Mould, “Toxins” and Aspergillus: Understanding What’s True and What Isn’t
Last reviewed: April 2026
Key points
- Exposure to mould is not the same as having aspergillosis.
- Aspergillus is a common environmental fungus that most people inhale daily.
- “Mycotoxin” and “detox” explanations are common online but are not part of standard diagnosis.
- Symptoms usually arise from a combination of lung disease, infection, inflammation, and environment.
- Diagnosis relies on clinical tests (scans, blood tests, microbiology), not environmental testing alone.
- Specialist home testing is sometimes used—but only in specific clinical situations.
A guide for patients and carers
Many people with lung conditions come across information linking mould exposure, toxins, and Aspergillus infections. Some of this information can be helpful—but much of it can also be confusing.
This article explains the most common misunderstandings and what current medical practice actually relies on.
Important: Some tests measure exposure—but medical diagnosis requires evidence of disease.
Contents
- Why this topic is confusing
- Mould exposure vs Aspergillus disease
- Mycotoxins and “detox” claims
- Why “mould toxin tests” are not used diagnostically
- Why symptoms don’t have one single cause
- How Aspergillus conditions are actually diagnosed
- When home testing may be used
- What matters most for patients
Why this topic is confusing
- Mould is visible and easy to focus on
- Symptoms (fatigue, cough, breathlessness) are non-specific
- Online information often mixes different conditions together
This can lead to the idea that one single cause—such as “mould toxicity”—explains everything. In practice, respiratory conditions are usually more complex.
Mould exposure vs Aspergillus disease
Mould exposure
- Common in homes and outdoor air
- Can irritate airways
- May worsen symptoms
Aspergillus disease
- Occurs in specific medical contexts
- Related to lung structure and immune response
- Requires clinical diagnosis
Important context: Aspergillus spores are present in the air we breathe every day. Most people inhale them without developing disease.
Mycotoxins and “detox” claims
You may see references to:
- “Mycotoxin illness”
- “Die-off reactions”
- “Binders” to remove toxins
These ideas are widely discussed online, but they are not part of standard medical diagnosis or treatment for Aspergillus lung conditions.
This does not mean symptoms are not real. It means they are usually explained through:
- Inflammation
- Infection
- Underlying lung disease
Why “mould toxin tests” are not used diagnostically
Exposure is common
Many people have detectable environmental exposure, so results are not specific.
Results do not match symptoms reliably
Levels do not consistently correlate with disease or severity.
Lack of standardisation
Different labs use different methods, making interpretation difficult.
Not part of clinical guidelines
Major respiratory guidelines do not include these tests in diagnosing Aspergillus conditions.
Risk of confusion
- May cause unnecessary concern
- May lead to unproven treatments
Why symptoms don’t have one single cause
Symptoms often arise from a combination of:
- Underlying lung disease
- Inflammation
- Infection (fungal or bacterial)
- Environmental triggers (pollution, damp)
This is why symptoms can fluctuate and may not respond to a single explanation or treatment.
How Aspergillus conditions are actually diagnosed
Diagnosis is based on a combination of:
- CT imaging
- Blood tests (e.g. IgE, IgG)
- Microbiology (sputum or bronchoscopy)
Environmental testing alone is not sufficient to diagnose disease.
When home testing may be used
In some cases, specialist teams (for example via the Mycology Reference Centre Manchester) may arrange targeted environmental sampling.
This is different from commercial testing and focuses on:
- Specific clinically relevant fungi (e.g. Aspergillus species)
- Known allergens or pathogens
Why it is done
- Established Aspergillus-related disease
- Unexplained or persistent symptoms
- Concern about ongoing exposure
This testing is used to answer specific clinical questions and is interpreted alongside medical findings.
What matters most for patients
- Work with your clinical team for diagnosis and treatment
- Address damp and mould in your home
- Focus on practical steps that improve symptoms
- Avoid relying on a single explanation for complex symptoms
Final takeaway
Mould, environment, and Aspergillus are connected—but not in a simple cause-and-effect way.
Understanding this helps you focus on what is most likely to improve your health: appropriate treatment, good living conditions, and ongoing monitoring.
Author: aspergillosis.org
Note: Educational content only – not medical advice.
Indoor Air Quality, Damp, Mould and Aspergillus
Last reviewed: April 2026
Key points
- Indoor air problems usually relate to pollution, damp, or mould—these are different but can overlap.
- Aspergillus is a normal part of the environment and not automatically a sign of a problem indoors.
- Damp and mould can worsen breathing symptoms and should be taken seriously.
- Fixing the underlying moisture problem is more important than cleaning visible mould.
- Knowing who to contact (GP, landlord, council) is key to resolving problems.
Indoor Air Quality, Damp, Mould and Aspergillus
A practical guide for patients
Many people with aspergillosis or other lung conditions are concerned about the air inside their home. This article explains how indoor air quality works, how to recognise problems, and what steps you can take to improve your environment.
Contents
- What affects indoor air?
- Three common problems
- Aspergillus in the home
- Damp and mould
- Symptoms and health effects
- Identifying problems
- Getting the right help
- Practical steps
- Air purifiers
What affects indoor air?
Indoor air quality is influenced by both indoor and outdoor factors. People spend most of their time indoors, so even small issues can have a noticeable effect on health. :contentReference[oaicite:0]{index=0}
Indoor air can be affected by:
- Outdoor pollution entering the building
- Damp and moisture
- Mould growth
- Cooking, heating, and cleaning products
- Dust and particles
Three common indoor air problems
1. Indoor air pollution
- Particles from cooking, heating, and candles
- Outdoor pollution enters indoors
2. Damp (moisture)
- Condensation, leaks, poor ventilation
- Creates conditions for mould growth
3. Mould
- Visible fungal growth on surfaces
- Releases spores into the air
Aspergillus in the home
Aspergillus is a common environmental fungus found in air, dust, and soil.
This means:
- Everyone breathes in Aspergillus spores regularly
- Indoor exposure is not unusual
Important: Exposure does not equal disease. Aspergillosis depends on lung health and immune response—not just environment.
Damp and mould
Damp and mould are important because they can affect respiratory health. Damp homes are linked with increased respiratory symptoms and illness. :contentReference[oaicite:1]{index=1}
UK guidance highlights that damp and mould can produce irritants and spores that affect the lungs and should be addressed promptly. :contentReference[oaicite:2]{index=2}
Symptoms and health effects
Indoor air problems may contribute to:
- Cough
- Breathlessness
- Wheeze
- Chest tightness
- Fatigue
These symptoms often overlap with infection or underlying disease, making them difficult to interpret.
Identifying problems
Signs of damp
- Condensation on windows
- Cold or damp walls
- Peeling paint or wallpaper
- Musty smell
Signs of mould
- Black or green patches
- Mould returning after cleaning
- Growth behind furniture or in corners
Hidden issues
- Persistent damp smell
- Symptoms are worse in certain rooms
Getting the right help
1. Your healthcare team
- If symptoms worsen
- If you suspect your environment is affecting your health
2. Landlord or housing provider
- Report problems early
- Keep records (photos, dates)
UK guidance makes clear that damp and mould should be addressed promptly and not ignored.
3. Local council
- If landlord does not act
- If health is affected
Further reading
See more detailed guidance and support resources here:
Housing, damp and mould articles (aspergillosis.org)
Practical steps
- Improve ventilation (especially kitchens and bathrooms)
- Reduce moisture
- Address leaks quickly
- Clean small mould areas safely
Air purifiers
Air purifiers can reduce airborne particles, but:
- They do not fix damp
- They do not remove mould from surfaces
- They do not treat aspergillosis
Final takeaway
Indoor air problems are common and often manageable. The key is to:
- Recognise the signs early
- Address moisture and mould properly
- Seek help when needed
Author: aspergillosis.org
Note: This article is for general education and does not replace medical advice.

Outdoor Air Pollution and Aspergillosis
Last reviewed: April 2026
Key points
- Harmful air pollution can be visible or invisible.
- The Air Quality Index (AQI) is more reliable than how the air looks.
- Air pollution comes from natural, industrial, and everyday urban sources.
- Staying indoors can reduce exposure, but it does not remove it completely.
- People with aspergillosis, asthma, or bronchiectasis may be more sensitive to polluted air.
- Simple steps such as checking AQI, closing windows, and using filtration can help reduce exposure.
A practical guide for patients with lung conditions
Air pollution can make breathing symptoms worse for many people, especially those with existing lung disease. If you live with aspergillosis, asthma, bronchiectasis, chronic obstructive pulmonary disease (COPD), or other long-term lung problems, outdoor air quality can make a noticeable difference to how you feel day to day.
This guide explains what outdoor air pollution is, where it comes from, how to judge risk, what practical steps may help reduce exposure, and how to think sensibly about buying an air purifier.
Contents
- What is outdoor air pollution?
- Where does it come from?
- Visible or invisible pollution
- Understanding AQI (Air Quality Index)
- Where to check AQI
- Why air pollution matters in aspergillosis
- Dust storms, haze and extreme events
- How much protection does staying indoors give?
- Practical ways to reduce exposure
- Masks and air filtration
- Buying an air purifier: what matters and what does not
- Travel and changing environments
- Common misconceptions
- Managing your condition during high air pollution
- When to seek medical help
- References
What is outdoor air pollution?
Outdoor air pollution is a mixture of particles and gases in the air that can irritate the lungs and worsen breathing symptoms.
The main pollutants discussed in health guidance include:
- PM2.5 – very fine particles small enough to travel deep into the lungs
- PM10 – slightly larger particles that can still irritate the airways
- Nitrogen dioxide (NO2) – often linked to traffic and combustion
- Ozone (O3) – a gas that can irritate the lungs, especially in hot weather
- Smoke, dust and soot – depending on local conditions
Some of these pollutants are easy to see, but some are not. This is one reason why it is important not to rely only on appearance when judging air quality.
Where does it come from?
Outdoor air pollution usually comes from a combination of sources, not just one.
Natural sources
- Desert dust or sandstorms
- Wildfire smoke
- Wind-blown soil and dust
- Pollen (not usually included in AQI in the same way, but still relevant for symptoms)
Commercial and industrial sources
- Factories
- Power stations
- Shipping emissions
- Aviation emissions
- Construction and demolition dust
Domestic and urban sources
- Road traffic
- Heating systems
- Wood burners and solid fuel burning
- Cooking emissions in densely populated areas
In some situations, one source clearly dominates. For example, a severe dust event in North Africa or the Middle East may be mainly caused by natural desert dust. In a busy city, day-to-day pollution may be more strongly linked to traffic, heating, and industry. In many real-life situations, however, several sources are contributing at the same time.
Visible or invisible pollution
One of the most important things for patients to know is that harmful air pollution can be visible or invisible.
Visible pollution
- Dust or sand in the air
- Smoke
- Grey or brown smog
- Heavy haze
Invisible pollution
- Fine particles such as PM2.5
- Gases such as ozone or nitrogen dioxide
Clear sky does not always mean clean air. Equally, hazy air is not always the only dangerous situation. Some invisible pollutants can be especially harmful because they are easy to miss and can still reach deep into the lungs.
Key message: If you can see it, it may be harmful. If you cannot see it, it still may be harmful.
Understanding AQI (Air Quality Index)
The Air Quality Index (AQI) is often the most useful practical tool for patients. It gives a simple way of describing how healthy or unhealthy the air is likely to be.
| AQI | Meaning |
|---|---|
| 0–50 | Good |
| 51–100 | Moderate |
| 101–150 | Unhealthy for sensitive groups |
| 151–200 | Unhealthy |
| 201–300 | Very unhealthy |
| 300+ | Hazardous |
Very high readings can occur in severe dust events, smoke events, or heavily polluted urban conditions. For patients with lung disease, even levels well below the highest categories may still trigger symptoms.
Why AQI matters more than appearance
AQI can help you judge risk more reliably than what you can see or smell. Dust may have no obvious smell. Fine particles may be invisible. Air that looks like fog may actually be carrying a heavy particle load. Because of this, it is usually safer to trust the AQI reading rather than appearance alone.
Where to check AQI
Reliable sources for checking air quality include:
- QAir AirVisual
– widely used internationally, with real-time air quality data, forecasts, and health guidance - UK Department for Environment, Food & Rural Affairs (DEFRA) – UK-AIR
– official UK air quality data and health advice - Plume Labs
– useful for air-quality maps and forecasts - Windy
– helpful for visualising dust, smoke and weather patterns
For most people, it is best to use one app consistently, and occasionally cross-check with a second source if readings seem unusual.
Why air pollution matters in aspergillosis
People living with aspergillosis may already have lungs that are inflamed, structurally damaged, or more easily irritated. This may include people with:
- Allergic bronchopulmonary aspergillosis (ABPA)
- Chronic pulmonary aspergillosis (CPA)
- Bronchiectasis
- Asthma
- Chronic obstructive pulmonary disease (COPD)
Air pollution can potentially worsen:
- Cough
- Breathlessness
- Chest tightness
- Wheeze
- Mucus production
- General irritation of the airways
It can also make it harder to work out what is causing symptoms. A flare in symptoms is not always due to infection. Sometimes symptoms may be made worse by air pollution, airway irritation, or inflammation, even when there is no new infection.
Dust storms, haze and extreme events
In some parts of the world, especially in North Africa and the Middle East, very high AQI readings are often caused by dust and sand in the air. This can sometimes be mistaken for fog.
Clues that this may be dust rather than fog include:
- Very high AQI readings
- Dry-looking haze rather than damp mist
- Dust collecting on surfaces
- Weather reports mentioning dust, sand, or reduced visibility
Dust does not always have a noticeable smell, so the absence of smell does not mean the air is safe.
How much protection does staying indoors give?
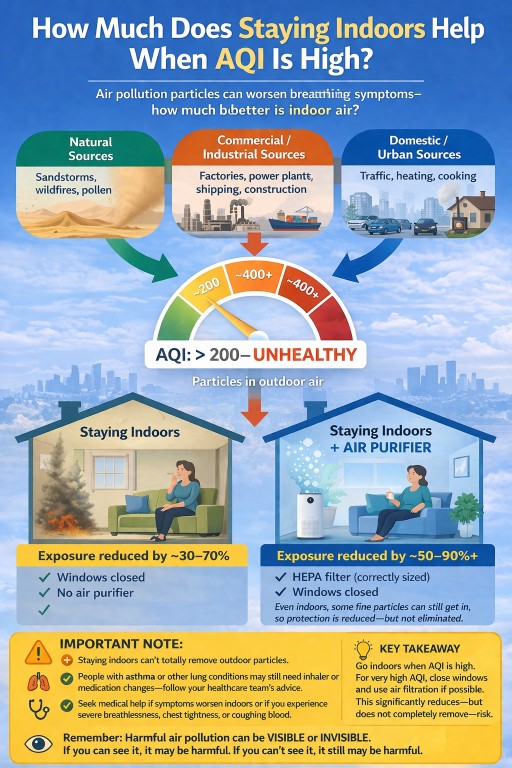
Staying indoors usually does help, but the amount of protection varies.
Typical home with windows closed
In general terms, staying indoors with windows closed may reduce exposure by around 30% to 70%, depending on:
- How well sealed the building is
- Whether windows or doors are being opened
- The age and condition of the property
- How long the pollution event lasts
Indoors with HEPA filtration
Using a correctly sized High Efficiency Particulate Air (HEPA) purifier can improve indoor air further. In some situations, this may reduce indoor particle exposure by around 50% to 90% or more.
Important limits
- Fine particles can still get indoors
- Older or drafty buildings may offer less protection
- Opening windows can quickly increase indoor particle levels again
The realistic goal is usually to reduce exposure as much as possible, not to expect complete protection.
Practical ways to reduce exposure
When outdoor AQI is high, the following steps may help:
- Stay indoors as much as possible
- Keep windows and doors closed
- Avoid strenuous outdoor activity
- Use air filtration if you have it
- Delay non-essential trips outdoors if practical
- Check AQI more than once per day during unstable conditions
For some people, symptoms may still occur even indoors. If so, it may help to reduce physical activity, keep rescue medication available if prescribed, and monitor symptoms closely.
Masks and air filtration
Masks
Well-fitted particle-filtering masks such as FFP2 or FFP3 may reduce exposure to fine particles when you need to go outdoors. Their usefulness depends heavily on fit, comfort, and wearing them correctly.
Not everyone can tolerate masks easily, especially if they are already short of breath, so they are not always a complete solution.
Air purifiers
A HEPA purifier may be especially useful in the room where you spend the most time, such as a bedroom or living room. Performance depends on:
- Correct room size
- Good maintenance of filters
- Keeping windows closed during high pollution periods
Buying an air purifier: what matters and what does not
Air purifiers can help reduce indoor particle levels, but it is important to be realistic about what they can and cannot do.
Important: An air purifier does not treat aspergillosis, does not cure asthma or bronchiectasis, and does not remove all particles. It is best thought of as one way to reduce exposure.
What matters most
- True HEPA filtration (or a clearly specified high-efficiency particle filter)
- Room-size coverage that matches the room where it will be used
- Clean Air Delivery Rate (CADR), where provided
- Noise level, especially if used in a bedroom
- Replacement filter cost and availability
What these terms mean
True HEPA: This usually means the purifier is designed to remove very small airborne particles efficiently. For patients concerned about dust and polluted air, this is generally more important than extra “smart” features.
Room size: A purifier that is too small for the room may not make much difference. It is usually better to buy the correct size for the room where you spend the most time than to buy a very cheap device that cannot handle the space.
CADR: This is a measure of how quickly a purifier can clean the air. Higher CADR usually means faster particle removal, though room size and real-life use still matter.
What to be cautious about
- Very cheap devices with vague claims but no clear filter specification
- Small USB-powered “desk purifiers” claiming to clean large rooms
- Ioniser-only devices with no proper particulate filter
- Products that make sweeping medical claims
Practical buying advice
- Start with the room you use most, often the bedroom or living room
- Choose a purifier that is rated for that room size
- Check how often filters need replacing and how much replacements cost
- Read the real specifications, not just the marketing headline
- If you are noise-sensitive, look at the sleep-mode or low-speed sound level
Reasonable expectations
Used properly, a good air purifier may make a meaningful difference during high pollution periods, especially when combined with keeping windows closed. However, it is only one part of managing exposure.
Travel and changing environments
Air quality can change dramatically between regions and countries. Some places have persistent urban pollution, while others may experience sudden dust events, wildfire smoke, or seasonal changes.
If you are travelling, it may help to:
- Check local AQI before travel and during your stay
- Be aware of seasonal dust or wildfire risks
- Know where you can spend time indoors if air quality worsens
- Keep regular medications with you
This can be particularly important if you already know that poor air quality tends to worsen your symptoms.
Common misconceptions
Myth: “If I cannot see pollution, it is safe.”
Fact: Invisible pollution such as PM2.5 and gases can still be harmful.
Myth: “If the air looks foggy, it must just be water vapour.”
Fact: Hazy air can sometimes be caused by dust or pollution rather than fog.
Myth: “Staying indoors completely solves the problem.”
Fact: Staying indoors usually reduces exposure, but does not remove it completely.
Myth: “If my symptoms worsen, it must be an infection.”
Fact: Pollution and airway irritation can also worsen symptoms.
Myth: “Air pollution is always caused by traffic.”
Fact: Pollution may come from natural, industrial, and domestic sources, often in combination.
Managing your condition during high air pollution
For people with aspergillosis, asthma, bronchiectasis or other lung conditions, air pollution can trigger symptoms even when there is no infection. Having a simple plan can help you feel more in control.
Continue your regular medication
- Take your prescribed medications as usual, including inhalers or antifungal treatments
- Do not stop or reduce medication without medical advice
Have your reliever medication available
- Carry your reliever inhaler (if prescribed) when leaving the house
- Make sure it is within easy reach, not packed away
- Check that it is in date and not empty
Plan ahead before going outdoors
- Check the AQI before leaving home
- Avoid going out during peak pollution times if possible
- Consider shorter trips or lower-exertion activities
Adjust activity levels
- Reduce strenuous activity when AQI is high
- Walk more slowly and allow extra time
- Take breaks if you feel breathless
Know your early warning signs
Be aware of symptoms that may indicate your lungs are being affected:
- Increased breathlessness
- More coughing or wheezing
- Chest tightness
- Unusual fatigue
Have a simple action plan
- Know what you usually do if symptoms worsen
- Follow any personalised plan provided by your clinical team
- Seek advice if symptoms are different from your usual pattern
Practical tip: On high pollution days, think ahead before leaving home—take medication with you, plan shorter trips, and allow extra time so you do not have to rush.
When to seek medical help
Seek medical advice promptly if you notice:
- Worsening breathlessness
- New or worsening wheeze
- Chest tightness that is not settling
- A major increase in cough
- Coughing blood (haemoptysis)
- Symptoms that are more severe than your usual pattern
If you have a severe flare, marked breathing difficulty, or significant haemoptysis, seek urgent medical help.
Final takeaway
Outdoor air pollution is an important and often under-recognised trigger for people with lung disease. For patients with aspergillosis and related lung conditions, it can worsen symptoms even when there is no new infection.
The most helpful practical points are:
- Use AQI rather than appearance alone
- Remember that pollution may be visible or invisible
- Stay indoors when AQI is high
- Use air filtration where possible
- Keep an eye on changing symptoms and seek help if needed
References
- World Health Organization. WHO Global Air Quality Guidelines. 2021.
- UK Department for Environment, Food & Rural Affairs (DEFRA). UK-AIR: Air Information Resource.
- IQAir AirVisual air quality app.
- European Respiratory Society statements and guidance on air pollution and respiratory health.
- British Thoracic Society resources on respiratory health and environmental exposure.
Author: Prepared for aspergillosis.org
Review note: This article is intended for general education and should not replace advice from your own clinical team.

Voriconazole interactions: what patients need to know
Key points
- Voriconazole interacts with many medicines.
- It affects several liver enzyme pathways, including CYP3A4, CYP2C19, and CYP2C9.
- Its behaviour can vary more from one person to another than some other azoles.
- Some medicines can make voriconazole stronger, while others can make it less effective.
- Visual side effects and sensitivity to sunlight are well recognised with voriconazole.
What is voriconazole?
Voriconazole is an azole antifungal often used in serious fungal infections, including aspergillosis. It can be very effective, but it also has a relatively complex interaction profile.
Why voriconazole interacts with so many medicines
Voriconazole affects several liver enzyme systems, including CYP3A4, CYP2C19, and CYP2C9. It can increase the levels of some medicines, while some other medicines can lower voriconazole levels and reduce its effectiveness.
Because voriconazole metabolism varies between patients, the same combination can affect people differently.
The interaction groups most likely to matter
Steroids
Voriconazole can increase exposure to some steroids, including inhaled steroids, which may increase the risk of steroid side effects.
Medicines that reduce voriconazole levels
Some medicines, including certain anti-seizure medicines and rifampicin-type antibiotics, can reduce voriconazole levels so much that the antifungal may not work properly.
Blood thinners
Some blood thinners may become stronger when taken with voriconazole, increasing bleeding risk.
Heart rhythm medicines
Voriconazole can contribute to QT prolongation, so combinations with other medicines that affect heart rhythm may be particularly important.
Statins
Some statins can become stronger when taken with voriconazole, increasing the risk of muscle side effects.
Immunosuppressants
Medicines such as tacrolimus and ciclosporin can rise significantly with voriconazole and often require specialist monitoring and dose adjustment.
Sedatives and some mental health medicines
Some sedatives and psychiatric medicines can become stronger when combined with voriconazole, increasing the risk of drowsiness, confusion, or other side effects.
Voriconazole-specific issues patients should know
Visual changes
Temporary visual disturbances are well recognised with voriconazole. Patients may notice blurred vision, brighter vision, or changes in colour perception.
Photosensitivity
Voriconazole can increase sensitivity to sunlight. Patients should use sensible sun protection and report new skin changes, especially during long-term treatment.
Variable drug levels
Voriconazole levels can vary between patients, which is one reason some teams use therapeutic drug monitoring in selected situations.
What patients should do in practice
- Tell your clinical team and pharmacist that you are taking voriconazole.
- Check before starting new medicines, including over-the-counter or herbal products.
- Report visual changes, significant sensitivity to sunlight, or a change in symptoms after a medicine change.
- Do not change treatment without advice.
When to seek medical advice
Seek medical advice urgently for severe bleeding, fainting, severe palpitations, marked confusion, or rapid worsening after a medicine change.
Important
This page is educational and does not list every interaction. For a full check, use the BNF interaction checker or speak to a pharmacist or clinician.
References
Itraconazole interactions: what patients need to know
Key points
- Itraconazole can interact with many other medicines.
- It usually does this by affecting liver enzymes, especially CYP3A4.
- Some combinations need careful monitoring, while others are best avoided.
- Capsules and liquid formulations are not handled by the body in exactly the same way.
- This page highlights the interactions most likely to matter to people with aspergillosis.
What is itraconazole?
Itraconazole is an azole antifungal used in aspergillosis and other fungal infections. It has a relatively high interaction burden, so medicine checks are especially important before starting it and whenever another medicine is added, stopped, or changed.
Why itraconazole interacts with so many medicines
Itraconazole can increase the levels of some other medicines by affecting liver enzymes, especially CYP3A4. This means that some medicines may become stronger than intended, which can increase the risk of side effects or toxicity.
The interaction groups most likely to matter
Steroids and inhalers
This is one of the most important groups for many aspergillosis patients, especially those with asthma or allergic bronchopulmonary aspergillosis. Itraconazole can increase exposure to some steroids, including inhaled steroids, which may increase the risk of steroid side effects.
Possible symptoms to report: unusual weight gain, easy bruising, increased facial rounding, mood changes, worsening blood sugar control, weakness, or marked fatigue.
Statins
Some statins can become much stronger when taken with itraconazole. This can increase the risk of muscle toxicity.
Possible symptoms to report: new muscle pain, muscle weakness, or dark urine.
Blood thinners
Itraconazole can increase the effect of some blood thinners, which may raise bleeding risk.
Possible symptoms to report: unusual bruising, bleeding that is hard to stop, black stools, vomiting blood, or coughing up much more blood than usual.
Heart and rhythm medicines
Some combinations can increase the risk of serious heart rhythm problems. Itraconazole is also used cautiously in people with a history of ventricular dysfunction or heart failure unless the infection is serious.
Possible symptoms to report: fainting, palpitations, marked dizziness, increasing ankle swelling, or worsening breathlessness.
Sleeping tablets, sedatives, and some mental health medicines
Some sedatives and psychotropic medicines can become stronger when combined with itraconazole, increasing the risk of drowsiness, confusion, falls, or breathing problems.
Immunosuppressants
Medicines such as tacrolimus and ciclosporin can rise significantly when taken with itraconazole and usually need specialist monitoring.
Medicines that can make itraconazole less effective
Some medicines lower itraconazole levels, which means the antifungal may not work as well. This can happen with some anti-seizure medicines, rifampicin-type antibiotics, and some antiviral medicines.
Acid-reducing medicines and itraconazole capsules
Reduced stomach acid can lower the absorption of itraconazole capsules. This means reflux medicines, antacids, and some acid-suppressing treatments can affect how well the capsules work. The liquid formulation behaves differently and should not be treated as interchangeable with capsules.
What patients should do in practice
- Keep a current medicines list and bring it to appointments.
- Tell clinicians and pharmacists if you are taking itraconazole.
- Ask specifically about inhalers, steroid tablets, statins, blood thinners, and reflux treatment.
- Do not change doses or stop medicines without advice.
- If your itraconazole formulation changes, ask whether it should be taken with food or on an empty stomach.
When to seek medical advice
Seek urgent medical advice for severe bleeding, black stools, vomiting blood, severe muscle pain, fainting, marked palpitations, or rapidly worsening breathlessness.
Important
This page is not a full interaction database. For a complete medicine-by-medicine check, use the BNF interaction checker or speak to a pharmacist or clinician.
References
Amphotericin B interactions: what patients need to know
Key points
- Amphotericin B comes in different formulations, and they are not interchangeable.
- Its main interaction risks are different from the azoles.
- The most important problems are usually kidney stress, low potassium, low magnesium, and additive toxicity with other medicines.
- These risks matter most with intravenous treatment.
- If you hear “amphotericin B”, it is important to know which formulation is being used.
What is amphotericin B?
Amphotericin B is an antifungal used mainly for serious fungal infections. In modern UK practice this often means liposomal amphotericin B, but conventional amphotericin B deoxycholate is also a recognised formulation.
Why amphotericin B interactions are different from azoles
Unlike azole antifungals, amphotericin B does not mainly cause medicine interactions through liver enzymes. Its most important interaction risks usually relate to kidney injury, low potassium, low magnesium, and infusion-related effects.
The interaction groups most likely to matter
Other medicines that can damage the kidneys
This is one of the most important groups. Combining amphotericin B with other nephrotoxic medicines can increase the risk of kidney injury.
Diuretics, steroids, and other medicines that lower potassium
Amphotericin B can lower potassium, and some other medicines can make this worse. This may increase the risk of weakness, cramps, or heart rhythm problems.
Digoxin and heart-rhythm-sensitive situations
Low potassium caused by amphotericin B can make digoxin-related toxicity more likely and may increase the importance of electrolyte monitoring.
Flucytosine
When combined with flucytosine, specialist monitoring may be needed because toxicity can increase.
Some cancer medicines and intensive hospital treatments
In hospital, additive toxicity with other intensive treatments may be particularly important, especially where kidneys and electrolytes are already under strain.
White blood cell transfusions
Acute lung reactions are a recognised specialist concern if amphotericin B is given during or soon after leukocyte transfusions.
Why the formulations matter
Amphotericin B formulations are not interchangeable. Conventional amphotericin B deoxycholate and liposomal amphotericin B have different dosing, different handling by the body, and different safety profiles. Using the wrong formulation in the wrong dose has caused serious and even fatal errors.
In general, liposomal amphotericin B is less nephrotoxic than conventional amphotericin B deoxycholate, but it still requires careful monitoring.
What patients should do in practice
- Ask which amphotericin B formulation is being used.
- Tell the clinical team about all medicines, especially kidney-risk medicines, diuretics, steroids, and digoxin.
- Expect blood tests to monitor kidney function, potassium, and magnesium during intravenous treatment.
- Report weakness, reduced urine output, worsening swelling, palpitations, or marked dizziness.
When to seek medical advice
Seek urgent medical help for severe breathlessness, fainting, major palpitations, or a rapid deterioration during treatment.
Important
This page is educational and does not list every possible interaction. Amphotericin B treatment is usually managed by specialist teams, especially when given intravenously.
References
Isavuconazole interactions: what patients need to know
Key points
- Isavuconazole can interact with other medicines, but its interaction profile is often less complex than older azoles.
- It mainly interacts through CYP3A4.
- Some medicines can increase isavuconazole levels, while others can reduce its effectiveness.
- It has an important difference from some other azoles: it can shorten the QT interval.
- It is still essential to check new medicines carefully.
What is isavuconazole?
Isavuconazole is a newer azole antifungal used in invasive aspergillosis and some other serious fungal infections. It is often seen as having a more predictable interaction profile than some older azoles, but it still has important interactions.
Why isavuconazole interacts with other medicines
Isavuconazole is mainly linked to CYP3A4. This means some medicines can become stronger when combined with it, while other medicines can lower isavuconazole levels and reduce its effectiveness.
The interaction groups most likely to matter
Medicines that reduce isavuconazole effectiveness
Some medicines, including rifampicin-type antibiotics and certain anti-seizure drugs, can lower isavuconazole levels and may make treatment ineffective.
Steroids
Some steroid levels may rise with isavuconazole, although the interaction pattern is often less intense than with some older azoles.
Immunosuppressants
Medicines such as tacrolimus and ciclosporin may increase and usually need specialist review and monitoring.
Blood thinners
Some blood thinners may become stronger, increasing bleeding risk.
Statins
Some statin levels may increase, which can raise the risk of muscle side effects.
Important isavuconazole-specific points
QT shortening
Unlike several other azole antifungals, isavuconazole can shorten the QT interval. This is an important difference and should be considered when other heart medicines are being reviewed.
Generally simpler interaction profile
Compared with itraconazole and voriconazole, isavuconazole is often considered a little easier to manage in patients taking several medicines, although checks are still essential.
What patients should do in practice
- Tell your pharmacist or clinician if you are taking isavuconazole.
- Check before starting prescription, over-the-counter, or herbal medicines.
- Ask specifically about anti-seizure drugs, antibiotics, blood thinners, and heart medicines.
- Do not stop or change medicines without advice.
When to seek medical advice
Seek medical advice urgently for severe bleeding, fainting, severe palpitations, severe muscle pain, or rapid worsening after a medicine change.
Important
This page is educational and not a complete interaction database. For a full check, use the BNF interaction checker or speak to a pharmacist or clinician.
References
- BNF: isavuconazole monograph and interactions
- UK isavuconazole SmPCs - not available
Posaconazole interactions: what patients need to know
Key points
- Posaconazole can interact with other medicines, although its interaction pattern is often a little simpler than itraconazole or voriconazole.
- It mainly interacts through CYP3A4 inhibition.
- Important interaction groups include immunosuppressants, steroids, blood thinners, and some heart medicines.
- Some medicines can reduce posaconazole levels and make treatment less effective.
- Tablets and oral suspension are not interchangeable in the same way.
What is posaconazole?
Posaconazole is an azole antifungal used in aspergillosis and in some high-risk patients for prevention of fungal infection. It is often seen as somewhat easier to manage than some older azoles, but important interactions still exist.
Why posaconazole interacts with other medicines
Posaconazole mainly affects CYP3A4, a key liver enzyme involved in handling many medicines. This means some drugs can become stronger, while some combinations can lower posaconazole levels and make it less effective.
The interaction groups most likely to matter
Steroids
Posaconazole can increase exposure to some steroids, including inhaled or oral steroids, which may increase the risk of steroid side effects.
Immunosuppressants
Medicines such as tacrolimus and ciclosporin can rise significantly with posaconazole and usually need close specialist monitoring.
Blood thinners
Some blood thinners may become stronger, increasing bleeding risk.
Statins
Some statins can rise in level, increasing the risk of muscle problems.
Heart rhythm medicines
Some combinations can increase the risk of heart rhythm problems and need careful review.
Medicines that reduce posaconazole effectiveness
Some medicines, including rifampicin-type antibiotics and certain anti-seizure drugs, can lower posaconazole levels and may make treatment less effective.
Posaconazole formulations and absorption
Posaconazole comes in different forms, including tablets, oral suspension, and infusion. The oral suspension and tablets are not handled identically by the body and should not be assumed to be interchangeable dose-for-dose without clinical advice.
In practice, the tablets tend to be more predictable than the suspension.
What patients should do in practice
- Tell your pharmacist or clinician if you are taking posaconazole.
- Ask about new medicines, especially blood thinners, steroids, statins, and heart medicines.
- If your formulation changes, ask whether there are any special instructions.
- Do not stop or swap medicines without advice.
When to seek medical advice
Seek medical advice urgently for severe bleeding, fainting, major palpitations, severe muscle pain, or rapid worsening after a medicine change.
Important
This page does not list every interaction. For a full check, use the BNF interaction checker or speak to a pharmacist or clinician.
References
Antifungal drug interactions: what patients with aspergillosis need to know
Key points
- Antifungal medicines can interact with other medicines, including inhalers, steroid tablets, blood thinners, heart medicines, cholesterol tablets, and some over-the-counter or herbal products.
- The azole antifungals usually interact by affecting how the liver handles medicines.
- Amphotericin B is different: its main interaction risks are more often linked to kidneys, potassium, magnesium, and infusion-related effects.
- This page gives an overview. It does not list every interaction.
- For a full medicine-by-medicine check, use the BNF interaction checker or ask a pharmacist or clinician.
Why interactions matter in aspergillosis
People with aspergillosis often take more than one medicine. This may include inhalers, steroid tablets, medicines for reflux, antibiotics, pain relief, blood pressure treatment, blood thinners, cholesterol tablets, and drugs for other long-term conditions. That means medicine checks are especially important whenever an antifungal is started, stopped, or changed.
How the main antifungals differ
Most long-term interaction questions in aspergillosis involve the azole antifungals: itraconazole, voriconazole, posaconazole, and isavuconazole. These mainly interact because they affect liver enzymes, especially CYP3A4, although some also affect CYP2C9 and CYP2C19.
Amphotericin B behaves differently. Its most important risks are usually kidney stress, low potassium, low magnesium, and additive toxicity with other medicines rather than classic liver-enzyme interactions.
Quick comparison table
| Antifungal | Main interaction pattern | Typical complexity | Important extra point |
|---|---|---|---|
| Itraconazole | Strong enzyme-based interactions, especially CYP3A4 | High | Capsules and liquid are not handled by the body in the same way |
| Voriconazole | Complex enzyme-based interactions involving several CYP pathways | High | More variable between patients; visual side effects and photosensitivity are well recognised |
| Posaconazole | Mainly CYP3A4-related interactions | Moderate | Tablets and oral suspension are not interchangeable in the same way |
| Isavuconazole | Mainly CYP3A4-related interactions, usually less complex than older azoles | Lower to moderate | Can shorten the QT interval |
| Amphotericin B | Kidney, potassium, magnesium, and infusion-related interaction risks | Different rather than simpler | Formulations are not interchangeable |
Individual antifungal guides
- Itraconazole interactions: what patients need to know
- Voriconazole interactions: what patients need to know
- Posaconazole interactions: what patients need to know
- Isavuconazole interactions: what patients need to know
- Amphotericin B interactions: what patients need to know
What patients should do in practice
- Keep an up-to-date list of all medicines, including inhalers, creams, over-the-counter medicines, supplements, and herbal products.
- Tell your doctor, nurse, pharmacist, or hospital team that you are taking an antifungal.
- Do not start, stop, or swap medicines on your own because of something you have read online.
- Ask specifically about new medicines, steroid changes, reflux treatment, blood thinners, cholesterol medicines, and heart medicines.
When to seek medical advice
Seek medical advice promptly if symptoms change after a medicine is started, stopped, or changed. Seek urgent help for severe bleeding, fainting, severe muscle pain, marked palpitations, rapidly worsening breathlessness, severe drowsiness, or a sudden significant decline in your health.
Important
This resource is educational. It does not replace personalised advice from your clinical team, GP, or pharmacist, and it is not a complete interaction database.
References
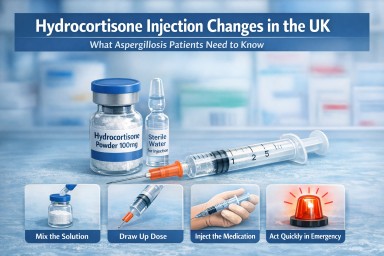
Hydrocortisone Injection Changes in the UK: What It Means for Aspergillosis Patients
Last reviewed: March 2026
Audience: Patients, carers, and non-specialist healthcare professionals
Key points
- A ready-to-use hydrocortisone injection (liquid solution) is no longer available in the UK.
- Patients are now usually given a hydrocortisone injection that must be mixed before use.
- The medication itself is unchanged, but preparation is more complex.
- This may feel more difficult during an emergency, especially if someone is unwell or distressed.
- Training and preparation can help reduce delays.
- Always seek urgent medical help in a suspected emergency.
Table of contents
- Overview
- Why hydrocortisone matters in aspergillosis
- What has changed in the UK
- What this means in practice
- Potential concerns and risks
- Practical steps for patients and carers
- Common questions
- When to seek medical help
- References
Overview
Hydrocortisone is a steroid hormone used as cortisol replacement in people whose bodies cannot produce enough cortisol, a condition known as adrenal insufficiency.
Some patients with aspergillosis may be affected by this change because:
- long-term steroid use can suppress the body’s natural cortisol production
- adrenal function may be reduced during or after treatment
- some patients may already have adrenal insufficiency or need emergency steroid cover
In emergencies, hydrocortisone injections can be life-saving.
Why hydrocortisone matters in aspergillosis
Patients with aspergillosis may encounter adrenal-related issues for several reasons. For example, some people with allergic bronchopulmonary aspergillosis (ABPA) have needed prolonged courses of steroid treatment. Over time, this can reduce the body’s own cortisol production.
There can also be concerns about drug interactions, especially where antifungal medicines and steroid medicines affect the way the body handles hormones. Not every aspergillosis patient will be affected, but for some people this is an important part of their wider treatment plan.
If cortisol levels are too low during illness, injury, vomiting, or other physical stress, this can lead to an adrenal crisis, which is a medical emergency.
What has changed in the UK
Previously, some patients were supplied with a ready-made liquid hydrocortisone injection. This was already in solution and could be given more quickly.
This ready-to-use product is no longer available in the UK.
Most patients who need emergency hydrocortisone injection are now supplied with a preparation that includes:
- a vial containing hydrocortisone powder
- a liquid for mixing
- a syringe and needle for drawing up and giving the injection
The medicine itself is still hydrocortisone and remains standard treatment. What has changed is the practical process: it now needs to be prepared before it can be injected.
Diagram: preparing hydrocortisone injection
Preparing a hydrocortisone injection (Video) : https://www.youtube.com/watch?v=NXXB3w1ADcI
What this means in practice
For many patients, this change is manageable with training and practice. However, it does change the experience of using emergency medication.
Compared with a ready-made solution, there are now more steps involved. In a calm situation, that may not seem significant. In an emergency, it can feel much harder.
This is especially relevant if the person is:
- very unwell
- vomiting
- dizzy or confused
- trying to guide a family member or carer through the process
For some patients, this could potentially cause a delay in giving the injection. That does not mean the current treatment is ineffective or unsafe, but it does mean that confidence, familiarity, and training matter even more.
Potential concerns and risks
1. More steps may mean more delay
The current injection usually has to be mixed before use. That means opening the kit, preparing the medicine, drawing it up, and then giving the injection. In an emergency, even a short delay may feel important.
2. Stress makes practical tasks harder
Patients and carers are often being asked to act quickly during a frightening situation. Even people who have previously been shown what to do may lose confidence if they rarely need to use the injection.
3. Training may vary
Not everyone receives the same level of teaching or refresher support. Some people may feel very confident. Others may feel unsure, especially if their kit has changed.
4. Aspergillosis patients may already be managing a lot
Some patients are already coping with breathlessness, fatigue, infections, multiple medicines, and complex follow-up. Adding a more complicated emergency injection process can feel like an extra burden.
It is important to keep this concern in proportion. Many patients and carers do use mixed hydrocortisone kits successfully. The key issue is not that the medicine no longer works, but that the loss of a ready-made formulation may make emergency use less straightforward.
Practical steps for patients and carers
If you have been prescribed emergency hydrocortisone, it may help to:
- check that you know exactly which product you have been given
- ask for a demonstration of how to prepare and inject it
- ask for a refresher if you are not confident
- make sure family members, carers, or trusted friends also know what to do
- keep the emergency kit somewhere accessible and check expiry dates regularly
- carry any steroid emergency information you have been given, such as a steroid card
These steps cannot remove all risk, but they may reduce hesitation and confusion if the injection is ever needed urgently.
Common questions
Has hydrocortisone been withdrawn completely?
No. Hydrocortisone is still widely used. The main issue is that a ready-to-use liquid injectable form is no longer available in the UK.
Is the current injection less effective?
No. The medicine remains hydrocortisone. The change is in the formulation and the preparation steps, not in the intended effect of treatment.
Why does this matter so much?
In an emergency, simple treatments are often easier to use correctly and quickly. A preparation that needs mixing may be more difficult for some patients or carers under pressure.
Does this affect every aspergillosis patient?
No. This is mainly relevant to people who have adrenal insufficiency, adrenal suppression, or a clear plan from their clinical team to keep emergency hydrocortisone available.
Should patients be worried?
Patients should not panic, but it is reasonable to recognise this as a practical concern. If you rely on emergency hydrocortisone, it is sensible to make sure you understand your current kit and feel as confident as possible using it.
When to seek medical help
Seek urgent medical help if there are symptoms suggesting a possible adrenal emergency, especially if there is:
- severe weakness
- collapse or near-collapse
- confusion or marked drowsiness
- vomiting or inability to keep medicines down
- sudden severe illness or infection
If an emergency hydrocortisone injection has been prescribed, follow the instructions given by your clinical team and seek urgent medical care immediately.
References
- British National Formulary (BNF): hydrocortisone medicinal forms
- Society for Endocrinology guidance on adrenal crisis and emergency steroid treatment
- NHS information on steroids, steroid emergency cards, and urgent care
- UK endocrine and Addison’s patient group communications on hydrocortisone supply changes
Author and review information
Prepared for: aspergillosis.org
Purpose: General information for patients, carers, and non-specialist healthcare professionals
Important note: This article is intended for general education and should not replace individual medical advice from your own clinical team.