with Oxygen
- 14. Accommodation Risk Reduction
- 15. High-Spore & Dust Exposure Environments
- 16. Infection Prevention
- 17. Haemoptysis Planning
- 18. Red Flag Symptoms
- 19. Advanced Planning Checklist
1. Understanding Travel Risk in Aspergillosis
Travel risk arises from four domains:
- Structural lung vulnerability (cavities, fibrosis, bronchiectasis)
- Inflammatory instability (ABPA activity, asthma control)
- Environmental exposure (humidity, dust, pollution)
- Healthcare accessibility (if deterioration occurs)
Travel is usually safe when disease is stable and exposures are predictable.
2. Coordinating With Your Medical Team
Respiratory Clinic
- Review recent imaging (particularly in CPA)
- Assess haemoptysis history
- Consider fit-to-fly testing if oxygen saturation borderline
- Discuss standby rescue medication
GP
- Ensure medication supply exceeds travel duration
- Provide updated medication summary
- Support vaccination review
- Assist with insurance documentation
3. Assessing Stability Before Travel
Delay travel if within 4–6 weeks of:
- Significant haemoptysis
- Escalating breathlessness
- Recent hospital admission
- New antifungal initiation
Stable inflammatory markers and symptom plateau are reassuring.
4. Choosing a Destination: Environmental Determinants
Key determinants:
- Humidity: promotes indoor mould growth
- Flood history: water damage increases fungal load
- Air pollution: triggers bronchospasm
- Dust burden: irritates inflamed airways
- Healthcare infrastructure: safety net if unwell
5. Regional Risk Patterns Explained
Lower Overall Respiratory Stress
- Scandinavia
- New Zealand
- Canada (outside wildfire season)
Cooler climates limit mould growth; strong building codes reduce damp housing.
Moderate Risk
- Mediterranean Europe
Generally safe when stable; monitor wildfire smoke and heat stress.
Higher Respiratory Stress
- Tropical monsoon climates
- Flood-prone regions
- Highly polluted megacities
- Dust storm zones
Humidity increases fungal proliferation; particulate pollution worsens airway inflammation.
6. Air Pollution & AQI Monitoring
Air pollution can exacerbate cough, bronchospasm, breathlessness and fatigue in people with chronic lung disease. In some urban environments, pollution may pose a greater day-to-day risk than fungal exposure.
The most widely used measure of air quality is the Air Quality Index (AQI), which combines several pollutants into a single score.
Key Pollutants That Matter in Lung Disease
- PM2.5 – fine particulate matter small enough to penetrate deep into the lungs
- PM10 – larger inhalable particles
- Ozone (O₃) – irritates airways, especially in heat
- Nitrogen dioxide (NO₂) – associated with traffic pollution
PM2.5 is particularly important in aspergillosis and severe asthma because it can:
- Trigger airway inflammation
- Increase mucus production
- Worsen bronchospasm
- Reduce exercise tolerance
Reliable Air Quality Monitoring Resources
These sites provide real-time data and forecasts:
- World Air Quality Index (WAQI)
https://waqi.info
Interactive global map with live AQI data for cities worldwide. - IQAir (AirVisual)
https://www.iqair.com
Detailed pollutant breakdowns, 7-day forecasts and wildfire smoke tracking. - UK Daily Air Quality Index (DEFRA)
https://uk-air.defra.gov.uk
Official UK monitoring network with health advice bands.
These platforms also offer mobile apps, which are useful for checking conditions while travelling.
How to Interpret AQI in Practical Terms
| AQI | Category | Practical Advice for Lung Conditions |
|---|---|---|
| 0–50 | Good | Ideal conditions for outdoor activity |
| 51–100 | Moderate | Usually safe; monitor symptoms |
| 101–150 | Unhealthy for sensitive groups | Reduce strenuous outdoor activity; consider indoor plans |
| 151–200 | Unhealthy | Limit time outdoors; avoid exertion |
| 200+ | Very Unhealthy/Hazardous | Stay indoors with filtered air if possible |
For many patients with CPA, ABPA or severe asthma, an AQI above 100 warrants caution. Above 150, limiting outdoor exposure is advisable.
Wildfire Smoke
Wildfire smoke contains high concentrations of PM2.5 and organic particulates. Even patients who are stable at home may experience:
- Increased cough
- Chest tightness
- Increased sputum production
- Fatigue
If travelling during wildfire season:
- Check AQI daily
- Plan indoor activities when levels are elevated
- Use air-conditioned or filtered indoor environments
- Carry rescue inhalers
Urban Pollution vs Rural Dust
Urban areas are more affected by traffic-related pollutants (NO₂, PM2.5), while rural or desert areas may present dust exposure. Both can aggravate inflamed airways.
The risk is cumulative. Short exposure is usually tolerated; prolonged high-level exposure increases the likelihood of symptom flare.
Key principle: checking AQI before and during travel is one of the simplest and most effective risk-reduction steps for people with chronic lung disease.
7. Heat, Humidity & Hydration Physiology
Hot climates place additional physiological stress on people with chronic lung disease.
Why Heat Matters
In warm environments, the body increases sweating and respiratory water loss to regulate temperature. This leads to:
- Increased insensible fluid loss (fluid lost through breathing and skin)
- Reduced plasma volume if intake is inadequate
- Thickening of airway secretions
In bronchiectasis and chronic pulmonary aspergillosis (CPA), mucus clearance is already impaired. Dehydration increases mucus viscosity, making sputum:
- Harder to expectorate
- More likely to stagnate in damaged airways
- Potentially more prone to secondary infection
Patients may notice thicker sputum, increased cough, or chest tightness in hot weather.
Humidity: Helpful or Harmful?
Humidity has mixed effects:
- Moderate humidity can help prevent airway drying.
- High humidity can increase environmental mould growth, particularly indoors if ventilation is poor.
In tropical or monsoon climates, poorly ventilated buildings may have higher fungal spore burdens due to damp conditions.
Heat, Fatigue & Breathlessness
Heat increases cardiovascular demand. The heart works harder to dissipate heat, which can:
- Increase perceived breathlessness
- Increase fatigue
- Reduce exercise tolerance
This does not necessarily indicate worsening lung disease — but it can feel similar.
Hydration Strategy
Practical recommendations:
- Begin hydrating the day before travel
- Drink fluids regularly rather than waiting for thirst
- Aim for pale straw-coloured urine
- Increase intake during flights and hot excursions
Limit:
- Excess alcohol (diuretic effect)
- High caffeine intake
Additional Practical Measures
- Plan outdoor activity early morning or evening
- Rest during peak heat (midday)
- Use air-conditioned environments when available
- Continue airway clearance routines while travelling
Key principle: in chronic lung disease, hydration supports mucus clearance and reduces avoidable exacerbation risk during hot weather.
8. Travel Insurance & Full Medical Disclosure
Travel insurance is not a formality — it is a critical safety net for people with chronic lung disease.
When purchasing insurance, you must declare all pre-existing medical conditions. This typically includes:
- Chronic Pulmonary Aspergillosis (CPA)
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Severe asthma
- Bronchiectasis
- Pulmonary fibrosis
- Long-term steroid therapy
- Adrenal insufficiency (if present)
- Oxygen use (even if only occasional)
Why Full Disclosure Matters
If you fail to declare a relevant condition, the insurer may:
- Refuse to cover medical treatment abroad
- Decline repatriation costs
- Refuse to reimburse cancelled flights or accommodation
- Invalidate the entire policy
This applies even if the emergency appears unrelated. Insurers may review your full medical history during a claim.
What Insurers Typically Ask
You may be asked:
- Have you been hospitalised in the past 12 months?
- Have you had medication changes recently?
- Have you had haemoptysis?
- Are you awaiting tests or investigations?
- Are you on long-term steroids?
Answer these questions carefully and honestly.
Policies and Stability
Some insurers will decline cover if:
- You have been hospitalised recently
- You are awaiting investigations
- Your condition is considered unstable
This is another reason to travel during a period of clinical stability.
European Travel (UK Patients)
If travelling within Europe, ensure you carry:
- Your GHIC (Global Health Insurance Card)
However, GHIC does not replace travel insurance. It may not cover:
- Private healthcare
- Mountain rescue
- Repatriation to the UK
Practical Tips
- Purchase insurance as soon as you book travel
- Keep written confirmation of declared conditions
- Carry the insurer’s emergency contact number with you
- Inform the insurer early if you require hospital care abroad
In summary: full disclosure protects you. Insurance is only effective if the insurer understands your medical background from the outset.
9. Medication Planning & Contingency Prescriptions
- Carry 1–2 weeks extra supply
- Bring medications in original packaging
- Carry clinic letter
- Consider written rescue plan
10. Specific Considerations for Azole Antifungals
Azoles have significant drug–drug interactions.
- Inform any clinician abroad you are taking an azole
- Avoid grapefruit
- Be aware of sun sensitivity (voriconazole)
- Take itraconazole with food
11. Air Travel: What Actually Happens in the Cabin?
Commercial aircraft cabins are pressurised to simulate an altitude of approximately 6,000–8,000 feet (1,800–2,400 metres).
This means the partial pressure of oxygen is lower than at sea level. For healthy individuals this causes only a small drop in oxygen saturation (typically 3–4%).
Are Most People with Aspergillosis OK to Fly?
Yes — most stable patients fly without difficulty.
People who are:
- Clinically stable
- Not oxygen-dependent
- Without recent haemoptysis
- With resting oxygen saturations ≥95%
generally tolerate commercial flights well, including medium and long-haul travel.
Many patients report anxiety before their first flight after diagnosis, but in stable disease, significant problems are uncommon.
Who Should Consider Fit-to-Fly Testing?
Assessment may be appropriate if you have:
- Resting oxygen saturation consistently below 95%
- Advanced pulmonary fibrosis
- Extensive cavitation
- Significant breathlessness at minimal exertion
- Recent clinical deterioration
The test commonly used is a Hypoxic Challenge Test (HCT), which simulates cabin oxygen conditions to determine whether supplemental oxygen is required during flight.
Where would I have a Hypoxic Challenge Test (HCT)?
In the UK, a Hypoxic Challenge Test is usually arranged through a hospital respiratory physiology department.
You cannot book this test directly. It must be requested by:
- Your respiratory consultant or clinic, or
- Occasionally your GP (who would refer you to a hospital service)
The test is typically performed in:
- A hospital lung function laboratory
- A respiratory physiology unit
- A specialist respiratory centre
During the test, you breathe a gas mixture containing a lower oxygen concentration (usually around 15%) to simulate aircraft cabin conditions. Your oxygen saturation is monitored continuously. If levels fall below safe thresholds, in-flight oxygen may be recommended.
Do Most People Need This Test?
No. Many stable patients with normal resting oxygen saturation (typically ≥95%) do not require hypoxic challenge testing.
The test is generally considered if you:
- Have resting oxygen saturation below 95%
- Have advanced pulmonary fibrosis
- Are already using oxygen
- Have significant exertional desaturation
If you are unsure, ask your respiratory team whether assessment is appropriate for you.
Symptoms During Flight: What Is Normal?
Mild symptoms that can occur in stable patients include:
- Slight increase in breathlessness on walking the aisle
- Fatigue
- Dry cough (often due to low humidity)
These are usually temporary and not dangerous.
Severe symptoms (marked breathlessness at rest, chest pain, dizziness, confusion) are uncommon and require crew notification.
Anxiety vs Physiological Breathlessness
It is very common for people with chronic lung disease to experience heightened awareness of their breathing during flights. The enclosed environment, reduced cabin pressure and awareness of altitude can all increase anxiety.
Anxiety-related breathlessness typically presents as:
- A sensation of not getting a “satisfying” breath
- Chest tightness without wheeze
- Rapid breathing (hyperventilation)
- Tingling in fingers or lips
- Light-headedness
Hyperventilation lowers carbon dioxide levels in the blood. This can cause dizziness, tingling and a feeling of air hunger — even when oxygen levels are normal.
Physiological hypoxia (true low oxygen levels) is less common in stable patients who have been assessed as fit to fly. When it occurs, it is more likely in those with advanced fibrosis, low baseline oxygen saturations, or recent instability.
Features more suggestive of physiological compromise include:
- Persistent breathlessness at rest
- Worsening cyanosis (bluish lips or fingers)
- Marked fatigue or confusion
- Objective low oxygen saturation if measured
For patients who have undergone fit-to-fly assessment and been cleared to travel, significant in-flight hypoxia is uncommon.
Practical Strategies
- Use slow, paced breathing (e.g. inhale for 4 seconds, exhale for 6 seconds)
- Focus on extended exhalation to reduce hyperventilation
- Keep shoulders relaxed and posture upright
- Avoid repeatedly “checking” your breathing
- Remind yourself that mild symptoms are common and expected
Understanding the difference between anxiety-related breathlessness and true hypoxia can significantly reduce distress during flight.
Deep Vein Thrombosis (DVT) Risk
Chronic lung disease does not automatically increase DVT risk, but long-haul immobility does.
General advice:
- Move legs regularly
- Stay hydrated
- Avoid excess alcohol
12. Cabin Dryness & Post-Flight Airway Irritation
Cabin humidity is typically 10–20% (normal indoor comfort is 40–60%).
Low humidity can:
- Dry airway lining
- Reduce mucociliary clearance
- Thicken secretions
- Trigger cough or mild bronchospasm
This is often why people feel they have “caught a cold” the day after flying. In most cases, it is airway irritation rather than infection.
How to Reduce Dryness Effects
- Hydrate well before and during flight
- Limit alcohol and caffeine
- Use isotonic saline nasal spray
- Continue preventer inhalers
- Keep rescue inhaler accessible
- Avoid direct overhead air vents blowing onto your face
- Consider mask use — masks increase humidity of inhaled air
Symptoms typically settle within 24–48 hours.
When to Seek Advice After Flying
Seek medical advice if you develop:
- Progressively worsening breathlessness
- Persistent fever
- Significant haemoptysis
- Chest pain
In stable patients, serious in-flight deterioration is uncommon.
12. Cabin Dryness & Post-Flight Irritation
Cabin humidity is 10–20%.
Dry air:
- Reduces mucociliary clearance
- Thickens secretions
- Triggers cough
- Irritates airways
Hydration and saline sprays reduce symptoms. Post-flight irritation commonly lasts 24–48 hours and does not necessarily indicate infection.
13. Travelling with Oxygen
Confirm airline device approval and battery duration. Plan well in advance.
14. Accommodation Risk Reduction
Request:
- Hard flooring
- No damp odour
- No renovation dust
- Pet-free rooms
Chains Often Reported as Allergy-Conscious
- Hyatt
- Hilton
- Marriott
- Scandic
- Premier Inn
Newer business hotels often have better HVAC filtration.
15. High-Spore & Dust Exposure Environments
- Compost handling
- Construction sites
- Flood-damaged buildings
- Agricultural dust
Avoid heavy inhalation exposure.
16. Infection Prevention
- Hand hygiene
- Avoid close contact with visibly unwell individuals
- Maintain vaccination schedule
17. Haemoptysis Planning
If you have a history of haemoptysis:
- Know your previous pattern
- Carry clinic contact details
- Seek urgent care if volume increases significantly
18. Red Flag Symptoms
- Increasing breathlessness
- New or worsening haemoptysis
- Persistent fever
- Severe chest pain
19. Advanced Planning Checklist
- Travel when stable
- Plan with GP and respiratory clinic
- Carry documentation
- Monitor AQI
- Hydrate on flights
- Avoid damp & heavy dust
- Know red flags
With preparation, most people with stable aspergillosis travel safely and successfully.

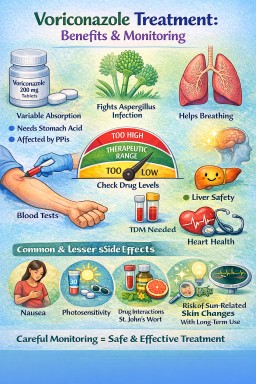
Voriconazole in Aspergillosis
A balanced guide for patients and clinicians
-
Chronic pulmonary aspergillosis (CPA)
-
Allergic bronchopulmonary aspergillosis (ABPA) (selected cases)
-
Invasive aspergillosis
-
Azole-resistant or itraconazole-intolerant cases
It is available orally and intravenously and is often used when a stronger or more reliably absorbed azole is required.
1️⃣ What Voriconazole Does
Voriconazole works by blocking fungal ergosterol synthesis (CYP51 inhibition), which disrupts the fungal cell membrane.
Compared with itraconazole:
-
More potent against Aspergillus
-
More predictable oral absorption
-
More central nervous system penetration
It often produces symptom improvement over weeks, though some effects (e.g. visual symptoms) may occur quickly.
2️⃣ How Long Is Treatment?
In CPA
-
Often 6–12 months or longer
-
Sometimes used as second-line or after intolerance to itraconazole
-
Long-term suppressive therapy may be required
In ABPA
-
Used in selected steroid-dependent or refractory cases
In invasive disease
-
Typically several months depending on response and immune status
3️⃣ Why Blood Level Monitoring Is Essential
Voriconazole has non-linear pharmacokinetics.
Small dose changes can cause large blood level shifts.
Two patients on the same dose may have very different levels due to:
-
Liver metabolism (CYP2C19 genetic variation is important)
-
Drug interactions
-
Age
-
Weight
-
Liver function
If Levels Are Too Low
-
Treatment failure
-
Persistent fungal activity
-
Risk of resistance
If Levels Are Too High
-
Liver toxicity
-
Neurological side effects
-
Visual disturbances
-
Increased interaction risk
Typical Target (Trough)
-
Generally 1–5.5 mg/L (lab dependent)
-
Toxicity risk increases >5–6 mg/L
Levels are usually checked:
-
5–7 days after starting
-
After dose adjustments
-
If side effects occur
-
If clinical response is inadequate
4️⃣ Common Side Effects (Often Mild & Reversible)
Visual Disturbances (Very Common but Usually Harmless)
-
Blurred vision
-
Altered colour perception
-
Light sensitivity
-
“Wavy” vision
These typically:
-
Occur within 30–60 minutes of dosing
-
Last less than an hour
-
Reduce over time
Patients should avoid night driving initially until they understand their response.
Photosensitivity
-
Increased sensitivity to sunlight
-
Sunburn risk
-
Long-term risk of skin damage with prolonged therapy
Sun protection is important.
Gastrointestinal
-
Nausea
-
Abdominal discomfort
5️⃣ Less Common but Important Effects
Neurological
-
Headache
-
Vivid dreams
-
Hallucinations (usually at high levels)
-
Confusion (dose-related)
These are generally reversible with dose adjustment.
Liver Abnormalities
Routine liver function monitoring is required.
Most abnormalities are mild and resolve with dose modification.
Cardiac Effects
Voriconazole can prolong the QT interval.
Caution in patients with:
-
Known arrhythmias
-
Electrolyte imbalance
-
Other QT-prolonging drugs
ECG monitoring may be appropriate in higher-risk patients.
Skin Cancer Risk (Long-Term Use)
With prolonged use (especially >1–2 years):
-
Increased risk of skin squamous cell carcinoma
-
Particularly in transplant recipients
Sun protection and dermatology review are advised for long-term therapy.
6️⃣ Food & Drug Advice
-
Avoid grapefruit
-
Avoid St John’s Wort
-
Take tablets at least 1 hour before or after meals (food reduces absorption)
Voriconazole has many CYP-mediated interactions and requires careful medication review.
7️⃣ Comparison With Itraconazole (Simple Overview)
| Feature | Itraconazole | Voriconazole |
|---|---|---|
| Absorption variability | High | More predictable |
| Visual side effects | Rare | Common but mild |
| Photosensitivity | Rare | More common |
| QT prolongation | Minimal | Possible |
| TDM needed | Yes | Yes (essential) |
Balanced Summary for Patients
Voriconazole is a strong antifungal used when more reliable or potent treatment is needed. Most side effects are manageable and reversible, and blood monitoring keeps treatment safe.
Clinician Checklist
-
Confirm indication and prior azole exposure
-
Check baseline LFTs
-
Review ECG if cardiac risk present
-
Assess drug interactions (CYP2C19, 2C9, 3A4)
-
Arrange trough level at day 5–7
-
Counsel regarding visual symptoms and sun protection
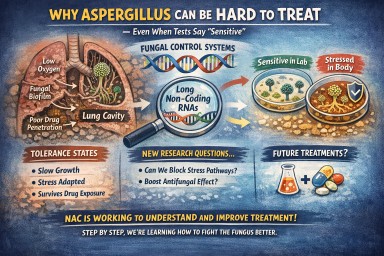
Why Can Aspergillus Infection Be Hard to Clear — Even When Tests Say It’s “Sensitive”?
Many patients ask:
“If my lab report says the fungus is sensitive to the antifungal drug, why is my condition not improving quickly?”
This is a very reasonable question.
The short answer is: fungi are biologically adaptable, and we are still learning how they adjust inside the lung.
Recent research involving scientists working with the National Aspergillosis Centre (NAC), including work led by Dr. Weaver and colleagues, is helping us understand this better.
You can read the scientific abstract here:
🔗 https://pubmed.ncbi.nlm.nih.gov/41673015/
1️⃣ What Does “Sensitive” Mean in the Lab?
When Aspergillus is tested against a drug (such as itraconazole or voriconazole), laboratories measure the minimum inhibitory concentration (MIC).
This tells us the drug level needed to stop fungal growth in a controlled lab setting.
If the MIC is low, the fungus is labelled “sensitive.”
But the laboratory environment is very different from a lung cavity.
2️⃣ The Lung Is Not a Uniform Environment
In chronic pulmonary aspergillosis (CPA), the fungus often lives inside:
-
Cavities
-
Scarred lung tissue
-
Fungal balls
-
Thick mucus
Within these areas there can be:
-
Low oxygen
-
Variable iron levels
-
Uneven drug penetration
-
Different levels of immune activity
This means that different parts of the same infection can behave differently at the same time.
3️⃣ New Research: Fungi Have Fine-Tuned Control Systems
Recent work from researchers collaborating with NAC, including Prof. Bowyer’s group, has shown that Aspergillus contains additional regulatory elements in its genome called long non-coding RNAs (lncRNAs).
These do not make proteins.
Instead, they help fine-tune how nearby genes behave under stress.
In laboratory studies, some of these regulatory elements appear to influence how the fungus responds to antifungal drugs — even when there is no classic resistance mutation.
This suggests:
-
Aspergillus can adjust how strongly certain pathways (like ergosterol production) are activated.
-
These adjustments may help the fungus survive stressful conditions.
-
This survival does not always show up as “resistance” in standard lab testing.
This does not mean the drug does not work.
It means the biological response can be more subtle and layered than we previously understood.
4️⃣ Resistance vs Tolerance — An Important Difference
Resistance
-
Caused by stable genetic mutations.
-
The drug becomes much less effective.
-
MIC levels rise clearly.
Tolerance
-
The fungus survives but grows slowly.
-
MIC may still appear “sensitive.”
-
The fungus adapts temporarily to stress conditions.
The new regulatory findings may help explain tolerance — not necessarily resistance.
5️⃣ Why This Matters for CPA
CPA is a chronic condition.
Inside lung cavities:
-
Drug levels may vary.
-
Oxygen levels fluctuate.
-
Stress signals are ongoing.
This environment encourages survival strategies.
Research like the Weaver study helps us understand why:
-
Treatment response may be gradual.
-
Cultures can be intermittently positive.
-
Stability may be the goal rather than rapid clearance.
6️⃣ How Could This Research Help in the Future?
It is important to be realistic: this research is still at an early stage.
However, understanding these regulatory systems opens new possibilities.
Instead of thinking only about killing the fungus directly, future approaches might aim to:
-
Weaken its survival responses.
-
Reduce its ability to enter protective stress states.
-
Make existing antifungal drugs work more effectively.
For example, research in fungal biology has already shown that interfering with certain stress-buffering pathways can increase azole effectiveness in laboratory models.
In the longer term, this type of work could lead to:
🔹 Better Diagnostics
Tests that detect not only resistance mutations, but also stress-adapted or tolerance states.
🔹 More Personalised Treatment
Identifying strains that rely heavily on stress adaptation and adjusting therapy accordingly.
🔹 Combination Strategies
Using antifungal drugs together with agents that reduce fungal stress tolerance, helping prevent persistence.
These ideas are still under investigation, and no lncRNA-based treatments exist yet.
But this research expands the way scientists think about fungal treatment.
7️⃣ Encouraging News
The important message is this:
NAC is actively involved in research that improves our understanding of how Aspergillus behaves under treatment.
This work:
-
Does not suggest current treatments are ineffective.
-
Does not mean patients are resistant.
-
Does highlight why long-term management can be complex.
-
Represents steady progress in understanding fungal biology.
Understanding these regulatory systems is a step toward:
-
Better diagnostics
-
More personalised treatment strategies
-
Improved long-term outcomes
A Reassuring Perspective
If progress feels slow, it is not because you or your clinicians have failed.
It reflects the adaptable survival biology of a fungus living in a complex lung environment.
And importantly, NAC and its research partners — including groups such as Dr. Weaver’s — are working to understand this biology in order to improve care.
Aspergillosis Literature Update: Week 5
This week’s aspergillosis research highlights evolving management of life-threatening haemoptysis in Chronic Pulmonary Aspergillosis (CPA), new insights into antifungal resistance mechanisms, and continued evidence linking post-tuberculosis lung disease with CPA risk. Notably, species beyond Aspergillus fumigatus — including Aspergillus flavus and Aspergillus udagawae — feature prominently, reinforcing the importance of accurate species identification and susceptibility testing in complex or refractory disease.
Weekly Aspergillosis Literature Update
9–15 February 2026
1️⃣ Clinical Complications & Interventional Management
Refractory Massive Haemoptysis in Chronic Pulmonary Aspergillosis
Superselective Pulmonary Artery Embolization for Refractory Massive Hemoptysis Post-Bronchial Artery Embolization: A Bail-Out Measure
Cardiovasc Intervent Radiol (Feb 15, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41692834/
Focus: Advanced haemoptysis management in Chronic Pulmonary Aspergillosis (CPA)
-
6 of 7 patients had CPA
-
All had failed prior bronchial artery embolization (BAE)
-
Pulmonary artery embolization used as salvage therapy
Why this matters:
Suggests a potential pathway for CPA patients with persistent life-threatening bleeding when conventional embolization fails.
2️⃣ Antifungal Resistance & Drug Sensitivity Mechanisms
Novel Caspofungin Resistance in Aspergillus flavus
Ubiquinone-based gene mutation and protein compactness of CoQ5 may contribute to a novel caspofungin resistance mode in Aspergillus flavus
Diagn Microbiol Infect Dis (Feb 9, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41690241/
Focus: Echinocandin resistance biology
-
Suggests mitochondrial/ubiquinone-linked mechanism
-
Moves beyond classical cell wall mutation models
-
Highlights increasing importance of non-fumigatus species
Why this matters:
Resistance biology is becoming more complex — molecular surveillance may need to expand.
Long Non-Coding RNAs and Antifungal Sensitivity
Genome-wide discovery and phenotyping of non-coding transcripts in A. fumigatus reveals lncRNAs with a role in antifungal drug sensitivity
Nat Commun (Feb 11, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41673015/
Focus: Regulatory genomics in antifungal response
-
Identifies long non-coding RNAs influencing drug sensitivity
-
Suggests new regulatory layers in antifungal resistance
-
Opens potential future therapeutic targets
Why this matters:
Signals a shift from single-gene resistance thinking toward systems-level regulation.
3️⃣ Species-Specific Virulence & Emerging Pathogens
Virulence of Aspergillus flavus and Relatives
Virulence of Aspergillus flavus and relatives using the Galleria mellonella model
Virulence (Epub Feb 13, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41685886/
Focus: Comparative pathogenicity
-
Demonstrates variability in virulence among related species
-
Reinforces need for accurate species identification
Why this matters:
Species differentiation has prognostic and potentially therapeutic implications.
Fatal Dissemination from Cryptic Species
Fatal Fungal Peritonitis Caused by Aspergillus udagawae: An Autopsy Case Report
Intern Med (Feb 10, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41672531/
Focus: Disseminated disease from chronic pulmonary infection
-
Multidrug-resistant A. udagawae
-
Autopsy-confirmed fatal fungal peritonitis
-
Highlights invasive potential of cryptic species
Why this matters:
Supports advanced diagnostics and susceptibility testing in refractory cases.
4️⃣ Structural Lung Disease & Secondary Aspergillosis
CPA Following Cavities and Prednisolone
Chronic pulmonary aspergillosis as a complication of lung cavities and prednisolone treatment
Ugeskr Laeger (Feb 9, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41685454/
Focus: Steroids + cavitation as CPA risk factors
-
Imaging and microbiology confirmed diagnosis
-
Long-term azole therapy successful
-
IgG normalisation observed
Why this matters:
Reinforces the structural lung disease + corticosteroid risk interaction.
Post-Tuberculosis Lung Disease and CPA
Post-tuberculosis lung disease and pulmonary aspergillosis management: challenges and considerations
Expert Rev Anti Infect Ther (Feb 12, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41674445/
Focus: Global burden interface
-
Post-TB structural damage predisposes to CPA
-
Major diagnostic and management challenges highlighted
Why this matters:
Post-tuberculosis lung disease remains one of the largest global drivers of CPA.
5️⃣ Mixed & Extrapulmonary Presentations
Abdominal Wall Aspergillosis
Letter: Abdominal Wall Aspergillosis
Surg Infect (Feb 12, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41680095/
Focus: Extrapulmonary aspergillosis
-
Uncommon presentation
-
Reinforces need for broad diagnostic awareness
Mixed Tuberculosis and Aspergillus Infection
Milky Tea-Colored Pleural Effusion: Empyema Complicated by Pneumothorax Due to Mixed Infection With Mycobacterium tuberculosis and Aspergillus fumigatus
Am J Case Rep (Feb 10, 2026)
🔗 https://pubmed.ncbi.nlm.nih.gov/41664446/
Focus: Dual infection
-
Structural damage enables mixed infection
-
TB diagnosis does not exclude concurrent aspergillosis
Overall Themes This Week
-
🔴 Haemoptysis management continues to evolve in advanced CPA
-
🧬 Resistance mechanisms are becoming increasingly complex
-
🌍 Post-tuberculosis lung disease remains central to global CPA burden
-
🧫 Species identification is clinically important
-
⚠ Mixed and disseminated infections continue to challenge diagnosis
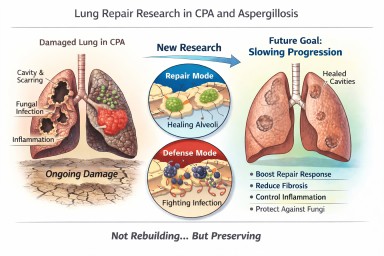
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?
What New Research Means for People with CPA (and Other Aspergillosis)
A recent scientific discovery has helped researchers understand how certain lung cells decide whether to focus on repairing damage or defending against infection. The work, highlighted by the Mayo Clinic and published in Nature Communications, describes a molecular “switch” inside specialised lung cells that influences this balance.
For people living with Chronic Pulmonary Aspergillosis (CPA) — and also those with Allergic Bronchopulmonary Aspergillosis (ABPA) — this kind of research is relevant. But it needs careful explanation.
This is not about rebuilding destroyed lungs.
It is about understanding how to better protect and preserve the lung tissue that remains.
The Discovery: A “Repair vs Defence” Switch
Researchers identified a regulatory circuit in alveolar type II (AT2) cells — specialised cells that:
-
Produce surfactant (which keeps air sacs open)
-
Act as a reserve “repair” population in the lung
-
Can regenerate other essential lung cells after injury
The study showed that these cells operate under tight control. When infection is present, they prioritise defence. When injury needs healing, they can switch into repair mode.
The key insight is that this switch is biologically regulated. It is not random. That means, in theory, it may one day be possible to influence it.
What “Repair” Means — and What It Does Not Mean
When we talk about lung repair in this context, we must be very clear.
It does not mean:
-
Lung cavities caused by CPA will close in the foreseeable future
-
Established fibrosis will melt away
-
Bronchiectasis will reverse
-
Severely distorted lung architecture will rebuild
CPA cavities represent major structural remodelling — destruction of alveoli, scarring, altered blood supply, and thickened pleura. Reconstructing that complex architecture is biologically extremely challenging and not currently realistic within the next decade.
What repair does realistically mean
In chronic lung disease, “repair” is more likely to mean:
-
Supporting survival of remaining alveoli
-
Preventing excessive fibrotic signalling
-
Helping lung lining cells recover more efficiently after inflammation
-
Reducing cumulative injury from repeated infection
-
Slowing progression of structural change
In other words:
Not rebuilding what is gone — but better protecting what remains.
For many people with CPA, this is a crucial distinction.
Why Preservation Is a Major Goal in CPA
CPA usually develops in lungs already weakened by conditions such as tuberculosis, non-tuberculous mycobacteria, chronic obstructive pulmonary disease, or severe pneumonia.
Over time, CPA can lead to:
-
Expanding cavities
-
Progressive scarring
-
Reduced gas exchange
-
Reduced exercise tolerance
Many patients have limited lung reserve. Even small additional losses of functioning lung tissue can significantly increase breathlessness or fatigue.
If future therapies could slow the rate of progression — even modestly — that would meaningfully affect long-term outcomes.
Flattening the decline curve is not trivial. It changes quality of life.
Why This Also Matters in ABPA
In ABPA, repeated inflammatory episodes can lead to:
-
Airway remodelling
-
Mucus plugging
-
Development or progression of bronchiectasis
Better control of inflammatory signalling — combined with improved epithelial recovery — could reduce long-term airway damage.
Again, this is about preservation rather than reversal.
Where Development Has Reached
The current research is still laboratory-based. It used advanced techniques such as:
-
Single-cell sequencing
-
Imaging of lung tissue
-
Preclinical models of injury
No human treatments based on this discovery are yet available.
However, the significance lies in identifying:
-
A defined molecular pathway
-
A controllable regulatory mechanism
-
A clearer understanding of why repair fails in chronic inflammation
That foundational knowledge is what eventually allows targeted drug development.
The Balance Challenge in Aspergillosis
There is an additional complexity in fungal lung disease.
Any attempt to promote repair must not weaken antifungal defence.
The immune system must:
-
Control Aspergillus
-
Avoid causing excessive inflammatory damage
Future therapies would need to strike that balance carefully.
What This Means for Patients Now
This discovery does not change current treatment.
The most effective preservation strategies today remain:
-
Consistent antifungal therapy when indicated
-
Careful inflammatory control
-
Biologic therapies where appropriate
-
Airway clearance
-
Vaccination and infection prevention
-
Avoiding damp and mould exposure
-
Pulmonary rehabilitation
These measures are already forms of lung preservation.
A Realistic and Hopeful Perspective
It is unlikely that cavities from CPA will be repaired in the near future.
It is realistic that within the next 5–10 years we may see improved strategies aimed at:
-
Slowing structural progression
-
Supporting endogenous repair cells
-
Reducing fibrotic signalling
-
Improving recovery after exacerbations
For people living long-term with CPA or ABPA, even incremental preservation could significantly affect independence and quality of life.
The science is still early — but understanding how the lung decides to repair itself is an important step forward.
Reference
Sawhney, A.S., Deskin, B.J., Cai, J. et al. A molecular circuit regulates fate plasticity in emerging and adult AT2 cells. Nat Commun 16, 8924 (2025). https://doi.org/10.1038/s41467-025-64224-1
🧬 How Biologics Are Reshaping Our Understanding of ABPA Subtypes
For many years, Allergic Bronchopulmonary Aspergillosis (ABPA) was viewed as a single condition:
An allergic reaction to Aspergillus fumigatus in the lungs, treated primarily with steroids and sometimes antifungal medication.
Biologic therapies are changing that picture.
They are not just new treatments — they are helping us understand that ABPA may not be one uniform disease, but a spectrum of related inflammatory patterns.
🧠 The Traditional View of ABPA
Historically, ABPA has been defined by:
-
Asthma (or cystic fibrosis)
-
High total IgE
-
Sensitisation to Aspergillus
-
Raised eosinophils
-
Characteristic CT changes (e.g. bronchiectasis, mucus plugging)
The dominant biological explanation was:
A Type 2 (allergic) immune overreaction driven by eosinophils and IgE.
Steroids were used to suppress this immune response.
This model assumed that most patients had broadly similar immune drivers.
💊 What Are Biologics?
Biologics are targeted antibody therapies designed to block specific immune pathways.
In asthma and ABPA, the main targets are:
-
IL-5 (drives eosinophils)
-
IL-5 receptor
-
IL-4 / IL-13 (drive allergic inflammation)
-
IgE
Examples include:
-
Anti–IL-5 therapies (e.g. mepolizumab, benralizumab)
-
Anti–IL-4/IL-13 therapy (e.g. dupilumab)
-
Anti-IgE therapy (e.g. omalizumab)
Instead of broadly suppressing immunity like steroids, they selectively block parts of the allergic pathway.
🔍 What Biologics Are Teaching Us
As biologics have been used in ABPA (often off-label or in specialist centres), an interesting pattern has emerged:
Not all ABPA behaves the same way.
Some patients respond dramatically to anti–IL-5 therapy.
Others respond better to anti–IL-4/IL-13 therapy.
Some show strong IgE-driven disease.
Others appear more mucus-dominant.
This suggests that ABPA may include different inflammatory endotypes (biological subtypes), even if outward symptoms look similar.
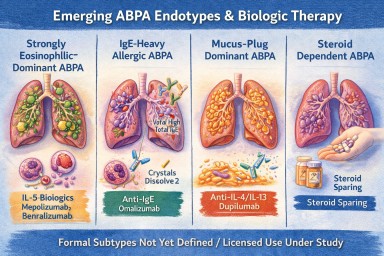
🧩 Possible Emerging ABPA Subtypes
While research is ongoing, clinicians are beginning to recognise patterns such as:
1️⃣ Strongly Eosinophilic-Dominant ABPA
-
Very high eosinophils
-
Frequent exacerbations
-
Often responds well to IL-5 blockade
2️⃣ IgE-Heavy Allergic ABPA
-
Extremely high total IgE
-
Prominent allergic features
-
May respond to anti-IgE therapy
3️⃣ Mucus-Plug Dominant ABPA
-
Recurrent thick mucus impaction
-
Radiological plugging
-
May involve additional inflammatory drivers
4️⃣ Steroid-Dependent ABPA
-
Relapses when steroids reduced
-
Biologics may allow steroid-sparing strategies
These patterns are not yet formal categories, but biologics are revealing that ABPA is biologically more complex than once thought.
🧪 Blood Eosinophils vs Airway Inflammation
Biologics have also highlighted another key insight:
Blood eosinophil levels do not always perfectly reflect what is happening in the lungs.
Some patients:
-
Have modest blood eosinophils
-
But still show eosinophilic airway activity
Biologic response patterns are helping refine how we interpret these markers.
🧠 Moving From “Diagnosis” to “Endotype”
Traditionally, medicine focused on:
Diagnosis (ABPA vs not ABPA)
Biologics are pushing us toward:
Endotype (which immune pathway is dominant in this patient?)
This matters because targeted therapy works best when matched to the dominant pathway.
In future, ABPA may be classified not just by clinical features, but by molecular drivers.
🫁 What This Means for Patients
Biologics offer:
-
Reduced steroid dependence
-
Fewer exacerbations
-
Improved lung function in selected patients
-
Potential improvement in mucus burden
But they also help answer deeper questions:
-
Why do some patients relapse frequently?
-
Why do some have extreme eosinophilia?
-
Why do others have more mucus plugging than inflammation?
They are helping personalise ABPA care.
⚖ Important Caveats
-
Biologics are not currently licensed specifically for ABPA in many countries.
-
Evidence is growing but still developing.
-
They are usually considered in specialist centres.
-
They are not appropriate for every patient.
Steroids and antifungals remain core treatments.
🔭 The Future
Over the next decade, we may see:
-
Better classification of ABPA subtypes
-
Biomarker-guided treatment selection
-
Reduced long-term steroid exposure
-
Improved understanding of mucus plug biology
-
Trials specifically designed for ABPA (rather than extrapolated from asthma)
Biologics are not just new drugs.
They are acting as scientific tools that are reshaping how we think about ABPA itself.
🧠 Key Takeaway
ABPA is no longer seen as one single uniform allergic condition.
Biologic therapies are revealing that:
ABPA is likely a spectrum of related inflammatory patterns — and treatment may increasingly be tailored to the dominant pathway in each individual.
References
Agarwal R, Sehgal IS, Muthu V, Denning DW, Chakrabarti A, Soundappan K, Garg M, Rudramurthy SM, Dhooria S, Armstrong-James D, Asano K, Gangneux JP, Chotirmall SH, Salzer HJF, Chalmers JD, Godet C, Joest M, Page I, Nair P, Arjun P, Dhar R, Jat KR, Joe G, Krishnaswamy UM, Mathew JL, Maturu VN, Mohan A, Nath A, Patel D, Savio J, Saxena P, Soman R, Thangakunam B, Baxter CG, Bongomin F, Calhoun WJ, Cornely OA, Douglass JA, Kosmidis C, Meis JF, Moss R, Pasqualotto AC, Seidel D, Sprute R, Prasad KT, Aggarwal AN. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses. Eur Respir J. 2024 Apr 4;63(4):2400061. doi: 10.1183/13993003.00061-2024. PMID: 38423624; PMCID: PMC10991853.
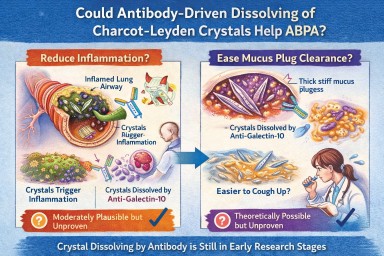
🧬 Could Antibody-Driven Dissolving of Charcot–Leyden Crystals Help ABPA?
Researchers have recently discovered that Charcot–Leyden crystals (CLCs) — the needle-shaped structures formed from the eosinophil protein galectin-10 — are not just debris.
In laboratory studies, specially designed antibodies can dissolve these crystals.
This has raised two important questions:
-
Could dissolving the crystals reduce airway inflammation?
-
Could dissolving them make mucus plugs easier to clear?
Here is what we currently know.
1️⃣ Could dissolving crystals reduce airway inflammation?
What we know
Laboratory and animal studies have shown:
-
Charcot–Leyden crystals can activate immune cells (especially macrophages).
-
They can stimulate inflammatory pathways (including inflammasome signalling).
-
In mouse models, antibodies targeting galectin-10 dissolved the crystals.
-
When crystals were dissolved, airway inflammation decreased.
This suggests that the crystals themselves may amplify inflammation, rather than simply mark it.
What this means biologically
In ABPA and eosinophilic asthma:
-
Eosinophils release galectin-10.
-
Galectin-10 crystallises.
-
Crystals may trigger further immune activation.
-
That leads to more inflammation → more eosinophils → more crystals.
Dissolving the crystals could theoretically interrupt this feedback loop.
How likely is this to help inflammation in humans?
Moderately plausible, but not yet proven.
The biological mechanism is strong.
The animal data are encouraging.
But no human clinical trials have yet shown reduced inflammation through crystal dissolution.
If developed successfully, this approach could:
-
Reduce airway immune activation
-
Lower exacerbation risk
-
Potentially reduce steroid dependence
But at present, it remains investigational.
2️⃣ Could dissolving crystals make mucus plugs easier to cough up?
This is more speculative — but still biologically reasonable.
Why mucus plugs are so thick in ABPA
ABPA mucus plugs contain:
-
Gel-forming mucins
-
DNA from inflammatory cells
-
Dead cells
-
Fungal fragments
-
Eosinophil proteins
-
Charcot–Leyden crystals
The crystals are:
-
Rigid
-
Needle-shaped
-
Structurally stable
When embedded in mucus, they likely increase:
-
Mechanical stiffness
-
Plug density
-
Resistance to deformation
From a physics perspective:
Removing rigid crystalline structures from a gel should reduce stiffness and improve flow.
Do we have direct evidence?
No.
There are currently:
-
No human studies measuring mucus clearance after crystal dissolution
-
No trials showing improved plug expectoration from crystal-targeting therapy
So while it is plausible that dissolving crystals could soften plugs, this has not yet been demonstrated in patients.
3️⃣ How strong is the overall case?
| Outcome | Evidence strength | Likelihood |
|---|---|---|
| Reduced inflammation | Strong biological rationale + animal data | Moderately promising |
| Easier mucus clearance | Biophysical plausibility only | Possible but unproven |
Inflammation reduction is the more evidence-supported target.
Improved plug clearance is plausible but currently theoretical.
4️⃣ How does this compare to existing treatments?
Current therapies (e.g., anti-IL-5 biologics) reduce eosinophils upstream.
That leads to:
-
Less galectin-10 release
-
Fewer crystals forming
-
Reduced inflammation
-
Often improved mucus plugging
So biologics already indirectly reduce crystal burden.
A crystal-dissolving antibody would act downstream, targeting the structural product directly.
This could theoretically:
-
Accelerate resolution of existing plugs
-
Reduce residual inflammatory signalling
But again, this remains in early research stages.
5️⃣ Practical take-home message
At present:
-
Dissolving Charcot–Leyden crystals reduces inflammation in animal models.
-
It is biologically plausible that this could also soften mucus plugs.
-
There is no human clinical proof yet.
-
No approved therapy currently targets the crystals directly.
The concept is scientifically credible — but still under development.
🔭 The Bigger Picture
ABPA is increasingly understood as a condition driven by:
-
Eosinophils
-
Allergic immune signalling
-
Abnormal mucus biology
-
Structural plug formation
Crystal-targeting therapies may eventually become part of a more precise approach to treating eosinophilic airway disease.
But for now, they remain a promising research direction rather than a clinical option.
🔬 Charcot–Leyden Crystals in ABPA and Asthma
What are they? Why do they form? Do they matter?
If you live with Allergic Bronchopulmonary Aspergillosis (ABPA) or severe asthma, you may see the term Charcot–Leyden crystals in a sputum or pathology report.
They can sound worrying.
They are:
-
Not fungus
-
Not infection
-
Not cancer
They are a sign of a particular type of allergic inflammation in the airways.
🧬 What Are Charcot–Leyden Crystals?
Charcot–Leyden crystals are microscopic, needle-shaped structures found in mucus.
They are made from a protein called galectin-10, which is stored inside a type of white blood cell called an eosinophil.
Eosinophils are immune cells involved in:
-
Allergic asthma
-
ABPA
-
Severe asthma with fungal sensitisation
-
Parasitic infections
When eosinophils are activated and break down, they release galectin-10.
If enough of this protein accumulates in thick airway mucus, it crystallises into visible crystals.
So the crystals are made from your immune cells, not from Aspergillus.
🫁 Why Do They Appear in ABPA?
In ABPA:
-
The immune system overreacts to Aspergillus fumigatus.
-
This triggers a strong allergic (Type 2) immune response.
-
Large numbers of eosinophils move into the airways.
-
Eosinophils break down and release galectin-10.
-
The protein crystallises inside mucus plugs.
The crystals are therefore a footprint of intense allergic inflammation, not fungal invasion.
🌡 Is Most ABPA Eosinophilic?
Yes — almost all classical ABPA is eosinophilic.
ABPA is fundamentally a Type 2 allergic condition, driven by immune pathways involving:
-
IL-4
-
IL-5
-
IL-13
-
IgE
-
Eosinophils
IL-5 in particular stimulates eosinophil production and survival.
Because of this, eosinophils are central to the disease process.
Historically, raised blood eosinophils have been part of diagnostic criteria.
However:
-
Eosinophil counts can fluctuate
-
Steroids can suppress blood levels
-
Eosinophils may still be present in airway mucus even if blood counts appear normal
So ABPA is biologically eosinophilic — even if a single blood test does not show a high count.
True non-eosinophilic ABPA would be unusual and would prompt clinicians to reconsider the diagnosis.
❓ Are Crystals Caused by Aspergillus Infection?
No.
They are caused by the immune reaction to Aspergillus — not by the fungus itself.
They can also be seen in:
-
Severe eosinophilic asthma
-
Parasitic infections
-
Other allergic lung conditions
They reflect eosinophil activity, not fungal growth.
🧠 Why Don’t All People with Asthma Develop These Crystals?
Asthma is not one single disease. It has different inflammatory patterns.
Type 2 (Eosinophilic) Asthma
This involves high eosinophils and allergic pathways.
Common in:
-
Allergic asthma
-
ABPA
-
Severe eosinophilic asthma
These patients can develop Charcot–Leyden crystals.
Non–Type 2 (Non-Eosinophilic) Asthma
This includes:
Neutrophilic asthma
Driven by neutrophils rather than eosinophils.
Paucigranulocytic asthma
Very few inflammatory cells present.
In these forms:
-
Eosinophils are low
-
Galectin-10 is not released in large amounts
-
Crystals are unlikely to form
🧱 Do Charcot–Leyden Crystals Make Mucus Plugs Worse?
Possibly.
Research suggests they may:
-
Increase mucus thickness
-
Contribute mechanically to airway blockage
-
Stimulate further inflammation
For many years they were thought to be harmless debris.
Modern studies suggest they may actively amplify inflammation when present in large amounts.
🎯 Do They Have a Purpose?
Eosinophils evolved mainly to help fight parasitic infections.
Galectin-10 probably has immune signalling roles inside cells.
However, when large amounts are released into thick airway mucus, crystallisation appears to be a by-product of excessive immune activity rather than a useful defence.
In ABPA and allergic asthma, they are more likely part of the problem than part of the solution.
💧 Can Their Formation Be Reduced?
Hydration alone does not stop them forming.
Drinking fluids helps:
-
Keep mucus less sticky
-
Support airway clearance
But it does not prevent eosinophils releasing galectin-10.
What reduces crystal formation?
Reducing eosinophilic inflammation:
-
Corticosteroids
-
Anti-IL-5 biologics
-
Anti-IL-4/IL-13 biologics
When eosinophil numbers fall:
→ Less galectin-10 is released
→ Fewer crystals form
Antifungal treatment in ABPA may indirectly help by reducing allergic stimulation, but the main driver is the immune response.
📊 Do They Change Treatment?
Not directly.
Doctors base treatment on:
-
Symptoms
-
Blood eosinophils
-
Total IgE
-
Imaging
-
Lung function
-
Exacerbation history
Crystals support the diagnosis of eosinophilic inflammation but do not determine treatment alone.
🔎 What Do They Tell Us?
Charcot–Leyden crystals tell us:
-
The airway inflammation is eosinophilic.
-
The immune response is strongly allergic.
-
Mucus plugging risk may be higher.
They are a marker of immune overreaction, not infection severity.
🧠 Key Points to Remember
-
They are made from proteins released by eosinophils.
-
They are not Aspergillus.
-
They do not mean invasive fungal infection.
-
Most classical ABPA is eosinophilic.
-
They are unlikely in non-eosinophilic asthma.
-
Reducing eosinophils reduces their formation.
-
Hydration helps clearance but does not prevent formation.
In simple terms:
Charcot–Leyden crystals are microscopic signs that the immune system is working too hard in the airways.