Building fitness with Aspergillosis
Last reviewed: 20 March 2026
Audience: Patients, carers, families, and non-specialists
Applies to: Allergic bronchopulmonary aspergillosis (ABPA), chronic pulmonary aspergillosis (CPA), Aspergillus bronchitis, severe asthma with fungal sensitisation (SAFS)
Why it feels so hard — and how to improve safely
Key points
- Feeling exhausted after activity is common in aspergillosis and does not mean you are failing.
- Breathlessness and fatigue are often due to lung changes, not just “lack of fitness”.
- Pushing too hard can make symptoms worse — pacing is essential.
- Small, steady increases in activity are more effective than big efforts.
- Respiratory physiotherapy can make a major difference.
- Some patients (e.g. with cavities or haemoptysis) need tailored, cautious approaches.
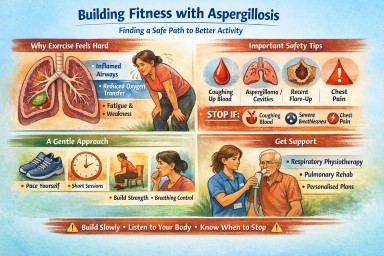
Why exercise feels so difficult
Many people with aspergillosis find that even simple activity can feel exhausting.
This is not just about fitness. It is often due to changes in how the lungs and body work, including:
- Inflamed or narrowed airways
- Mucus affecting airflow
- Reduced oxygen transfer
- Increased effort needed to breathe
In addition:
- Long-term illness can reduce muscle strength
- Treatments such as steroids may affect weight and energy
- Many people experience post-exertional fatigue (feeling worse after activity)
This means your body is working harder than it used to — even for everyday tasks.
Why “just doing more” can backfire
It is natural to think that pushing harder will improve fitness. However, in aspergillosis this often leads to a cycle:
- Doing too much on a “good day”
- Feeling exhausted afterwards
- Needing longer recovery
- Losing confidence
This is sometimes called a “boom and bust” cycle.
The goal is not to push harder — it is to build steadily and sustainably.
A safer way to build fitness
1. Find your baseline
Start with what you can do without feeling completely exhausted afterwards.
This may be much less than you expect — and that is normal.
2. Use the 70–80% rule
Only do about 70–80% of what you feel capable of.
This helps prevent setbacks and allows gradual improvement.
3. Break activity into smaller chunks
Short sessions (e.g. 10–15 minutes) with rest in between are often easier than one long effort.
4. Use breathing control
Pursed-lip breathing:
- Breathe in through your nose
- Breathe out slowly through pursed lips
This helps keep airways open and reduces breathlessness.
5. Add gentle strength work
Improving muscle strength can reduce breathlessness and improve stamina.
- Sit-to-stand from a chair
- Light squats (with support)
- Step-ups
Start small — 2–3 times per week is enough.
The role of respiratory physiotherapy
Respiratory physiotherapy can be one of the most helpful supports available.
A respiratory physiotherapist can help with:
- Breathing techniques to reduce breathlessness
- Airway clearance to manage mucus
- Tailored exercise plans at the right pace
- Confidence in what is safe to do
You may be offered this as pulmonary rehabilitation.
If you have not been referred, it is worth asking your GP or specialist team.
⚠️ Important safety advice (including bleeding risk)
Exercise is helpful for many people with aspergillosis — but it is not always appropriate to increase activity without guidance.
Be especially cautious if you have:
- Coughing up blood (haemoptysis) — current or recent
- An aspergilloma (fungal ball)
- Lung cavities
- A recent flare or worsening symptoms
Why this matters
In some forms of aspergillosis, blood vessels in the lungs can become fragile. Strain or increased pressure in the chest can increase the risk of bleeding.
When to stop and seek advice
- Coughing up blood (even small amounts)
- Sudden increase in breathlessness
- Chest pain or tightness
- Feeling significantly worse after activity
How to exercise more safely (if stable)
- Keep activity gentle and controlled
- Avoid heavy lifting or straining
- Avoid holding your breath during exertion
- Build activity gradually
If you are unsure, seek advice from your specialist team or a respiratory physiotherapist before increasing activity.
What progress really looks like
Improvement is rarely a straight line.
- Some days will be better than others
- Setbacks are common
- Progress may be slow but meaningful
This is normal in chronic lung conditions.
When to seek medical advice
Contact your healthcare team if you experience:
- New or worsening breathlessness
- Changes in cough or sputum
- Chest pain
- Coughing up blood
- Severe or persistent fatigue
Final message
Living with aspergillosis changes how your body responds to activity.
But improvement is possible — with the right approach.
Build slowly, pace yourself, and get the right support — especially from a respiratory physiotherapist.
In one sentence
Exercise can help — but it must be paced, personalised, and safe for your type of aspergillosis.
A Drop of Blood, Real-Time Answers
Last reviewed: 20 March 2026
Audience: Patients, carers, families, and non-specialists
Topic: Point-of-care monitoring of antifungal drug levels
New bedside testing for antifungal drugs — and why patients welcome it
For many people taking antifungal medicines, blood tests are an important part of care. These tests help doctors check whether the amount of medicine in the body is too low, too high, or about right.
A new type of technology is being developed to do this much more quickly, using just a single drop of blood placed onto a specialised chip. Instead of sending blood away to a laboratory and waiting days for a result, this kind of test may be able to provide an answer much more quickly, sometimes during the clinic visit itself.
Patients in a recent focus group responded very positively to this idea. They welcomed not only the technology itself, but also what it could mean for their care: less waiting, less uncertainty, fewer trips to hospital, and more personalised treatment.
Key points
- A new test can measure antifungal drug levels from a drop of blood.
- The blood is placed on a specialised chip containing tiny sensors.
- Results may be available much faster than standard laboratory testing.
- This could help doctors adjust treatment more quickly and more precisely.
- Patients in a focus group strongly welcomed the technology.
- Reported benefits included less anxiety, fewer hospital visits, and more confidence in treatment decisions.
What is this new test?
This is a type of point-of-care test. That means it is designed to be used close to the patient, such as in a clinic or at the bedside, rather than sending the sample away to a central laboratory.
In this case, the aim is to measure the level of an antifungal drug in the blood from a very small sample, sometimes just a finger-prick drop. The drop of blood is placed onto a specialised chip. That chip contains tiny channels and sensors that can detect the amount of drug present.
People sometimes describe this type of system as a “lab on a chip” because it performs some of the work of a laboratory in a very small device.
How does the technology work?
The exact science varies between devices, but the general idea is similar.
- A small blood sample is taken.
This may be from a finger prick rather than a larger blood draw. - The blood is placed onto a specialised chip.
The chip is designed to handle a tiny volume of blood. - The blood moves through microscopic channels.
These channels guide the sample to the parts of the chip that do the measurement. - Sensors on the chip detect the antifungal drug.
These sensors are designed to recognise the drug or react to it in a measurable way. - A reader produces a result.
A connected device reads the signal from the chip and estimates the drug level.
Some systems use electrical signals, some use light, and some use chemical reactions. Patients do not need to understand all the engineering details to understand the main point: the chip is acting like a mini laboratory.
A simple way to think about it is this:
Instead of sending your blood sample to a distant laboratory, this technology brings part of the laboratory to your fingertip.
Why do antifungal drug levels matter?
Some antifungal medicines need careful monitoring because the “right” level can be quite important.
If the drug level is too low, the medicine may not work well enough. If the drug level is too high, side effects may become more likely.
This can be especially relevant for antifungal drugs such as:
- itraconazole
- voriconazole
- posaconazole
Drug levels can vary from person to person for many reasons, including:
- how well the body absorbs the medicine
- interactions with other medicines
- differences in liver function and metabolism
- changes in health over time
At present, monitoring usually involves sending blood to a laboratory. That works, but it can mean delays. Results may not come back quickly enough to guide decisions during the clinic appointment itself.
A faster bedside test could help clinicians make treatment decisions more quickly and could support more personalised care.
What did patients say about it?
In the patient focus group, this technology was widely welcomed. Patients were not only interested in the novelty of the test. They also recognised several practical benefits that could make day-to-day care easier and safer.
1. Faster results could reduce anxiety
Many patients described the stress of waiting for test results. Waiting can create a sense of uncertainty: Is the treatment working? Is the dose correct? Are side effects more likely?
A test that gives much quicker results was seen as reassuring. Instead of waiting days, patients liked the idea of getting answers much sooner, possibly while still in clinic.
2. Fewer visits could reduce the burden of care
For many people with chronic lung conditions or long-term illness, going to hospital is not a small task. Travel, parking, breathlessness, fatigue, mobility problems, and long waits can make even a short appointment exhausting.
Patients felt that a faster and simpler test could reduce some of this burden, especially if it could be built into a normal appointment or eventually be offered closer to home.
3. More personalised dosing felt important
Patients often understand from experience that medicines do not affect everyone in the same way. One person may tolerate a treatment well, while another may have side effects or absorb the medicine differently.
Because of this, patients valued the idea that treatment could be adjusted based on their own measured drug level, rather than relying only on standard dosing. This gave a stronger sense that care was being tailored to the individual.
4. Closer monitoring gave reassurance about safety
Antifungal drugs can be very helpful, but patients also know that some of them can have side effects and interactions. That can make treatment feel worrying, especially over longer periods.
Patients said that being able to check drug levels more quickly and more easily could help them feel safer. It suggested that treatment was being watched closely rather than left unchecked between appointments.
5. Immediate results could help patients feel more involved
Another important theme was involvement. Patients often feel that blood is taken, results disappear into the system, and decisions come later without much real-time discussion.
By contrast, a bedside result creates the possibility of discussing the number there and then. Patients felt this could help them better understand their treatment and feel more involved in decisions about dose changes and ongoing care.
6. It seemed to fit better with real life
Patients repeatedly emphasised that long-term treatment has to fit around real lives, not just clinic systems. Many welcomed the idea of a test that was quicker, simpler, and potentially more convenient.
In that sense, what patients welcomed was not just a chip or a machine, but a model of care that felt more responsive and more human-centred.
What could this mean for future care?
If this technology proves accurate, reliable, and affordable, it could support a different way of monitoring antifungal treatment.
Possible future benefits could include:
- drug level testing during the clinic appointment itself
- faster dose adjustment when levels are too high or too low
- closer monitoring when starting or changing treatment
- fewer repeat visits just to check blood levels
- potential future use in community settings or, one day, at home
It is important to be realistic. New technologies must be carefully tested before they become routine. They need to be shown to be accurate, dependable, and practical in real healthcare settings.
Even so, patients clearly recognised the potential. For them, this is not just about speed. It is about moving toward care that is:
- more responsive
- more personalised
- more convenient
- less anxiety-provoking
Common questions
Is this available now?
Usually not as a routine test in most healthcare settings. It is still being developed and studied, although interest in this type of monitoring is growing.
Will this replace ordinary blood tests?
Not immediately. Standard laboratory testing is still important. New bedside systems may first be used alongside existing methods while they are being evaluated and introduced.
Would this work for every antifungal drug?
Not necessarily. Some devices may be designed for specific drugs first. Wider use would depend on the technology and the evidence supporting it.
Could this be used at home?
Possibly one day, but that is likely to depend on how reliable, affordable, and easy to use the technology becomes. For now, clinic or bedside use is the more immediate possibility.
Why is a drop-of-blood test appealing to patients?
Because it may mean quicker answers, less uncertainty, fewer hospital trips, and more confidence that treatment decisions are based on what is happening in their own body.
When to seek medical advice
You should contact your healthcare team if you:
- develop new or worsening side effects from your antifungal medicine
- feel your treatment is not helping
- have concerns about drug interactions with other medicines
- are unsure whether to continue, stop, or change your medication
A new bedside test could support treatment decisions, but it would not replace medical advice. Symptoms, scans, blood tests, and clinical review would still matter.
Final thoughts
This new chip-based bedside technology may sound futuristic, but the reason patients welcomed it is very straightforward.
They saw the possibility of care that is faster, clearer, safer, and better adapted to real life.
In other words, this is about more than measuring a drug level from a drop of blood. It is about moving away from delayed, one-size-fits-all monitoring and toward real-time, personalised, patient-centred care.
In one sentence
A tiny chip and a drop of blood could help doctors adjust antifungal treatment more quickly — and patients believe that could make care less stressful, less burdensome, and more personal.

Understanding the Journey to Diagnosis (Start Here)
Last reviewed: 18 March 2026
Key points
- Aspergillosis can be difficult to diagnose because symptoms often overlap with more common illnesses.
- Long diagnostic journeys are common in many chronic and uncommon conditions, not just aspergillosis.
- Uncertainty does not mean symptoms are unreal.
- Diagnosis often becomes clearer over time, as symptoms, scans, tests, and patterns build up.
- Good communication, ongoing review, and specialist input can make a major difference.

Why we created this series
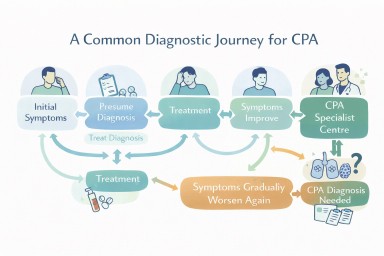
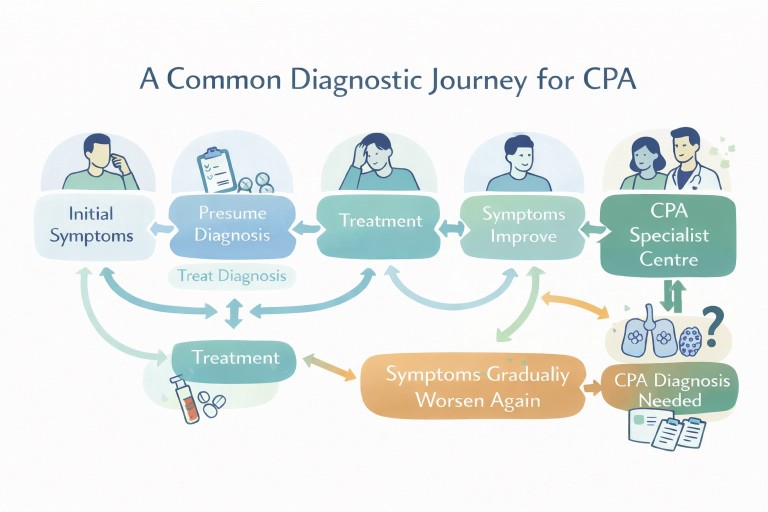
People living with aspergillosis often tell us that the hardest part was not only the illness itself, but the time before they had an answer. Many describe repeated symptoms, multiple appointments, courses of treatment that only partly helped, and a growing sense that something still did not fit.
This experience is common in conditions such as chronic pulmonary aspergillosis (CPA) and allergic bronchopulmonary aspergillosis (ABPA), but it is also seen much more widely across medicine.
We created this series to help make sense of that process in a way that is:
- clear and accessible for patients and carers
- respectful of clinicians working within complex systems
- honest about uncertainty, delay, and emotional impact
- useful for improving understanding on both sides
The articles in this series
1. Why Aspergillosis Is So Hard to Diagnose
This article explains why aspergillosis can be difficult to recognise, why medicine usually starts with more common explanations, and how diagnosis often depends on patterns building up over time rather than one single test.
Best for: understanding the overall process and why delays can happen.
2. When Symptoms Are Real but Answers Are Not: Understanding Uncertainty
This article looks at the emotional and communication side of the diagnostic journey, including why patients may feel unheard, what clinicians may mean when they speak cautiously, and why unexplained symptoms are still real symptoms.
Best for: understanding uncertainty, communication gaps, and the experience of not yet having answers.
3. Why Diagnosis Can Take Time — and Why You Are Not Alone
This article places the diagnostic journey in a wider context, showing that long paths to diagnosis are common in many chronic and complex conditions, and offering reassurance that patients are not alone in this experience.
Best for: reassurance, perspective, and recognising that this journey is shared by many others.
Who may find this series helpful
This series may be useful if you are:
- a patient with ongoing respiratory symptoms and no clear diagnosis yet
- a carer or family member trying to understand what your loved one is going through
- a person recently diagnosed with aspergillosis and looking back on a long journey
- a general practitioner, respiratory clinician, nurse, or allied health professional wanting to better understand the patient perspective
It may also help people with other chronic conditions, because many of the same themes—uncertainty, overlap of symptoms, repeated reassessment, and eventual recognition—are seen across a wide range of illnesses.
When to seek medical advice
Seek medical advice if you have ongoing or worsening symptoms that are not improving as expected, especially if they keep returning or no longer fit the original explanation.
Seek urgent medical advice if you have symptoms such as:
- coughing up blood
- rapidly worsening breathlessness
- new chest pain
- significant unexplained weight loss
- high fever or signs of severe infection
If you already have an underlying lung condition and your usual treatment no longer seems to be working, it is reasonable to ask whether the diagnosis needs to be reviewed.
Why Diagnosis Can Take Time — and Why You Are Not Alone
Last reviewed: 18 March 2026
Key points
- Long diagnostic journeys are common in many chronic and rare conditions—not just aspergillosis.
- Delays do not mean your symptoms were not real or important.
- Diagnosis often becomes clear over time, as patterns develop.
- Many patients go through similar experiences before reaching answers.
- Specialist centres play an important role when conditions are complex.
You are not alone in this
One of the most important things to understand is this:
Long and difficult diagnostic journeys are common—especially in chronic or complex illness.
Many people living with conditions such as chronic pulmonary aspergillosis (CPA) or allergic bronchopulmonary aspergillosis (ABPA) describe months or years of symptoms before a clear diagnosis was made.
This experience, while frustrating, is not unusual—and it does not mean your care has failed.
This happens in many conditions
Aspergillosis is not unique in this respect.
Similar diagnostic journeys are seen in:
- chronic lung diseases
- autoimmune conditions
- rare infections
- conditions with overlapping symptoms (e.g. fatigue syndromes)
In all of these, the same pattern often occurs:
- early symptoms are non-specific
- common conditions are treated first
- tests may initially be normal
- the true pattern only becomes clear over time
Why time helps diagnosis
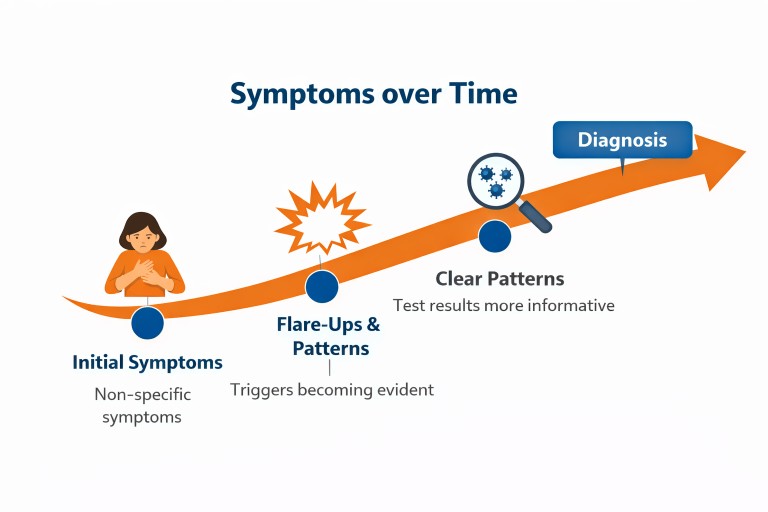
Although it can feel like delay, time often provides essential information.
Patterns emerge
- symptoms become more consistent
- flare-ups follow recognisable triggers
- response to treatment becomes clearer
Tests become more informative
- changes appear on imaging (e.g. CT scans)
- blood markers become more clearly abnormal
- microbiology results become more consistent
What was unclear early on can become much more visible later.
The turning point
Many patients describe a moment when things begin to change:
- symptoms no longer fit common conditions
- treatments stop working as expected
- a clinician recognises a pattern
This is often the point where less common diagnoses—including aspergillosis—are considered.
The role of specialist centres
Complex conditions are often best diagnosed in specialist centres with experience in that field.
In the UK, the National Aspergillosis Centre provides:
- expert multidisciplinary assessment
- access to specialist diagnostics
- experience in recognising patterns of disease
Referral to a specialist centre is often a key step in reaching a diagnosis.
The emotional impact
Long periods without answers can be deeply challenging.
Patients often describe:
- frustration and uncertainty
- feeling unheard or misunderstood
- loss of confidence in their own body
These reactions are entirely understandable.
Your experience is valid—even if the diagnosis took time to emerge.
Moving forward
Once a diagnosis is made, many patients feel a sense of relief—even if treatment is still needed.
A diagnosis provides:
- an explanation for symptoms
- a direction for treatment
- a clearer future plan
Even before diagnosis, it is important to remember:
You are still on a pathway—just not always a straight one.
Common questions
Does a long delay mean something was missed?
Not necessarily. Many conditions are only diagnosable once they have developed further.
Should I have been referred earlier?
Sometimes earlier referral is helpful, but it usually depends on how symptoms evolve over time.
Is this unique to aspergillosis?
No—this pattern is seen across many chronic and rare conditions.
Why Aspergillosis Is So Hard to Diagnose
Last reviewed: 18 March 2026
Key points
- Aspergillosis is often difficult to diagnose because its symptoms can look very similar to those of more common conditions.
- Diagnosis usually depends on several pieces of evidence being brought together, rather than one simple test.
- Doctors are trained to consider common conditions first, because this is usually the safest and most efficient approach.
- This approach works well for many patients, but it can delay recognition of conditions such as aspergillosis.
- Delays are often caused by the way healthcare systems are organised, not by lack of care or effort from individual clinicians.
- Patients can help by keeping a clear record of symptoms, tests, treatments, and how things have changed over time.
Why diagnosis can be difficult
Aspergillosis is not a single illness but a group of conditions caused by Aspergillus, a mould commonly found in the environment. These include:
- Allergic bronchopulmonary aspergillosis (ABPA)
- Chronic pulmonary aspergillosis (CPA)
- Other airway and colonisation-related conditions
Diagnosis usually depends on combining:
- symptoms over time
- CT scan findings
- blood tests (including immunological tests)
- sputum microbiology
- clinical history
There is rarely a single “yes or no” test, which is why diagnosis can take time.
What the patient journey often looks like
Early symptoms
Symptoms such as cough, breathlessness, fatigue, or sputum are common across many conditions including bronchiectasis, asthma, and infection.
Treatment for common conditions
Initial treatment often includes antibiotics, inhalers, or steroids. These are appropriate first steps based on clinical guidelines such as those from the British Thoracic Society (BTS).
Ongoing symptoms
When symptoms persist or return, further investigation is usually needed.
The turning point
At some stage, fungal disease may be considered and tests for Aspergillus are performed.
Why doctors tackle common conditions first
Why do doctors start with common conditions?
Doctors treat common diseases first, prioritizing efficiency, patient safety, and high-probability outcomes. This approach, considering the most likely diagnosis first, helps manage patient health efficiently and effecctively before investigating rare or complex conditions.
This approach is safe and effective for most people, but conditions like aspergillosis can sit outside these usual pathways.
Where delays can happen
Overlap of symptoms
Symptoms overlap with many conditions, including tuberculosis and lung cancer.
No single definitive test
Diagnosis often requires combining multiple test results rather than relying on one.
Gradual disease progression
Conditions such as CPA may evolve over months or years.
Multiple conditions
Patients may have more than one lung condition at the same time.
Why this is often about the system, not the individual doctor
Healthcare systems are designed to manage large numbers of patients efficiently and safely. This means prioritising common conditions first.
However, aspergillosis often requires specialist input. In the UK, this may include referral to the National Aspergillosis Centre, which provides expert assessment and management.
International guidance from organisations such as ESCMID (European Society of Clinical Microbiology and Infectious Diseases) also highlights the complexity of fungal diseases.
What patients can do
- Keep a record of symptoms and treatments
- Ask when diagnosis should be reviewed
- Discuss whether further tests are needed
- Use trusted information sources such as our diagnosis guide
A more balanced way to think about delay
Diagnosis is often not a single event but a process that unfolds over time.
The goal is to recognise patterns earlier and ensure patients who need specialist input are identified sooner.
Common questions
Why was I treated for other conditions first?
Because those conditions are more common and more likely.
Should I ask about aspergillosis?
Yes, especially if symptoms are persistent or unusual—but it should be part of a broader discussion.
When to seek medical advice
- Persistent or worsening symptoms
- Coughing up blood
- Unexplained weight loss
References and further reading
When Symptoms Are Real but Answers Are Not: Understanding Uncertainty
Last reviewed: 18 March 2026
Key points
- Many people experience a period where symptoms are real but no clear diagnosis has been made.
- This can sometimes feel like being told “nothing is wrong” or “it is all in your head”.
- In most cases, this reflects uncertainty in the system, not disbelief from clinicians.
- Conditions such as aspergillosis can take time to become recognisable.
- Physical and psychological factors can overlap—but unexplained symptoms are still real symptoms.
- Clear communication and ongoing review are key to moving forward.
The experience many patients describe
During a long diagnostic journey, many people reach a point where they hear phrases such as:
- “Your tests are normal”
- “We can’t find anything serious”
- “It may be stress or anxiety contributing”
Even when these words are carefully chosen, they can feel like:
“Nothing is wrong” or “it’s all in my head”
This can be one of the most difficult parts of the journey—especially when symptoms are ongoing, disruptive, and clearly real.
Why this happens
This situation usually reflects the limits of current medical systems rather than a lack of concern.
Tests do not always give clear answers
Modern medicine relies heavily on tests. But for many conditions—including chronic pulmonary aspergillosis (CPA)—tests may:
- be negative early on
- show unclear or borderline results
- require interpretation over time
This creates a gap between:
- what the patient is experiencing
- what can currently be measured
Medicine is designed to provide answers
Clinicians are trained to explain symptoms and reassure patients. When no clear diagnosis is available, they may turn to explanations such as:
- stress
- anxiety
- functional symptoms
These are real and valid factors—but if introduced too early, they can feel like the search has stopped.
Time pressure
Short consultations can mean:
- less time to explain uncertainty
- less opportunity to validate patient experience
- simplified explanations that lose nuance
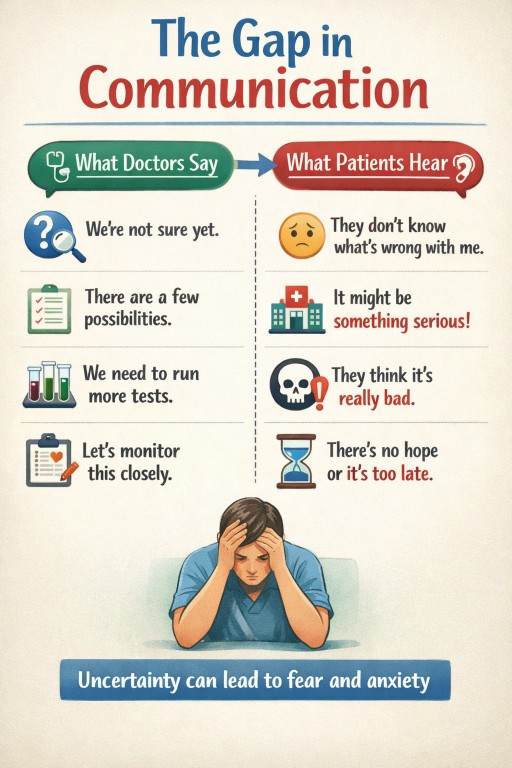
What doctors mean vs what patients hear
Often, the issue is not what is said—but how it is understood.
| What may be said | What may be heard |
|---|---|
| “Your tests are normal” | “Nothing is wrong” |
| “We haven’t found a cause yet” | “There is no cause” |
| “Stress may be contributing” | “It’s all in your head” |
Understanding this gap can help both patients and clinicians move forward more constructively.
A critical clarification
Not having a diagnosis is not the same as not having a disease.
Unexplained symptoms are still real symptoms.
Medicine does not always have immediate answers—especially for conditions that develop slowly or do not fit standard patterns.
Physical and psychological overlap
It is important to take a balanced view.
- Physical illness can lead to anxiety, fatigue, and distress
- Anxiety can worsen physical symptoms such as breathlessness
This relationship is two-way, not either/or.
The problem arises when psychological explanations replace further investigation, rather than sitting alongside it.
Why this matters in aspergillosis
Conditions such as aspergillosis often:
- develop gradually
- have non-specific symptoms
- require multiple tests over time
This makes periods of uncertainty more likely, particularly before a diagnosis such as allergic bronchopulmonary aspergillosis (ABPA) or CPA is confirmed.
You can read more about this in Why Aspergillosis Is So Hard to Diagnose.
What patients can do
- Keep a record of symptoms and how they change over time
- Ask what the current working diagnosis is
- Ask when the situation should be reviewed
- Share concerns clearly, but remain open to different explanations
Helpful questions include:
- “What else could this be?”
- “What would make you reconsider the diagnosis?”
- “When should we review this again?”
A shared understanding
This situation is not about:
- patients being dismissed
- clinicians not caring
It reflects a deeper reality:
Medicine does not always have immediate answers—especially for complex or evolving conditions.
The goal is to keep the process open, respectful, and moving forward.
Common questions
Does this mean doctors think I’m imagining symptoms?
No. It usually reflects uncertainty rather than disbelief.
Can stress really affect physical symptoms?
Yes—but this should not stop appropriate medical investigation.
What should I do if I feel dismissed?
Ask for clarification, a review plan, or a second opinion if needed.
Aspergillosis Research Highlights - Week 11
Mid-March 2026 Literature Update
This update summarises notable recent publications mentioning aspergillosis, prioritising studies relevant to chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), diagnostics, epidemiology and management.
Table of Contents
Key Highlights
- Pulmonary aspergilloma review published in CHEST: a substantial review summarises modern understanding of pulmonary aspergilloma, including diagnosis, haemoptysis risk and management.
- Rapid diagnostic technologies emerging: new CRISPR-based and LAMP molecular approaches show promise for faster identification of Aspergillus fumigatus and antifungal resistance.
- Nebulised antifungal therapy explored for ABPA: a case report describes inhaled antifungal therapy in a patient with treatment-limiting comorbidities.
- Microbiome disruption may increase susceptibility to Aspergillus infection: experimental data suggest antibiotics can impair neutrophil-mediated antifungal immunity.
- Global burden continues to emerge: recent studies again show Aspergillus infection in patients initially suspected of tuberculosis or pneumonia.
Clinical and Review Papers
Pulmonary Aspergilloma: Comprehensive Clinical Review
Seo C, Dumoulin E, Thornton CS.
Spore Wars: A Comprehensive Review of Pulmonary Aspergilloma and Its Clinical Management.
CHEST, 12 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41831523/
This review provides an updated overview of pulmonary aspergilloma, covering pathogenesis, imaging findings, haemoptysis risk and current management strategies.
- Aspergilloma develops in pre-existing lung cavities, often related to previous tuberculosis or other structural lung disease.
- The major complication is haemoptysis, which can be severe or life-threatening.
- Management may include monitoring, antifungal therapy, bronchial artery embolisation or surgical resection in selected patients.
Systematic Review Planned on ABPA Therapies
Nwankwo L, Maidment I, Periselneris J, Jackson DJ, Agarwal R, Asano K, Nuh A, Ni M, Shah A, Armstrong-James D.
Protocol for a systematic literature review and network meta-analysis of the evidence for therapies in allergic bronchopulmonary aspergillosis (ABPA).
Systematic Reviews, 11 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41814377/
This protocol sets out a planned network meta-analysis comparing therapies used in ABPA.
- Will assess the evidence for oral corticosteroids, antifungal therapy, biologics and combination approaches.
- Aims to address the continuing lack of strong comparative evidence between treatment strategies.
Diagnostics and Detection Advances
Rapid Antifungal Susceptibility Testing for Aspergillus fumigatus
Nozue S, Furuhashi K, Toguchi A, Ishikawa J, Nagura O, Yamashita K, Maekawa M, Iwaizumi M.
Rapid antifungal susceptibility testing for Aspergillus fumigatus using a loop-mediated isothermal amplification method.
Journal of Microbiological Methods, 12 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41831694/
This study describes a loop-mediated isothermal amplification (LAMP) method for rapid antifungal susceptibility testing.
- Designed to identify antifungal resistance more quickly than conventional culture-based testing.
- Potentially useful for early recognition of azole resistance.
CRISPR-Based Detection of Aspergillus fumigatus
Jiang Q, Zeng X, Zhang Q, Yang F, Lv T, Zhang Y, Wang J, Li F, Xu D.
Development and application of a rapid detection system for Aspergillus fumigatus based on ERA/CRISPR-Cas12a.
BMC Microbiology, 9 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41803678/
This paper reports a rapid molecular detection platform combining ERA amplification with CRISPR-Cas12a.
- Aims to detect A. fumigatus DNA rapidly and accurately.
- Represents the wider move toward faster molecular fungal diagnostics.
Sputum Galactomannan for Diagnosing IPA in COPD
Lan Y, Li H, Su D, Liao X, Zhang Q, Ma Q.
Clinical value of sputum galactomannan testing in the diagnosis of invasive pulmonary aspergillosis among chronic obstructive pulmonary disease patients.
European Journal of Medical Research, 9 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41803989/
This study evaluates sputum galactomannan as a less invasive diagnostic tool for invasive pulmonary aspergillosis in patients with COPD.
- Could provide useful diagnostic information when bronchoscopy is not feasible.
- May complement serum or bronchoalveolar lavage-based testing.
Immunology and Pathogenesis
Antibiotics and Susceptibility to Aspergillus Infection
Aufiero MA, Hohl TM.
Antibiotic-induced microbiota disruption impairs neutrophil-mediated immunity to respiratory Aspergillus fumigatus infection in mice.
mBio, 11 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41810941/
This experimental paper suggests that antibiotic-driven microbiome disruption can impair neutrophil responses and increase vulnerability to Aspergillus infection.
- Antibiotics altered microbial communities in ways that weakened antifungal immunity.
- The findings support a protective role for the microbiome in respiratory host defence.
Therapeutic Developments
Nebulised Antifungal Therapy in ABPA
Carrasco Sánchez M, Llopis Pastor E, García-Salmones Martín M.
Nebulised antifungal therapy in allergic bronchopulmonary aspergillosis in a patient with treatment-limiting comorbidities.
Medicina Clínica (Barcelona), 12 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41832814/
This case report describes use of nebulised antifungal therapy in ABPA where standard systemic treatment was limited by comorbidities.
- Suggests inhaled delivery may occasionally offer a practical workaround in selected patients.
- Evidence remains limited and this should still be viewed as a niche or exploratory approach.
Epidemiology and Public Health
Aspergillus Positivity in Patients With Tuberculosis-Like Symptoms
Ebong SMA, Kengne VN, Ayong MNA, Foko LPK, Ambono JLN, Ndzana GM, Baïdam MT, Youguitcha O, Abah OZA, Ayangma C, Koro FK.
Positivity rate of Aspergillus spp. in patients with tuberculosis-like symptoms in Yaoundé, Cameroon and antifungal resistance profile.
BMC Infectious Diseases, 9 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41803790/
This study found Aspergillus positivity in patients initially presenting with tuberculosis-like symptoms.
- Shows again how pulmonary aspergillosis can be confused with TB.
- Also assessed antifungal resistance patterns.
Pulmonary Fungal Infection in Pneumonia
Shokohi R, Mehraban Z, Darvishi F, Fatahinia M, Kiasat N.
Epidemiology and Clinical Features of Pulmonary Fungal Infections in Patients with Pneumonia: A Single-Center Study from Southwestern Iran.
Research Square preprint, 11 Mar 2026.
Preprint: https://www.researchsquare.com/article/rs-1164127
This preprint reports that aspergillosis was a significant component of pulmonary fungal infection among patients with pneumonia.
- Suggests fungal infection may be more common in severe respiratory disease than often recognised.
- As a preprint, findings should be interpreted cautiously until peer reviewed.
Aspergillosis in Complex Clinical Settings
Brain Abscess With Tuberculosis and Aspergillosis
Mirg S, Parihar J, Vibha D, Garg A, Singh G, Singh U, Sharma MC, Tripathi M.
Brain abscess with concurrent infection: tuberculosis and aspergillosis.
Practical Neurology, 13 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/40784749/
This case report describes a rare brain abscess caused by concurrent tuberculosis and aspergillosis.
- Illustrates the complexity of diagnosis when multiple serious infections coexist.
- Highlights the need to keep fungal infection in the differential diagnosis.
Nosocomial Aspergillus calidoustus Infection in CAR-T Cell Therapy
Aubry A, Joris M, Choquet M, Kemp H, Bigot J, Braule B, Lemonnier D, Merlin-Brochart J, Lebon D, Maizel J, Guitard J, Chouaki T.
Nosocomial invasive Aspergillus calidoustus infection in a CAR-T cell-treated patient with concomitant Aspergillus fumigatus respiratory infection.
European Journal of Clinical Microbiology & Infectious Diseases, 12 Mar 2026.
PubMed: https://pubmed.ncbi.nlm.nih.gov/41817606/
This case highlights invasive infection by the rarer species Aspergillus calidoustus in a highly immunocompromised patient.
- Occurred alongside respiratory infection with A. fumigatus.
- Emphasises the diverse Aspergillus species that may affect profoundly immunosuppressed patients.
Additional Papers Mentioning Aspergillosis
These papers mention aspergillosis but are not primarily focused on it.
- Seffar L et al. Beyond Classification: An Antineutrophil Cytoplasmic Antibody-Associated Vasculitis Overlap Case. Cureus, 14 Mar 2026. PMC: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12983185/
- Jandric M et al. Continuous Renal Replacement Therapy for Patients With Sepsis in a Low-Resource Medical Intensive Care Unit (MICU): Incidence, Risk Factors, and Outcomes. Cureus, 14 Mar 2026. PMC: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12979951/
- Koh M et al. Understanding disease burden, challenges in current treatment strategies and call for action for management of severe asthma in Asia: a position statement from Asian respiratory experts. Frontiers in Allergy, 14 Mar 2026. PMC: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12979456/
- Mustafa J et al. Phytochemical profiling of Vitex negundo seeds via UHPLC-QTOF-MS/MS analyses with antimicrobial evaluation and in silico targeting of DNA Gyrase B and Secreted Aspartic Proteinase 2 (SAP2). PLoS One, 13 Mar 2026. PubMed: https://pubmed.ncbi.nlm.nih.gov/41824429/
- Mitchelmore P, Duggan S. Candida in the lung: Fact, fiction, friend or foe? PLoS Pathogens, 10 Mar 2026. PubMed: https://pubmed.ncbi.nlm.nih.gov/41805870/
- Xie Y, Zhang A, Wang Y, Wang R. Community-Acquired Pneumonia in Patients With Diabetes: Narrative Review. JMIR Diabetes, 10 Mar 2026. PubMed: https://pubmed.ncbi.nlm.nih.gov/41805689/
- Long MB et al. Design and rationale of the AIR-NET trial: a randomised, open-label, multifactorial, multicentre, adaptive platform trial using a range of repurposed anti-inflammatory treatments to improve outcomes in patients with bronchiectasis within the EMBARC clinical research network. ERJ Open Research, 9 Mar 2026. PubMed: https://pubmed.ncbi.nlm.nih.gov/41809869/
- Zablonski KG et al. Successful allogeneic stem cell transplant in a patient with a left ventricular assist device: a novel case report. Annals of Hematology, 11 Mar 2026. PubMed: https://pubmed.ncbi.nlm.nih.gov/41807548/
- He D et al. Amphotericin B promotes respiratory viral entry by enhancing late endosomal maturation and fusion via glucocerebrosidase-mediated ceramide remodeling. Nature Communications, 9 Mar 2026. PubMed: https://pubmed.ncbi.nlm.nih.gov/41803143/
Overall Trends
- Rapid molecular diagnostics for Aspergillus detection and resistance testing continue to advance.
- Global awareness of fungal lung disease is improving, especially in patients initially thought to have tuberculosis or bacterial pneumonia.
- Host immunity and microbiome research is expanding understanding of why some patients become vulnerable to Aspergillus disease.
- Alternative treatment approaches, such as inhaled antifungal therapy, are being explored in selected difficult cases.
Clinical Trials and Emerging Treatments for Chronic Aspergillosis
Last reviewed: 12 March 2026
Key points
- Only a small number of antifungal drug classes are currently available to treat aspergillosis.
- New treatments are needed because of drug resistance, side effects, drug interactions and the long-term burden of chronic disease.
- Research is now exploring not only new antifungal drugs, but also inhaled therapies, biologics, immune-modulating treatments and combination approaches.
- Most new drugs are first tested in invasive aspergillosis before being studied in chronic pulmonary aspergillosis (CPA) or allergic bronchopulmonary aspergillosis (ABPA).
- Clinical trials are essential for showing whether new treatments are safe and effective.
Table of contents
- Overview
- Why new treatments are needed
- How new treatments are developed
- Clinical trial phases
- Regulatory approval and NHS use
- New antifungal drugs in development
- Other emerging treatments for chronic aspergillosis
- Why new treatments are often tested in invasive aspergillosis first
- How to find clinical trials
- Common questions
- Further information
- Author and review information
Overview
Treatment options for aspergillosis have improved over time, but there are still important limitations. Only a small number of antifungal drug classes are available, some fungi develop resistance to existing medicines, and some patients cannot tolerate treatment because of side effects or drug interactions.
This is particularly important in chronic aspergillosis, where treatment may need to continue for months or years. Research is therefore focused not only on new antifungal drugs, but also on better drug delivery systems, immune-based treatments, biologic therapies and combinations of treatments.
Clinical trials are the main way that researchers test whether these new approaches are safe and effective.

Why new treatments are needed
New treatments for chronic aspergillosis are needed for several reasons:
- the number of available antifungal drug classes is limited,
- Aspergillus can develop resistance to azole antifungals,
- some patients experience significant side effects or important drug interactions,
- long-term treatment can be difficult to sustain,
- chronic disease may continue to affect symptoms, lung function and quality of life even when treatment is helping.
Because chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA) and related conditions can behave differently, researchers are exploring a wider range of therapies than in the past.
How new treatments are developed
Before a new treatment can be used routinely, it must pass through several stages of development.
| Stage | Description |
|---|---|
| Basic research | Scientists study the disease and identify targets that could be affected by a new drug or treatment approach. |
| Drug discovery | Researchers screen chemical compounds or modify promising molecules to find potential treatments. |
| Pre-clinical studies | Potential treatments are tested in laboratory systems and sometimes animal models to assess activity and safety. |
| Application to begin human trials | Researchers apply to regulators and ethics committees for permission to test the treatment in people. |
Clinical trial phases
Clinical trials are usually carried out in phases.
| Phase | Purpose |
|---|---|
| Phase 0 / Phase I | Small studies, often in healthy volunteers, to understand how the treatment behaves in the body, including absorption, distribution and safe dose ranges. |
| Phase II | Studies in patients with the disease to identify useful doses and gather early information on effectiveness and side effects. |
| Phase III | Larger studies comparing the new treatment with existing care to assess effectiveness and safety more accurately. |
| Phase IV | Post-marketing studies that monitor how the treatment performs in real-world use after approval. |
Regulatory approval and NHS use
If a treatment performs well in trials, the manufacturer can apply for approval from a medicines regulator such as the European Medicines Agency (EMA) or the U.S. Food and Drug Administration (FDA).
In the United Kingdom, a treatment may also be assessed by the National Institute for Health and Care Excellence (NICE) to determine whether it should be funded for routine use in the NHS.
Even when a drug is not recommended for routine NHS use, doctors may sometimes apply for individual funding if they believe it could benefit a particular patient.
New antifungal drugs in development
Many new antifungal drugs are first developed for severe invasive fungal infections and may later be studied in chronic conditions such as CPA or ABPA.
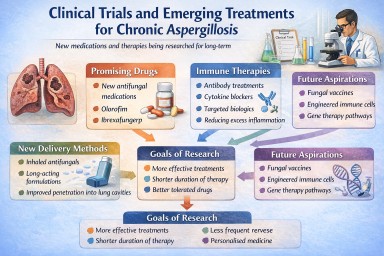
Olorofim
Olorofim is a novel antifungal from a completely new class called the orotomides. It targets fungal pyrimidine synthesis, a pathway not affected by current azole, echinocandin or polyene antifungals.
Rezafungin
Rezafungin is an echinocandin designed to have a longer duration of action and improved pharmacokinetic properties compared with older drugs in the same class.
Ibrexafungerp
Ibrexafungerp belongs to a new group of antifungals called triterpenoids. It acts on fungal cell wall synthesis in a way that is similar to echinocandins, but its structure is different and it can be given orally.
Fosmanogepix
Fosmanogepix is a first-in-class antifungal that blocks production of a molecule needed for fungal cell wall construction and self-regulation.
Oteseconazole
Oteseconazole is one of the newer tetrazole agents designed to improve selectivity and reduce side effects compared with traditional azoles.
Encochleated Amphotericin B
This is a reformulated version of amphotericin B designed to improve delivery and reduce toxicity.
ATI-2307
ATI-2307 is an arylamidine antifungal that interferes with mitochondrial function in fungal cells.
Other emerging treatments for chronic aspergillosis
Although new antifungal drugs are an important area of research, scientists are also exploring other ways to treat chronic forms of aspergillosis such as chronic pulmonary aspergillosis (CPA) and allergic bronchopulmonary aspergillosis (ABPA). These approaches aim to improve treatment effectiveness, reduce side effects, or target the immune response to the fungus.
Inhaled antifungal treatments
One area of research is the development of antifungal medicines that can be delivered directly to the lungs using inhalers or nebulisers. Delivering medication directly to the lungs may allow higher drug concentrations at the site of disease while reducing side effects elsewhere in the body.
Examples being explored include inhaled or nebulised formulations of amphotericin B, itraconazole and voriconazole.
Immune-modulating therapies
In some patients with aspergillosis, the immune response to the fungus plays an important role in how the disease develops or persists. Researchers are studying treatments that help modify the immune response rather than directly killing the fungus.
Examples include therapies that may enhance antifungal immunity or reduce harmful inflammation.
Biologic therapies
Biologic drugs that target specific immune pathways are already used to treat severe asthma and allergic disease. Some of these medicines are now being studied or used in fungal-related airway disease.
Examples include drugs targeting immunoglobulin E (IgE) or eosinophilic inflammation, such as omalizumab, mepolizumab, benralizumab, dupilumab and tezepelumab. These may be particularly relevant in ABPA or severe asthma with fungal sensitisation (SAFS).
Combination therapies
Future treatment strategies may combine different approaches, for example antifungal medication together with biologic therapy, inhaled therapy or immune-modulating treatment. Combination treatment may improve outcomes in patients whose disease does not respond fully to a single treatment alone.
Research is ongoing to determine which combinations are most effective and safest for patients with chronic aspergillosis.
Why new treatments are often tested in invasive aspergillosis first
Many new antifungal drugs are first tested in patients with invasive aspergillosis before being studied in chronic forms of the disease such as chronic pulmonary aspergillosis (CPA) or allergic bronchopulmonary aspergillosis (ABPA).
There are several reasons for this:
- Disease progression is faster. In invasive infections the illness progresses quickly, so researchers can more easily measure whether a new treatment is working.
- Clearer treatment outcomes. Invasive infections often have well-defined clinical outcomes such as survival or clearance of infection.
- Smaller studies can provide useful results. Because invasive infections are severe, treatment effects may be detected in smaller numbers of patients.
Chronic forms of aspergillosis usually progress more slowly. This means clinical trials often need to run for longer periods and include larger numbers of patients to demonstrate whether a treatment is effective.
Once a new antifungal drug has shown benefit in invasive disease, researchers may then study how it performs in chronic conditions such as CPA or ABPA.
Specialist centres such as the National Aspergillosis Centre contribute to research that helps evaluate new treatments for chronic forms of aspergillosis and improve care for patients living with these conditions.
How to find clinical trials
Clinical trials involving human participants must be registered publicly for ethical and regulatory reasons.
You can search for ongoing or completed studies at:
This database allows you to search for studies by disease, location, treatment or trial status.
Not all studies test new drugs. Some trials investigate diagnostics, biomarkers, new ways of using existing medicines, or observational registries that help researchers understand disease patterns over time.
If you are interested in taking part in a clinical trial, discuss this with your specialist respiratory team.
Common questions
Why are new treatments needed if antifungal drugs already exist?
Current antifungal drugs help many patients, but they do not work for everyone. Some fungi develop resistance, some patients experience side effects or interactions, and chronic disease can remain difficult to control.
Are all new treatments new antifungal drugs?
No. Research now includes new antifungal drugs, inhaled treatments, biologics, immune-modulating therapies and combination approaches.
Why are there more trials in invasive aspergillosis than CPA?
Invasive aspergillosis progresses more quickly, so trial results can often be measured sooner and with fewer patients. CPA usually changes more slowly, which makes trials longer and more difficult to run.
Can patients with chronic aspergillosis join clinical trials?
Sometimes, yes. Eligibility depends on the trial design, the type of aspergillosis, previous treatment and other health factors. Your specialist team can advise whether there may be suitable studies.
Do clinical trials always involve testing a completely new drug?
No. Some studies test new doses, new combinations, new formulations such as inhaled treatment, or new diagnostic approaches.
Further information
You may find these pages helpful:
- Antifungal medicines for aspergillosis
- Biologics and eosinophilic asthma
- Inhalers and nebulisers
- Chronic pulmonary aspergillosis (CPA)
- Allergic bronchopulmonary aspergillosis (ABPA)
More information about the medicine development process can be found through major medicines regulators, clinical trial registries, and specialist respiratory teams.
Author and review information
Author: Aspergillosis Website Editorial Team
Audience: Patients, carers, GPs and non-specialists
Last reviewed: 12 March 2026

Clinical Trials and Emerging Diagnostics for Aspergillus Infections
How new diagnostic technologies may improve detection of Aspergillus lung infections
Last reviewed: March 2026
Author: Graham Atherton
Key points
- Diagnosing Aspergillus lung infections can be challenging because symptoms often resemble other lung diseases.
- Doctors usually combine CT scans, blood tests and microbiology tests to make a diagnosis.
- Researchers are developing new diagnostics that detect fungal DNA, fungal molecules, or drug-resistant strains.
- Emerging tools include PCR tests, antigen detection, rapid tests, sequencing technologies and artificial intelligence imaging.
- This page focuses on Aspergillus infections rather than allergic conditions such as Allergic Bronchopulmonary Aspergillosis, Severe Asthma with Fungal Sensitisation, or Aspergillus bronchitis.
- Many of these newer technologies are being studied in clinical trials and research programmes worldwide.
Table of contents
- 1. Important note: infection vs allergy
- 2. Why better diagnostics are needed
- 3. How Aspergillus infections are diagnosed today
- 4. Detecting the immune response vs detecting the fungus
- 5. Simple diagram: two ways of looking for Aspergillus disease
- 6. DNA testing (PCR diagnostics)
- 7. Fungal antigen detection
- 8. Rapid diagnostic tests
- 9. Breath diagnostics
- 10. Sequencing technologies and the lung microbiome
- 11. Detecting antifungal resistance
- 12. Artificial intelligence and CT imaging
- 13. Flowchart: how doctors diagnose chronic Aspergillus infection
- 14. The future diagnostic pathway
- 15. Common questions patients ask
- 16. When to seek medical advice
- 17. References
1. Important note: infection vs allergy
This article focuses on diagnosing Aspergillus infections of the lungs, particularly:
- Chronic Pulmonary Aspergillosis
- Aspergillus nodules
- Aspergilloma (fungal ball)
- Subacute invasive aspergillosis
These conditions involve the fungus growing in lung tissue or in pre-existing lung cavities.
This is different from allergic Aspergillus disease, such as:
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Severe Asthma with Fungal Sensitisation (SAFS)
- Aspergillus bronchitis (which overlaps with airway disease rather than the classic cavity-forming infections discussed here)
In allergic disease, diagnosis focuses more on immune reactions, such as IgE antibodies, eosinophils, allergy testing and markers of Type 2 inflammation.
This page therefore focuses mainly on diagnostics for Aspergillus infection rather than allergy. A separate article can cover immune diagnostics in allergic Aspergillus disease.
2. Why better diagnostics are needed
Chronic Pulmonary Aspergillosis often develops in people who already have damaged lungs, for example from:
- tuberculosis
- Chronic Obstructive Pulmonary Disease
- bronchiectasis
- sarcoidosis
- previous severe lung infections
- lung surgery
Symptoms may include:
- chronic cough
- breathlessness
- fatigue
- weight loss
- coughing up blood
- chest discomfort
These symptoms are not specific, meaning they can occur in many other lung diseases.
Aspergillus is also very common in the environment, so detecting it in sputum does not always mean it is causing disease. Sometimes it may simply be present without invading tissue or causing progressive damage.
For these reasons, diagnosing chronic aspergillosis usually requires multiple tests interpreted together, rather than relying on one result alone.
3. How Aspergillus infections are diagnosed today
Doctors usually combine three main types of evidence.
| Diagnostic method | What it shows |
|---|---|
| CT scan | Structural lung changes such as cavities, nodules or fungal balls |
| Blood tests | The body's immune response to Aspergillus |
| Microbiology tests | Evidence of the fungus itself |
The most important blood test for many patients with Chronic Pulmonary Aspergillosis is Aspergillus IgG antibodies.
CT scans are also critical because they can reveal features such as:
- lung cavities
- fungal balls
- nodules
- thickened cavity walls
- progressive lung destruction or scarring
Microbiology may include sputum culture, bronchoscopy samples, microscopy, molecular testing and antigen detection.
No single test is perfect. Doctors usually look at the whole picture: symptoms, scan findings, blood tests, microbiology, and how things change over time.
4. Detecting the immune response vs detecting the fungus
Some diagnostic tests detect how the body reacts to Aspergillus, while others try to detect the fungus itself.
Immune response tests
Examples include:
- Aspergillus IgG antibodies
- general inflammatory markers
These tests show that the immune system has encountered Aspergillus, but they do not always prove that the fungus is currently active, growing, or causing ongoing damage.
Direct fungal detection
Other tests look for components of the fungus itself.
| Test | What it detects |
|---|---|
| PCR | Aspergillus DNA |
| Galactomannan | Fungal cell wall molecules |
| Beta-D-glucan | Fungal structural components |
| Culture | Growth of the fungus in the laboratory |
These tests can sometimes provide more direct evidence that fungal material is present.
Why not rely only on the immune response?
Immune-response tests are extremely useful, but they are indirect. They tell us what the body is doing, not necessarily what the fungus is doing at that moment.
Antibodies may remain raised for quite a long time, may change only slowly, and may vary from person to person. Some patients also produce weaker immune responses than others.
By contrast, tests that detect fungal DNA or fungal cell wall components may sometimes give a better sense that fungal material is actually present in the lungs.
The footprints analogy
A useful way to understand this difference is:
- Immune response tests are like seeing footprints in the snow – they show that someone has been there.
- Direct fungal tests are like seeing the person themselves – they show that the organism is present.
In practice, doctors usually combine both kinds of evidence to make the diagnosis more reliable.
5. Simple diagram: two ways of looking for Aspergillus disease
Two broad diagnostic approaches
| Approach | Examples | Main question |
|---|---|---|
| Looking for the body's response | Aspergillus IgG, inflammation markers | Has the immune system reacted to Aspergillus? |
| Looking for the fungus itself | PCR, galactomannan, Beta-D-glucan, culture | Is fungal material present? |
| Looking for damage caused in the lungs | CT scan | Has Aspergillus or another disease caused structural lung change? |
This is why diagnosis is usually based on a combination of evidence rather than any single test.
6. DNA testing (PCR diagnostics)
Polymerase Chain Reaction, usually shortened to PCR, detects the DNA of Aspergillus fungi.
These tests can be performed on samples such as:
- sputum
- bronchoscopy samples
- lung tissue
Advantages of PCR include:
- faster results than fungal culture
- detection of very small amounts of fungus
- possible detection even when cultures are negative
However, PCR also has challenges. It may detect fungal material even when it is not clearly causing disease, and methods are not yet fully standardised across all laboratories.
Even so, PCR is one of the most important emerging tools in fungal diagnostics and is increasingly used in specialist centres.
7. Fungal antigen detection
Some tests look for molecules released by fungal cells. These are often called antigen tests.
Galactomannan
Galactomannan is a molecule found in the cell wall of Aspergillus.
It is already widely used in diagnosing invasive aspergillosis and is being studied more closely in chronic forms of disease as well.
Beta-D-glucan
Beta-D-glucan is a structural component found in the cell walls of many fungi.
Raised levels can suggest fungal infection somewhere in the body, although it is not specific for Aspergillus alone.
Researchers are interested in how these markers might be used alongside CT, antibody testing and PCR to improve accuracy.
8. Rapid diagnostic tests
Researchers are also developing rapid antigen tests that can detect fungal molecules within minutes.
These tests work in a similar way to a simple strip test and may offer:
- quick results
- minimal laboratory equipment
- possible use in clinics with fewer resources
These tests are promising, but they still need careful evaluation to show how accurate and reliable they are in real patients with chronic Aspergillus disease.
9. Breath diagnostics
Fungi release small chemicals called volatile organic compounds. Some experimental devices aim to detect these compounds in exhaled breath.
If successful, breath testing could provide:
- completely non-invasive testing
- rapid screening
- repeat testing over time without invasive procedures
This remains an early and experimental field, but it is attractive because it could make testing much easier for patients.
10. Sequencing technologies and the lung microbiome
Modern sequencing technologies can analyse all microbial DNA in a sample.
This means they may identify:
- fungi
- bacteria
- viruses
These approaches may help doctors understand mixed infections and the broader lung microbiome, especially in people with bronchiectasis or complex chronic lung disease.
In the future, sequencing may help explain why some patients have persistent symptoms or repeated flares involving more than one organism.
11. Detecting antifungal resistance
Some strains of Aspergillus fumigatus have developed resistance to azole antifungal drugs.
Newer diagnostic tests can detect genetic mutations linked to drug resistance, especially in the CYP51A gene.
Earlier detection of resistance could help doctors:
- choose effective antifungal drugs sooner
- avoid ineffective treatment
- improve long-term outcomes
This is an important area of research because antifungal resistance is a growing international concern.
12. Artificial intelligence and CT imaging
Artificial intelligence is increasingly being explored as a way to analyse CT scans more precisely.
These systems may eventually help doctors:
- detect subtle lung changes earlier
- measure cavity size or progression more consistently
- monitor disease over time
- compare scans more accurately
Artificial intelligence is unlikely to replace expert radiologists or specialist teams, but it may become a useful support tool.
13. Flowchart: how doctors diagnose chronic Aspergillus infection
Typical diagnostic pathway
Symptoms
persistent cough, breathlessness, fatigue, weight loss, coughing up blood
↓
CT scan
looking for cavities, fungal balls, nodules, scarring or progressive damage
↓
Blood tests
especially Aspergillus IgG and general inflammatory markers
↓
Microbiology
sputum, bronchoscopy, culture, PCR, antigen tests
↓
Clinical interpretation
combining symptoms, imaging, blood tests and microbiology
↓
Diagnosis and follow-up
deciding whether this is infection, colonisation, another lung condition, or mixed disease
This flowchart is simplified, but it shows the basic principle: diagnosis depends on combining evidence.
14. The future diagnostic pathway
In the future, diagnosing Aspergillus infection may involve several rapid tests used together.
A possible pathway could look like this:
Symptoms → CT scan → fungal antigen test → PCR confirmation → resistance testing
This approach could allow:
- faster diagnosis
- more personalised treatment
- earlier detection of complications
- better treatment monitoring
The aim is not necessarily to replace older tests, but to make the whole diagnostic process earlier, clearer and more precise.
15. Common questions patients ask
Why can Aspergillus infection take time to diagnose?
Because no single test can confirm the disease on its own. Doctors usually need to combine scan findings, blood tests, microbiology and the clinical history.
Why do some tests detect antibodies while others detect the fungus?
Antibody tests show how the immune system has reacted. Molecular and antigen tests try to show whether fungal material is present. Both are useful, but they answer slightly different questions.
Why is a CT scan so important?
A CT scan shows whether there is structural lung damage such as cavities, nodules or fungal balls. This helps doctors judge whether Aspergillus is likely to be causing disease rather than simply being present.
Are these new diagnostics available now?
Some are already used in specialist centres, but many are still being evaluated in clinical trials and research studies.
Will these newer tests replace existing blood tests?
Probably not completely. More likely, they will be used alongside existing tests to improve accuracy and speed.
16. When to seek medical advice
You should seek medical advice if you have symptoms such as:
- persistent cough
- worsening breathlessness
- unexplained fatigue
- weight loss
- coughing up blood
- new or worsening chest pain
These symptoms can have many causes, but they should be assessed properly, especially if you already have underlying lung disease.
17. References
- Denning DW, Cadranel J, Beigelman-Aubry C, Ader F, Chakrabarti A, Blot S, Ullmann AJ, Dimopoulos G, Lange C; European Society for Clinical Microbiology and Infectious Diseases and European Respiratory Society. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J. 2016 Jan;47(1):45-68. doi: 10.1183/13993003.00583-2015. PMID: 26699723.
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015 Mar;70(3):270-7. doi: 10.1136/thoraxjnl-2014-206291. Epub 2014 Oct 29. PMID: 25354514.
- Takazono T, Izumikawa K. Recent Advances in Diagnosing Chronic Pulmonary Aspergillosis. Front Microbiol. 2018 Aug 17;9:1810. doi: 10.3389/fmicb.2018.01810. PMID: 30174658; PMCID: PMC6107790.
Author and review information
This page is intended for patients, carers, and non-specialist clinicians. It provides general educational information and should not replace individual medical advice.

Managing fatigue and energy in aspergillosis and allergic fungal lung disease
Key points
- Many people with aspergillus-related lung conditions experience extreme tiredness after physical or mental exertion.
- This fatigue can last hours or even several days.
- Breathing, immune activity, inflammation and sometimes hormone imbalance all use extra energy.
- Activity can temporarily increase airway inflammation and mucus.
- Managing energy carefully (“spoon theory”) can help prevent fatigue crashes.
Contents
- Why people with lung disease feel exhausted after exertion
- What is happening in the lungs and body
- Managing energy: the “spoon theory”
- Practical ways to manage energy
- Nutrition and adrenal health
- Warning signs you are running out of energy
- Why fatigue in lung disease is different from normal tiredness
- Daily energy management checklist
- Can this fatigue be treated?
- When to talk to your doctor
Why people with lung disease feel exhausted after exertion
Healthy lungs have a large reserve capacity. When we exercise or do physical work, breathing becomes deeper and faster, but the lungs can usually cope easily.
In people with aspergillosis or allergic airway disease, the airways may already be:
- inflamed
- narrowed
- filled with mucus
- sensitive to allergens such as Aspergillus fumigatus
When the body demands more oxygen during activity, the lungs must work much harder to supply it. Activities that seem minor to other people may therefore require much greater effort from the body.
What is happening in the lungs and body?
Inflamed airways
Many aspergillus-related conditions involve inflammation in the airways. The immune system releases chemicals that cause:
- swelling of airway walls
- increased mucus production
- greater airway sensitivity
During exertion, breathing becomes faster and deeper, which can irritate these inflamed airways further.
Mucus affecting airflow
Inflamed airways often produce extra mucus. This mucus can partly block airflow and lead to:
- coughing
- wheezing
- breathlessness
- uneven airflow within the lungs
This may reduce how efficiently oxygen enters the bloodstream. Doctors sometimes refer to this as ventilation–perfusion mismatch.
Breathing uses more energy
In healthy people, breathing uses only a small fraction of the body's energy. In lung disease, breathing may require much more effort.
Additional muscles may assist breathing, including:
- chest muscles
- neck muscles
- shoulder muscles
These muscles can become fatigued during activity, just like leg muscles after exercise.
Immune system activity
If the immune system reacts to fungal proteins or allergens, it releases signalling chemicals called cytokines. These chemicals can produce symptoms similar to mild illness, including fatigue, brain fog and muscle aches.
Delayed inflammation after activity
Some people notice that fatigue appears later rather than immediately. Physical effort can trigger inflammation that develops over 12–48 hours, increasing mucus production, airway irritation and tiredness.
This explains why people sometimes feel worse the day after a busy day.
Managing energy: the “spoon theory”
Many people with chronic illness find it helpful to think about their energy using the idea of spoon theory.
In this idea:
- each spoon represents a small unit of energy
- you start the day with a limited number of spoons
- each activity uses some of those spoons
Because breathing and inflammation already use energy, people with lung disease may begin the day with fewer spoons available.
Example of spoon use
| Activity | Possible energy use |
|---|---|
| Getting dressed | 1 spoon |
| Showering | 2–3 spoons |
| Cooking a meal | 2 spoons |
| Doctor’s appointment | 3–4 spoons |
| Busy social day | Many spoons |
If too many spoons are used early in the day, the body may run out of energy, leading to exhaustion lasting hours or even days.
Practical ways to manage energy
Plan activities around your best time of day
| Time of day | Suggested activities |
|---|---|
| Morning | Errands or appointments |
| Midday | Light household tasks |
| Afternoon | Quieter activities |
| Evening | Rest and recovery |
Break tasks into smaller steps
Large tasks can overwhelm the lungs and muscles. Instead of doing everything at once:
- clean one room at a time
- cook in stages
- prepare things earlier in the day
Use the 50–70% rule
Try to stop activity when you reach about half to two-thirds of your limit. Stopping early often prevents the fatigue crash that can occur later.
Use breathing techniques
Pursed-lip breathing
- breathe in through your nose
- breathe out slowly through gently pursed lips
Rhythmic breathing
Match breathing with movement, for example when climbing stairs.
Keep mucus moving
Mucus increases the work of breathing. Helpful strategies include:
- airway clearance techniques
- staying well hydrated
- gentle movement
- using inhalers or nebulisers as prescribed
Maintain gentle regular activity
Although exertion can cause fatigue, complete inactivity can worsen the problem. Gentle activity such as walking or pulmonary rehabilitation exercises helps maintain muscle strength.
Protect sleep
- maintain a regular sleep routine
- clear mucus before bedtime if needed
- avoid heavy exertion late in the evening
Nutrition and adrenal health
Nutrition and energy
Good nutrition helps support energy levels. Helpful strategies include:
- eating regular meals
- including protein for muscle repair (eggs, fish, dairy, beans or nuts)
- eating complex carbohydrates for steady energy
- drinking enough fluids
Some people find that smaller, more frequent meals reduce breathlessness compared with large meals.
Important nutrients
- protein
- vitamin D
- iron
- B vitamins
Doctors may check for deficiencies if fatigue is severe.
Adrenal insufficiency
Some patients who have taken long-term steroid medications may develop adrenal insufficiency. The adrenal glands normally produce cortisol, which helps regulate energy and stress responses.
Symptoms may include:
- severe fatigue
- dizziness
- muscle weakness
- difficulty recovering after exertion
Patients with adrenal insufficiency usually take hydrocortisone replacement therapy and should follow their doctor’s advice carefully.
Warning signs you are running out of energy
- breathing becomes faster or more difficult
- increased coughing or mucus
- arms or legs feel heavy
- dizziness or weakness
- difficulty concentrating
- chest tightness or wheezing
When these warning signs appear, it is usually best to stop and rest before continuing.
Why fatigue in lung disease is different from normal tiredness
Fatigue in lung disease is not simply normal tiredness. Several factors occur at the same time:
- breathing requires more energy
- the immune system may be active
- oxygen exchange may be less efficient
- nutrition and hormone balance may influence recovery
Because of this combination, fatigue may appear suddenly and last longer than expected.
Daily energy management checklist
Pacing and activity
- spread activities across the day
- stop before exhaustion
- plan demanding tasks when energy is highest
- allow recovery time after busy days
Breathing and airway care
- use breathing techniques during exertion
- perform airway clearance if needed
- take inhalers or nebulisers as prescribed
- stay well hydrated
Nutrition and medication
- eat regular meals
- include protein for muscle strength
- take medications as prescribed
- follow sick-day rules if you have adrenal insufficiency
Sleep and recovery
- maintain a regular sleep routine
- clear mucus before bedtime
- rest when warning signs appear
Can this fatigue be treated?
Fatigue associated with aspergillosis, allergic fungal airway disease, or severe asthma can sometimes be improved when the underlying causes are treated. Because several different processes contribute to fatigue, treatment usually focuses on improving multiple factors rather than a single cure.
Treating airway inflammation
Inflammation in the airways is one of the major contributors to fatigue. When the airways are inflamed:
- breathing requires more effort
- mucus production increases
- oxygen exchange becomes less efficient
Treatments aimed at reducing airway inflammation may include:
- Inhaled corticosteroids – commonly used in asthma to reduce inflammation directly in the airways.
- Antifungal therapy – in some patients, reducing fungal growth can reduce immune activation and inflammation.
- Biologic therapies – newer treatments that target specific immune pathways involved in allergic and inflammatory lung disease.
Biologic treatments
Biologics are one of the most promising areas of treatment for severe asthma and allergic airway disease. These medications target specific parts of the immune system that drive inflammation.
| Biologic | Target | Effect |
|---|---|---|
| Omalizumab | IgE | Reduces allergic inflammation |
| Mepolizumab / Benralizumab | IL-5 pathway | Reduces eosinophilic inflammation |
| Dupilumab | IL-4 / IL-13 | Reduces type-2 inflammation |
| Tezepelumab | TSLP | Blocks upstream inflammatory signalling |
Some patients with conditions such as allergic bronchopulmonary aspergillosis (ABPA) or severe asthma report improvements in breathlessness, symptoms and overall energy levels when inflammation is better controlled.
Improving mucus clearance
Mucus in the airways increases the work of breathing and can contribute to fatigue. Strategies that may help include:
- airway clearance techniques
- physiotherapy
- maintaining good hydration
- using prescribed inhalers or nebulisers correctly
Treating other contributing factors
Fatigue can also be worsened by other health issues that are common in chronic lung disease, such as:
- iron deficiency
- vitamin deficiencies
- poor sleep
- adrenal insufficiency
- muscle deconditioning
Addressing these factors can sometimes improve overall energy levels.
Pulmonary rehabilitation
Pulmonary rehabilitation programmes combine exercise training, breathing techniques and education about pacing activities. These programmes can improve muscle efficiency and exercise tolerance, and many patients report reduced fatigue and improved quality of life.
Future treatments
Research into inflammatory lung diseases is advancing rapidly. New biologic drugs and other targeted therapies are being developed that may improve control of airway inflammation.
Researchers are also studying how the lung microbiome (bacteria and fungi living in the airways) influences inflammation. In the future, this may lead to more personalised treatments for patients with fungal-related lung disease.
Inflammatory fatigue
Researchers are increasingly recognising that chronic inflammatory diseases can cause a form of fatigue sometimes called “inflammatory fatigue.”
In these conditions, immune signalling chemicals released during inflammation can affect the brain and energy metabolism. Similar patterns of fatigue are seen in diseases such as rheumatoid arthritis and inflammatory bowel disease.
This may help explain why some treatments that reduce inflammation — including biologic therapies — can improve fatigue even when lung function measurements change only modestly.
Interrupting the fatigue cycle
Treatment aims to interrupt the cycle that can develop in chronic lung disease:
Airway inflammation
↓
Breathing requires more effort
↓
More energy used by respiratory muscles
↓
Immune system activity
↓
Reduced overall energy and fatigue
By improving airway inflammation, mucus clearance, muscle strength and overall health, many patients find their energy levels become more manageable.
When to talk to your doctor
Seek medical advice if:
- fatigue becomes progressively worse
- breathlessness increases
- new symptoms appear such as chest pain or coughing up blood
- fatigue prevents normal daily activities
A reassuring message
Many people with aspergillosis or allergic airway disease worry that exhaustion means their condition is worsening.
In most cases it reflects the extra energy required for breathing, inflammation and immune activity. Learning to pace activity can help people live more comfortably with chronic lung disease.
Author: National Aspergillosis Centre information team
Review: Clinical review recommended
Last reviewed: 2026