Can People with Aspergillosis Drink Kefir or Take Probiotics?
Many people with aspergillosis ask whether they can safely drink kefir or take probiotics. Kefir is a fermented drink containing live bacteria and yeasts, which raises understandable questions for people with lung conditions. This article explains what is known, what is uncertain, and why advice can differ between chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), and more severe forms of aspergillosis.
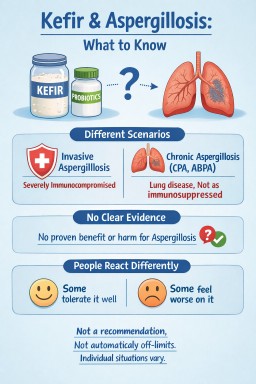
Short answer: this is not something with a simple yes-or-no answer. For people with chronic forms of aspergillosis, kefir and probiotic products are not routinely discussed in the same way as they are for people who are severely immunocompromised. However, there is also not enough evidence to say they are helpful for aspergillosis, and people’s experiences vary.
Key Points
- Advice about live foods is often stricter for people with invasive aspergillosis or severe immune suppression
- For chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), and related long-term conditions, the picture is usually less clear-cut
- There is no strong evidence that kefir specifically helps or harms chronic aspergillosis
- Some people feel fine with fermented foods; others feel they do not suit them
- The aim here is to inform, not recommend
What Is Kefir?
Kefir is a fermented drink, usually made from milk, containing a mixture of bacteria and yeasts. It is often described as a probiotic food because it contains live microorganisms.
People may use kefir or probiotic products because of interest in:
- gut health
- recovery after antibiotics
- the microbiome
If you are interested in the wider role of food and nutrition in lung health, see our article on diet and aspergillosis: what helps, what doesn’t, and what matters most.
Why Does This Question Come Up in Aspergillosis?
Different forms of aspergillosis have different risk profiles
It is important not to group all forms of aspergillosis together.
- Invasive aspergillosis usually affects people with very weakened immune systems. In that setting, clinicians are often more cautious about foods or products containing live microorganisms.
- Chronic pulmonary aspergillosis (CPA) usually affects people with underlying lung damage or structural lung disease. Many patients are not severely immunocompromised in the same way.
- Allergic bronchopulmonary aspergillosis (ABPA) and related allergic conditions raise slightly different questions again, because symptom flares may relate more to sensitivity and inflammation than to infection risk.
That distinction matters, because advice that is appropriate for one group may not automatically apply to another.
Chronic vs Invasive Aspergillosis: Why It Matters
For people with chronic pulmonary aspergillosis, the question is usually less about needing to avoid kefir as a rule, and more about recognising that there is no established role for it in treatment. In other words, kefir is not a treatment for CPA, but nor is it routinely listed as something that every patient with CPA must avoid.
For people with ABPA, the picture is slightly different again. Some patients are very aware of foods that seem to trigger symptoms, but that still does not create a universal rule that fermented foods should always be avoided.
What Does the Evidence Say?
At present, there is no strong evidence showing that kefir has a specific benefit for aspergillosis, and there is also no clear evidence that it is harmful in most people with chronic aspergillosis.
Most discussion around kefir and probiotics comes from broader research on:
- the gut microbiome
- antibiotic-associated bowel symptoms
- general digestive health
That is not the same as proving benefit for lung symptoms, fungal disease, or long-term respiratory outcomes.
For related discussion about how antibiotics affect symptoms, infections, and the microbiome, you may also find this helpful: why antibiotics do not always work.
Probiotics and the Gut–Lung Connection
Research into the gut–lung axis suggests that the gut microbiome may influence immune responses elsewhere in the body, including the lungs. This is an active area of research, but it is still early, and it does not yet mean that fermented foods or probiotic supplements should be seen as treatments for aspergillosis.
Some people are interested in probiotics because of repeated antibiotic courses, bowel side effects, or a general wish to support gut health. Those are understandable reasons, but the evidence for a direct lung benefit in chronic aspergillosis remains limited.
Why Do People React Differently?
The main reasons for caution are usually not “aspergillosis” on its own, but the wider clinical picture.
For example, extra caution may be more relevant in people who are:
- severely immunocompromised
- taking high-dose steroids or other immunosuppressive treatment
- acutely unwell
- known to react poorly to fermented foods or probiotic products
In some people, symptoms after kefir may be more about tolerance than infection risk. Patients sometimes describe:
- bloating
- nausea
- abdominal discomfort
- a sense that fermented foods do not suit them
Others report no obvious problems at all. This is one reason it is safer to frame kefir as an individual tolerance issue rather than something routinely recommended or routinely banned.
Kefir in Chronic Pulmonary Aspergillosis (CPA)
For people with CPA, the question is usually less about fungal exposure from kefir and more about whether it suits the individual patient. Many people with CPA have damaged lungs rather than profound immune suppression, so the same dietary warnings used in invasive fungal disease do not automatically apply.
- kefir is not a standard treatment for CPA
- it is not routinely listed as something that must be avoided in all patients with CPA
- individual circumstances, treatments, and tolerance still matter
If you are newly diagnosed or want a broader overview, see our CPA information page.
What About ABPA and Other Allergic Conditions?
In ABPA and related conditions, some people are understandably more alert to foods that seem to trigger symptoms. Fermented products may not suit everyone, but there is not a clear universal rule that they should be avoided.
As with many food-related questions in chronic lung disease, experiences are mixed and difficult to generalise. If you would like a fuller explanation of ABPA itself, visit our ABPA information page.
Homemade vs Shop-Bought Products
Some people also ask whether homemade kefir is different from commercial products. In general terms, homemade fermented products may be less standardised than commercially prepared ones, but that does not automatically mean they will cause a problem. It simply adds another layer of variability.
This is another reason why broad, one-size-fits-all advice is difficult.
How Should This Be Framed for Patients?
A cautious and balanced way to put it is:
Kefir is a fermented drink containing live bacteria and yeasts. Questions about it often come up in aspergillosis because advice is sometimes stricter for people who are severely immunocompromised. For people with chronic conditions such as CPA or ABPA, there is no clear evidence that kefir is either beneficial or harmful for aspergillosis itself. People’s experiences vary, so it is best thought of as an individual tolerance issue rather than something routinely recommended or routinely banned.
When Extra Caution May Be Needed
Extra caution may be more relevant if someone is:
- severely immunocompromised
- on significant immunosuppressive treatment
- recovering from serious illness
- already experiencing ongoing gut symptoms or unexplained food intolerance
In those situations, questions about probiotics, supplements, or fermented foods are often best discussed with a clinician who understands the wider medical picture.
When to Seek Medical Advice
It is sensible to discuss diet or probiotic questions with a clinician or specialist team if:
- you are severely immunocompromised
- you are on significant immunosuppressive treatment
- you develop persistent gut symptoms after using a probiotic product
- you are unsure how advice applies to your particular diagnosis or treatment
Healthcare professionals looking for more formal clinical material can visit our Information for Professionals page.
Common Questions
Can kefir treat aspergillosis?
No. There is no evidence that kefir treats aspergillosis.
Is kefir dangerous with chronic pulmonary aspergillosis?
There is no clear evidence that kefir is harmful in most people with chronic pulmonary aspergillosis, but there is also no evidence that it is beneficial for the condition itself. Tolerance varies between individuals.
Should people with ABPA avoid fermented foods?
Not necessarily. Some people feel certain foods do not suit them, but there is no universal rule that all fermented foods should be avoided in ABPA.
Summary
- Kefir is a fermented probiotic drink containing live bacteria and yeasts
- Advice that applies to invasive aspergillosis does not always apply in the same way to chronic pulmonary aspergillosis or allergic bronchopulmonary aspergillosis
- There is no strong evidence that kefir treats or worsens chronic aspergillosis
- The safest educational position is a neutral one: not a recommendation, not a blanket prohibition
- Individual circumstances, treatments, and tolerance matter
Last reviewed: April 2026
Reviewed by: National Aspergillosis Centre patient information team perspective
Please note: This article is for general education and should not be used as individual medical advice.
Could diarrhoea on itraconazole be C. diff?
Last reviewed: 20 April 2026
Understanding the difference for people with aspergillosis
Key points
- Clostridioides difficile (C. diff) is a bowel infection most often linked to antibiotic use, not antifungal treatment.
- Itraconazole can cause diarrhoea and stomach upset as a recognised side effect, but that is not the same as having C. diff.
- People with aspergillosis may still be at higher risk of C. diff because many have had recent antibiotics, repeated antibiotic courses, hospital care, or other illnesses.
- Persistent watery diarrhoea, tummy pain, fever, bleeding, dehydration, or diarrhoea lasting more than a few days should not be ignored.
- Probiotics may help some people reduce antibiotic-associated diarrhoea, but they are not suitable for everyone and are not a treatment for C. diff.
Contents
- Why this question comes up so often
- What is C. diff?
- Is itraconazole a usual cause of C. diff?
- Why people with aspergillosis may still worry about C. diff
- Side effect or infection?
- What do NHS sources advise?
- Do probiotics help?
- Common questions
- Why this matters in aspergillosis
- When to seek medical advice
- Take-home message
- Suggested internal links
- References
Why this question comes up so often
If you live with aspergillosis, it can be hard to work out why new symptoms have appeared. Many patients have had antibiotics at some point for chest infections, have been in hospital, or take several medicines at once. So when diarrhoea develops while on itraconazole, it is understandable to wonder whether the antifungal is to blame, whether it is a simple side effect, or whether something more important is going on.
That confusion is common, because several different problems can cause similar gut symptoms.
What is C. diff?
Clostridioides difficile (C. diff) is a bacterium that can infect the bowel and cause diarrhoea, abdominal pain and sometimes much more severe illness. It often affects people whose usual gut bacteria have been disrupted, especially after antibiotic use.
Some people carry C. diff without symptoms, but when the balance of the gut changes, the bacteria can multiply and produce toxins that irritate and inflame the bowel. That is why C. diff is more than “just diarrhoea”. It is a specific infection with recognised causes and recognised risks.
Is itraconazole a usual cause of C. diff?
In general, no. Itraconazole is an antifungal, not an antibiotic, and it is not recognised as a typical trigger for C. diff. Most guidance links C. diff mainly to antibiotics, especially in people who are older, frailer, recently hospitalised, or otherwise vulnerable.
That said, itraconazole can cause gastrointestinal side effects, including diarrhoea. So someone may genuinely develop bowel symptoms while taking itraconazole without having C. diff.
The important point is this: diarrhoea on itraconazole does not automatically mean C. diff, but it should not automatically be dismissed as “just the antifungal” either.
Why people with aspergillosis may still worry about C. diff
Even if itraconazole is not the usual cause, people with aspergillosis may still face a real risk of C. diff because many have had one or more recognised risk factors:
- recent or repeated antibiotic courses
- recent hospital stay or healthcare exposure
- older age
- other illnesses or frailty
- sometimes medicines such as proton pump inhibitors have also been associated with increased risk
So in practice, a patient may be taking itraconazole when diarrhoea starts, but the bigger driver may actually be a recent antibiotic course or hospital admission rather than the antifungal itself.
Side effect or infection?
Here is the distinction many patients find helpful.
Diarrhoea more suggestive of a medicine side effect
A simple side effect from itraconazole may cause:
- looser stools
- nausea
- abdominal discomfort
- symptoms that are unpleasant but relatively mild and not rapidly worsening
Diarrhoea more concerning for C. diff or another bowel infection
Symptoms that deserve proper attention include:
- frequent watery diarrhoea
- tummy pain or cramping
- fever
- blood in the stool or bleeding from the bottom
- dehydration, such as very dry mouth, dizziness, or passing very little urine
- diarrhoea lasting more than 7 days
- feeling generally very unwell
| More suggestive of side effect | More concerning for infection such as C. diff |
|---|---|
| Mild diarrhoea or looser stools | Frequent watery diarrhoea |
| Mild nausea or stomach discomfort | Tummy pain, cramping, fever |
| Symptoms remain mild | Symptoms worsening or lasting several days |
| No bleeding or dehydration | Bleeding, dehydration, or feeling very unwell |
In other words, the pattern and severity matter. Mild stomach upset can happen with many medicines. Persistent watery diarrhoea, pain, fever or bleeding should not simply be written off as “one of those things”.
What do NHS sources advise?
NHS advice is to seek urgent help if diarrhoea happens while taking, or after recently taking, antibiotics, if there is blood in the diarrhoea, or if it lasts more than 7 days. Severe pain, fever, or signs of dehydration are also warning signs.
This matters because true C. diff is a recognised medical problem with specific treatment pathways.
Do probiotics help?
Probiotics are products that contain live microorganisms (usually bacteria or yeast) intended to support the balance of the gut microbiome. They are often sold as capsules, powders, or drinks.
They are widely available, but their role in preventing or managing diarrhoea is still being studied, and product quality varies considerably.
What does the evidence suggest?
- Some studies suggest probiotics may help reduce antibiotic-associated diarrhoea.
- There is some evidence they may reduce the risk of C. diff in certain situations, particularly when started early during antibiotic treatment.
- However, results are inconsistent, and benefits are usually modest.
Are probiotics a treatment for C. diff?
No. Probiotics are not a standard treatment for confirmed C. diff infection. Medical treatment is required for confirmed cases.
How to recognise a higher-quality probiotic
If people are considering probiotics, it can be helpful to understand what distinguishes more credible products from less reliable ones.
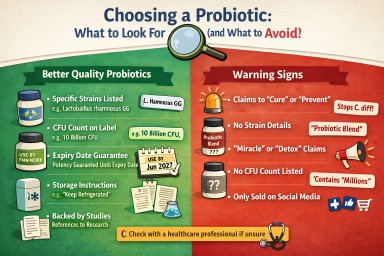
- Clearly labelled strains – for example Lactobacillus rhamnosus GG rather than just “Lactobacillus”. Evidence is strain-specific.
- CFU count (colony forming units) – this indicates the number of live organisms. Typical products range from millions to billions of CFU.
- Expiry-date guarantee – reputable products state the number of live organisms at the end of shelf life, not just “at manufacture”.
- Storage instructions – some require refrigeration; unclear instructions may suggest lower quality control.
- Evidence transparency – more reliable manufacturers refer to published studies rather than making vague claims.
Common red flags to be cautious about
- Claims to “cure” or “prevent” serious conditions such as C. diff
- Very long lists of ingredients without clear strain identification
- No CFU count or unclear labelling
- Heavy marketing language such as “miracle”, “detox”, or “boosts immunity dramatically”
- Products sold only through social media or unverified online sources
Are probiotics safe for everyone?
Probiotics are often well tolerated, but they are not suitable for everyone.
- People who are immunocompromised or seriously unwell may be at risk of rare infections linked to probiotic organisms.
- This includes some patients with complex lung disease, those on immunosuppressive treatment, or those with central lines.
- Because of this, probiotics should be discussed with a healthcare professional before use in these groups.
What is the practical take?
- Probiotics may help some people reduce diarrhoea associated with antibiotics.
- They are not routinely recommended for everyone.
- They are not a treatment for C. diff.
- Product quality varies, so understanding labels is important.
- For people with long-term conditions such as aspergillosis, it is sensible to check before using them.
As research into the gut microbiome develops, understanding of probiotics may improve. For now, they are best seen as a possible supportive option in some situations, rather than a standard part of care.
Common questions
Can antifungals cause C. diff?
Not usually. The main recognised trigger is antibiotic exposure, not antifungal therapy. But antifungals such as itraconazole can cause diarrhoea as a side effect, which can create understandable confusion.
Could I get C. diff if I have not had antibiotics recently?
Yes, it is possible, but antibiotics are the classic and most important risk factor. Recent hospital contact and other vulnerabilities can matter too.
If my diarrhoea started after itraconazole, does that prove itraconazole caused it?
No. Timing can be a clue, but it does not prove the cause. A side effect is possible, but so are other explanations, including infection, recent antibiotics, other medicines, or unrelated bowel problems.
Could acid-suppressing tablets increase risk?
Possibly. Proton pump inhibitors have been associated with C. diff risk in some studies, but that does not prove they directly cause it.
Why this matters in aspergillosis
For aspergillosis patients, this topic matters for two reasons.
First, gut symptoms are common, especially when treatment is complex. That makes it easy to mislabel symptoms. Second, many patients have also needed antibiotics for chest infections or have had hospital admissions, which means true C. diff risk may be more relevant than it first appears.
The safest message is not “itraconazole causes C. diff” and not “it is definitely nothing serious”, but rather: know the difference, notice the red flags, and get persistent symptoms checked.
When to seek medical advice
Seek medical advice promptly if diarrhoea is:
- frequent and watery
- continuing rather than settling
- happening after recent antibiotics
- accompanied by tummy pain, fever, bleeding, or dehydration
- making you feel significantly unwell
Take-home message
Long-term itraconazole use is not a typical direct cause of C. diff. However, itraconazole can cause diarrhoea, and people with aspergillosis may still be at risk of C. diff because of recent antibiotics, hospital exposure, and other health factors.
The key is not to jump to conclusions either way: mild diarrhoea can be a medicine side effect, but persistent watery diarrhoea, pain, fever, bleeding or dehydration should be taken seriously.
Suggested internal links
- Antifungal treatment hub
- Why antibiotics do not always work
- Chronic Pulmonary Aspergillosis
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Information for professionals
References
- NHS. Clostridioides difficile (C. diff) infection.
- NICE. Clostridioides difficile infection: antimicrobial prescribing (NG199).
- BNF. Itraconazole.
- UK Health Security Agency. Clostridioides difficile guidance, data and analysis.
- UK Health Security Agency. Increase in Clostridioides difficile infections: current epidemiology data and investigations.
Author: National Aspergillosis Centre CARES Team
Epigenetics and Aspergillosis: Why Your Body Responds Differently – and What Future Treatments May Look Like
Last reviewed: April 2026
Audience: Patients, carers, GPs, specialist nurses
This article explains how the immune system, environment, and emerging research all connect. If helpful, you can explore each topic in more detail using the links throughout this page.
Key Points
- Epigenetics controls how your genes behave without changing your DNA sequence.
- It helps explain why people with similar lung disease develop different forms of aspergillosis.
- Both the human immune system and the fungus itself use epigenetic mechanisms.
- These processes influence inflammation, immune response, and treatment effectiveness.
- Future treatments may combine antifungals, biologics, and epigenetic approaches.
- There are currently no epigenetic therapies for aspergillosis in routine NHS care.
Table of Contents
- What is epigenetics?
- How epigenetics works (simple explanation)
- Why this matters in aspergillosis
- Different diseases, different immune patterns
- Damp, mould, and environmental exposure
- Why treatment works differently
- Biologics vs epigenetics
- What research is trying to do
- Epigenetics in Aspergillus itself
- What this means for the future
- Common questions
- When to seek medical advice
- References
What is epigenetics?
If you are new to aspergillosis, you may find it helpful to first read our overview of what aspergillosis is.
Epigenetics refers to changes in how your genes are used by your body, without changing the underlying DNA sequence.
You can think of your DNA as a library of instructions. Epigenetics controls:
- Which instructions are read
- When they are used
- How strongly they are activated
This allows your body to adapt to its environment—but it can also contribute to disease.
How epigenetics works (simple explanation)
There are three main mechanisms:
- DNA methylation – switches genes off
- Histone modification – controls how tightly DNA is packaged (affecting access to genes)
- MicroRNAs – fine-tune gene activity
These processes are now recognised as key regulators of immune and fungal biology
(Nie et al., 2018).
Why this matters in aspergillosis
Patients often ask:
“Why did I develop this when others didn’t?”
Epigenetics helps explain why similar exposures to Aspergillus can result in:
- Allergic disease
- Chronic infection
- No disease
This reflects differences in immune system “programming”.
Importantly, this programming is influenced by:
- Past infections
- Lung damage (e.g. COPD, TB)
- Environmental exposure
- Medications
Is the body “testing” responses before they become permanent?
It can sometimes feel as though the body is “trying out” different ways of responding to infection or environmental exposure.
This idea comes close to how epigenetics works—but it is important to understand it carefully.
A useful way to think about it
Epigenetics allows the body to rapidly adjust how genes behave in response to the environment. This can happen over days, months, or years, and may influence how the immune system reacts to fungi such as Aspergillus.
In this sense, epigenetics can be thought of as allowing the body to explore different “settings” of immune response—for example:
- A stronger allergic response (as seen in ABPA)
- A weaker or less effective response (as seen in CPA)
- A balanced response with minimal symptoms
What epigenetics does not do
It is important to be clear that the body is not deliberately “testing” changes in a planned way, and epigenetic changes are not directly converted into permanent genetic mutations.
Instead:
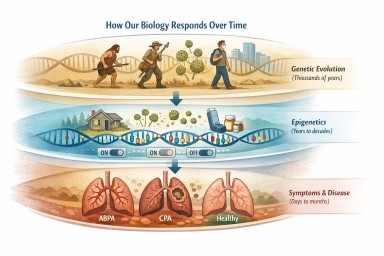
- Epigenetic changes are fast and flexible
- Genetic changes (mutations) occur slowly and randomly
- Natural selection acts over long timescales to favour traits that improve survival
How the two processes connect
Although separate, epigenetics and evolution can interact over time.
If a particular way of responding to infection is consistently helpful, individuals whose genes naturally produce a similar response may be more likely to thrive over generations.
This means:
- Epigenetics shapes how the body responds in the short term
- Evolution shapes which responses persist in the long term
Why this matters in aspergillosis
This helps explain why:
- Different people respond very differently to the same fungal exposure
- Symptoms can change over time
- Modern environments (such as damp housing or long-term steroid use) may produce responses that our immune systems were not originally adapted for
Can epigenetic changes be inherited?
Most epigenetic changes happen within a single lifetime and are not passed on to children. However, there is growing evidence that some epigenetic changes may persist or be transmitted across generations under certain conditions.
This is sometimes called transgenerational epigenetic inheritance.
For example, research suggests that:
- Environmental exposures (such as diet, stress, or infection) may leave lasting epigenetic marks
- Some of these marks may influence how genes behave in the next generation
- This effect is usually partial and not always predictable
In humans, this area is still being studied, and the extent to which epigenetic changes are inherited remains uncertain.
What this means in practice
It is important not to overinterpret this idea:
- Epigenetic inheritance is not a replacement for genetic inheritance
- Most traits and diseases are still determined by DNA and environment
- There is currently no evidence that conditions like aspergillosis are directly passed on through epigenetic changes
However, this research does suggest that environment and health may have longer-term effects than previously thought, potentially influencing future generations in subtle ways.
In simple terms:
Epigenetics allows the body to adapt quickly. Evolution determines what lasts.
Different diseases, different immune patterns
See also:
Allergic pattern (ABPA)
- Strong Th2 immune response
- High IgE and eosinophils
- Exaggerated reaction to fungal spores
Epigenetic changes may increase expression of cytokines such as IL-4, IL-5, and IL-13, driving allergic inflammation.
Chronic infection pattern (CPA)
- Reduced ability to clear fungus
- Persistent infection in damaged lung areas
- Chronic inflammation and tissue damage
Epigenetic changes may “lock in” ineffective immune responses.
Damp, mould, and environmental exposure
Long-term exposure to damp and mould is highly relevant.
It may:
- Alter airway cell behaviour
- Increase sensitivity to fungal spores
- Promote ongoing inflammation
These effects may persist through epigenetic changes, even after exposure is reduced.
See:
Why treatment works differently
Epigenetics may explain why patients respond differently to treatment.
- Some respond well to steroids
- Others develop resistance or side effects
- Biologic response varies between individuals
A key mechanism involves reduced activity of enzymes such as histone deacetylase 2 (HDAC2), which is important for steroid response.
See also: Why antibiotics do not always work
Biologics vs epigenetics
Biologics
- Target specific immune signals (e.g. IgE, IL-5)
- Fast and precise
- Widely used in severe asthma and ABPA
Epigenetics
- Acts at a deeper level
- Influences multiple pathways
- May create longer-lasting effects
Epigenetics is unlikely to replace biologics—it is more likely to enhance and personalise them.
What research is trying to do
1. Restoring steroid sensitivity
Research is exploring how to restore HDAC2 activity and improve steroid effectiveness.
2. Trained immunity (immune memory)
Immune cells can be “trained” by past exposures. This may lead to:
- Better defence
- Or harmful chronic inflammation
Scientists are studying how to reset this balance.
3. MicroRNA biomarkers
MicroRNAs may help predict:
- Disease severity
- Risk of relapse
- Treatment response
4. Metabolic and immune reprogramming
Immune cell metabolism is closely linked to epigenetic regulation. Modifying this may improve immune function.
Epigenetics in Aspergillus itself
The fungus is not passive—Aspergillus fumigatus also uses epigenetic control.
This influences:
- Virulence (how aggressive it is)
- Biofilm formation
- Resistance to antifungal drugs
Recent research shows that epigenetic regulators directly affect fungal interaction with the host
(Liu et al., 2026).
Other studies show control of toxin production and colonisation
(Hao et al., 2023).
What this means for the future
The most realistic model is layered care:
- Antifungals
- Steroids
- Biologics
- Environmental control
- Future epigenetic approaches
Epigenetics may:
- Improve treatment response
- Reduce relapse
- Enable personalised care
These approaches are still in development.
Common Questions
Can I change my epigenetics?
Not directly. However, reducing damp exposure and maintaining general health may support better immune regulation.
Are these treatments available?
No. They are still in research.
Why do my symptoms fluctuate?
Immune regulation changes over time. Epigenetics may contribute alongside infection and exposure.
Is this the next generation of treatment?
It is better seen as an additional layer that may improve existing treatments.
When to seek medical advice
- Worsening breathlessness
- Increased cough
- Chest pain
- Weight loss
- Sudden symptom changes
This article is for education and does not replace clinical advice.
References
- Liu H et al. (2026)
- Nie X et al. (2018)
- Hao L et al. (2023)
- BTS Clinical Statement
- ISHAM Guidelines
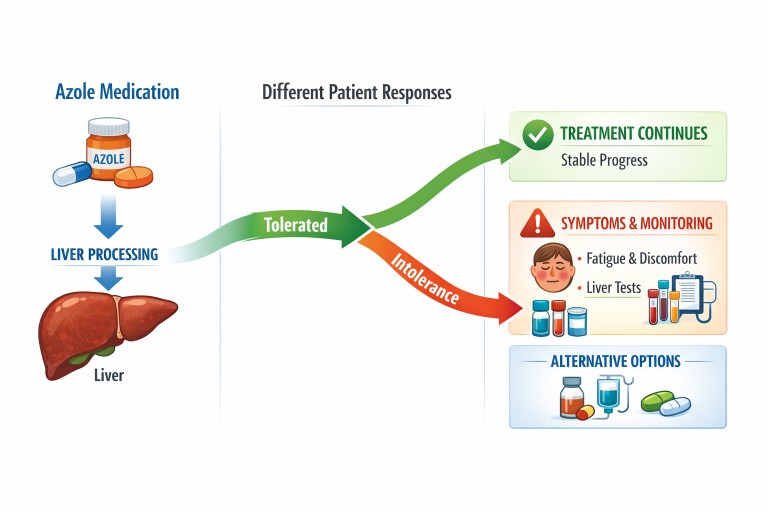
What if you can’t tolerate azole antifungal medicines?
Key points

- Azole antifungals are commonly used to treat aspergillosis, but not everyone tolerates them well.
- “Azole intolerance” means the body reacts badly to the medication, even if it is otherwise effective.
- Symptoms can include fatigue, flushing, shaking, nausea, and discomfort around the liver area.
- In some cases, blood tests show changes in liver function.
- If azoles are not tolerated, there are often alternative approaches your clinical team can consider.
Contents
- What are azole antifungals?
- What is azole intolerance?
- Why does azole intolerance happen?
- Common symptoms to look out for
- The role of the liver
- What can be done if azoles are not tolerated?
- Why monitoring is important
- Common questions
- When to seek medical advice
What are azole antifungals?
Azole antifungals are a group of medicines used to treat fungal infections such as aspergillosis. They work by interfering with the fungal cell membrane, helping to stop the fungus growing.
Common examples include:
- Fluconazole
- Itraconazole
- Voriconazole
- Posaconazole
They are often used long-term in conditions like chronic pulmonary aspergillosis (CPA) or allergic bronchopulmonary aspergillosis (ABPA).
What is azole intolerance?
Azole intolerance means that a person develops unpleasant or harmful side effects when taking these medications, even at standard doses.
This is different from:
- Allergy – an immune reaction (e.g. rash, swelling, breathing difficulty)
- Resistance – when the fungus is not affected by the drug
With intolerance, the drug may still work against the fungus—but the body cannot tolerate its effects.
Why does azole intolerance happen?
There is no single cause. Instead, several factors can contribute:
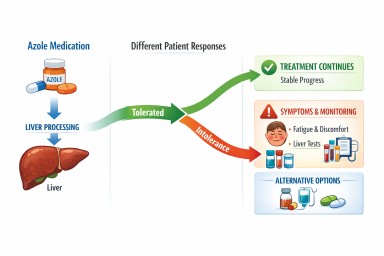
1. How the body processes the drug
Azoles are broken down in the liver. People vary in how efficiently this happens, which can lead to higher levels of the drug in the body.
2. Effects on liver enzymes
Azoles affect enzymes (called cytochrome P450 enzymes) that are involved in processing many medications. This can:
- Increase drug levels
- Cause interactions with other medications
- Put strain on the liver
3. Individual sensitivity
Some people are simply more sensitive to these drugs, even when blood levels are within the expected range.
4. Other health factors
- Existing liver conditions
- Age
- Other medications
- Nutritional status
Common symptoms to look out for
Patients describe a range of symptoms when azoles are not well tolerated, including:
- Flushed or hot cheeks
- Shaking or tremor
- Severe fatigue
- Nausea or reduced appetite
- Discomfort or pain in the upper abdomen, back, or sides (where the liver sits)
- General feeling of being unwell
These symptoms can appear soon after starting treatment or develop over time.
The role of the liver
The liver plays a central role in processing azole antifungals.
In some cases, this can lead to:
- Raised liver enzymes on blood tests
- Inflammation or irritation of the liver
It is important to note that:
- Some people have abnormal blood tests without symptoms
- Others feel unwell even when tests are only mildly changed
This is why both symptoms and blood tests are considered together.
What can be done if azoles are not tolerated?
If azole intolerance is suspected, your clinical team may consider several approaches:
Adjusting treatment
- Reducing the dose
- Changing how the medication is taken (e.g. with food)
Switching to another azole
Some people tolerate one azole better than another.
Therapeutic drug monitoring (TDM)
Blood tests can measure drug levels to help ensure they are not too high or too low.
Considering non-azole treatments
In some cases, different classes of antifungal medication may be considered.
The best approach depends on the individual, the condition being treated, and how severe the side effects are.
Why monitoring is important
Because azoles affect the liver and interact with other medications, monitoring is a routine part of care.
This may include:
- Regular liver function blood tests
- Drug level monitoring (for some azoles)
- Review of other medications
Monitoring helps detect problems early and allows treatment to be adjusted safely.
Common questions
Does intolerance mean I cannot take any antifungal treatment?
No. Many patients who cannot tolerate one medication can use another, or a different approach may be possible.
Will the symptoms settle if I continue?
In some cases mild symptoms improve, but persistent or worsening symptoms should always be reviewed.
Is this common?
Most people tolerate azoles reasonably well, but intolerance is recognised and not rare in specialist clinics.
When to seek medical advice
You should contact your healthcare team if you experience:
- Persistent or worsening fatigue
- Pain in the upper abdomen, back, or sides
- Nausea affecting eating or drinking
- New or unusual symptoms after starting medication
Seek urgent medical attention if you notice:
- Yellowing of the skin or eyes (jaundice)
- Dark urine or pale stools
- Severe abdominal pain
Summary
Azole antifungals are an important part of treating aspergillosis, but some people experience intolerance.
This is usually related to how the body processes the medication—particularly in the liver—and varies from person to person.
If intolerance occurs, it does not mean that treatment options have run out. With careful monitoring and specialist input, alternative strategies can often be found.
Further reading
- Chronic pulmonary aspergillosis (CPA)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Information for healthcare professionals
Author & review
This article has been prepared for patients and carers using information aligned with UK specialist practice, including the National Aspergillosis Centre (Manchester, UK).
Important: This content is for general educational purposes only and is not a substitute for medical advice. Always speak to your healthcare team about your own situation.
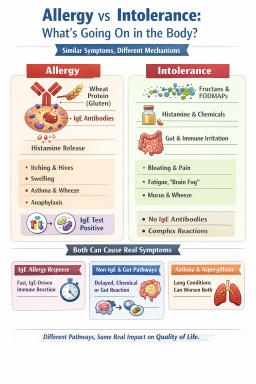
Allergy, Intolerance and Wheat Reactions: What Is Actually Going On?
Key points
- You can have real and sometimes severe symptoms without having a classic allergy.
- Allergy, intolerance, and non-IgE reactions involve different biological pathways.
- Similar symptoms (such as wheeze or mucus) do not always mean the same cause.
- The term “intolerance” is often used as a catch-all, which can be confusing.
- For people with lung conditions, triggers may still worsen symptoms even when allergy tests are negative.
This article is general educational information for patients and carers. If you are new to this topic, you may wish to start with our overview of what is aspergillosis or explore common symptoms affecting the lungs and airways.
Contents
- Why this is so confusing
- What is a true allergy?
- What is an intolerance?
- The grey area: non-IgE reactions
- Wheat as an example
- Why “downgraded” feels upsetting
- Why this matters in asthma and aspergillosis
- Why testing is often limited
- What usually happens next?
- Take-home message
- When to seek medical advice
Why this is so confusing
Many people use the word “allergy” to describe any reaction to food or environmental triggers. This is understandable, because the symptoms can feel very similar.
For example:
- wheeze or chest tightness
- increased mucus and respiratory symptoms
- bloating or abdominal discomfort
- fatigue or “brain fog”
However, similar symptoms do not always mean the same biological cause. This is where confusion begins.
What is a true allergy?
A true allergy usually refers to an IgE-mediated immune reaction.
This means the immune system reacts quickly to a substance, often within minutes to a couple of hours. Symptoms may include:
- itching or hives
- swelling
- wheeze (see asthma and airway symptoms)
- vomiting
- in severe cases, anaphylaxis
This type of reaction is what most allergy clinics are designed to detect, because it can be serious and is usually testable.
What is an intolerance?
An intolerance is a broader term used when symptoms do not follow the classic IgE allergy pathway.
It may involve:
- digestive processes
- food chemicals such as histamine or salicylates
- gut–immune interactions
- non-specific inflammation
Importantly: intolerance does not mean “mild” or “unimportant”. It simply means the mechanism is different and often harder to measure.
For guidance on managing food-related symptoms, see our diet and nutrition hub.
The grey area: non-IgE reactions
Not all immune reactions involve IgE.
Some reactions involve other parts of the immune system and may be:
- delayed
- longer lasting
- harder to detect with standard tests
This creates a grey area between “allergy” and “intolerance”.
This is why the statement:
“Same symptoms but no IgE = intolerance”
is often an oversimplification.
Wheat as an example
Wheat reactions are often used to illustrate this complexity:
- Wheat allergy → IgE reaction to wheat proteins
- Coeliac disease → autoimmune condition (see NICE guidance)
- Non-coeliac wheat sensitivity → unclear mechanism
- Carbohydrate intolerance → reaction to fructans (FODMAPs)
All of these may cause symptoms, but they require different ways of understanding and managing.
Why “downgraded” feels upsetting
Patients are sometimes told they have been “downgraded” from allergy to intolerance.
In reality, what has usually happened is:
- a classic IgE allergy has been considered unlikely
- testing is unlikely to add further information
- the reaction falls into a less clearly defined category
This is a change in classification, not a judgement about importance or severity.
Why this matters in asthma and aspergillosis
For people with asthma, Allergic Bronchopulmonary Aspergillosis (ABPA), or chronic pulmonary aspergillosis (CPA):
- airways are often more sensitive
- inflammation may already be present
This means that triggers do not always need to be classic allergens to cause problems.
Symptoms such as wheeze, mucus and chest tightness may worsen even when allergy tests are negative.
You may also find it helpful to read why antibiotics do not always work, which explains how non-bacterial causes can drive ongoing symptoms.
Why testing is often limited
Allergy testing works best for IgE-mediated conditions.
For many other reactions:
- there are no simple validated tests
- diagnosis relies more on clinical history and patterns
Further detail for clinicians and advanced readers is available in our information section for patients.
What usually happens next?
After a classic allergy has been ruled out, the process does not stop—it changes direction.
Understanding patterns
The focus often shifts to identifying:
- what triggers symptoms
- how quickly symptoms occur
- whether effects are delayed or cumulative
Identifying the main system involved
- Gut-related → bloating, pain, bowel symptoms
- Airway-related → wheeze, mucus, chest tightness
- Mixed/systemic → fatigue and general symptoms
Different types of support
Depending on the pattern, support may involve:
- dietary approaches (nutrition guidance)
- respiratory care (asthma management)
- specialist review (e.g. CPA services)
This stage is often less clear-cut but can still lead to meaningful improvements over time.
Take-home message
- Allergy and intolerance are not the same.
- “Intolerance” is often used as a broad label.
- Symptoms may be similar, but the underlying pathways differ.
- This affects how conditions are understood and managed.
- Even without a clear label, symptoms remain real and important.
When to seek medical advice
Seek urgent help if you develop:
- sudden breathing difficulty
- swelling of the lips, tongue or throat
- collapse or severe dizziness
Arrange medical review if you have:
- persistent or worsening symptoms
- repeated reactions to foods or triggers
- worsening respiratory symptoms
Related topics
- Asthma and airway inflammation
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Chronic Pulmonary Aspergillosis (CPA)
- Understanding symptoms
- Diet and food triggers
- Why antibiotics do not always work
References
- NHS – Food allergy and intolerance
- BSACI – Food allergy guidance
- NICE NG20 – Coeliac disease
Last reviewed: April 2026
Author: Aspergillosis Website Team
Review status: Educational content for patients and carers
Help us understand how damp homes affect health

We are supporting a UK research project looking at how damp homes may affect health, including respiratory health and conditions such as aspergillosis.
This study is being led by the National Aspergillosis Centre at Manchester University NHS Foundation Trust, and is being shared through aspergillosis.org to support research into damp homes and health.
We are currently inviting people across the UK to register their interest in taking part.
Registering your interest should take less than one minute and does not commit you to taking part.
Why this matters
Damp and mould are often linked to health problems, but there is still limited real-world evidence from people’s homes across the UK.
This project aims to help improve understanding of how home environments may affect health by gathering information from people living in a wide range of housing conditions.
Who can register interest?
We would like to hear from people living in the UK, including:
- people with lung or respiratory conditions
- people without any known lung or breathing condition
- people who have experienced damp or mould at home
- people who have not experienced damp or mould at home
- members of the general public who would like to contribute to the research
We are keen to hear from people with different health backgrounds and a wide range of home environments.
What is the study about?
This research is exploring how damp homes may affect health. The aim is to improve understanding of the relationship between home environments and health symptoms in real-world settings.
This project is for research purposes only and does not provide medical advice or diagnosis.
What might taking part involve later?
If the study opens, some people who register interest may later be invited to:
- complete a short questionnaire about their home and health symptoms
- receive a simple home sampling kit by post
- collect and return a small household sample, for example dust from the home, for research purposes
The home sampling part is intended to be simple and practical. Full instructions would be provided.
Registering your interest now does not commit you to taking part later.
Important information
- Registering interest is voluntary.
- You do not have to take part in the full study later.
- Your details will only be used to contact you about this project.
- Your data will be handled in line with UK data protection regulations.
- You can decide later whether or not to take part.
Frequently asked questions
Am I signing up to take part in the study now?
No. At this stage, you are only registering your interest in hearing more about the study.
Do I need to have a lung condition to register interest?
No. We would like to hear from people with and without lung conditions.
Do I need to have damp or mould in my home?
No. We are interested in hearing from people with a wide range of home environments and experiences.
Will I definitely receive a kit?
Not necessarily. Registering interest helps the research team understand the level of interest and contact people if the study opens.
Will I get personal results about my home or health?
At this stage, no individual results are being promised. More information would be provided if the study proceeds.
What happens after I register interest?
You do not need to do anything further straight away. If the study opens, you may be contacted with more information so you can decide whether you would like to take part.
Register your interest
Ready to help? Complete the form below.
This secure form should take less than one minute to complete.
If the form does not load, you can open it here:
Open the form in a new window
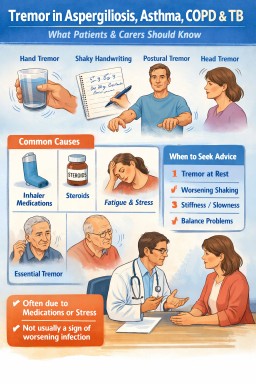
Tremor (Shaking) in Aspergillosis, Asthma, COPD and TB: Causes, Meaning and When to Seek Help
Last reviewed: 16 April 2026
For: Patients, carers, general practitioners, nurses and non-specialists
Topic: Tremor (shaking) in aspergillosis, asthma, Chronic Obstructive Pulmonary Disease (COPD) and tuberculosis (TB)
Shaking or tremor can feel alarming, but in most people with lung conditions it has a clear and manageable cause.
Key points
- A tremor is a shaking movement, usually affecting the hands.
- In people with aspergillosis, asthma, Chronic Obstructive Pulmonary Disease (COPD) or tuberculosis (TB), tremor is usually not caused by the lung condition itself.
- The most common causes are medications, breathlessness, stress, fatigue, weakness, or an unrelated tremor condition such as essential tremor.
- Reliever inhalers such as salbutamol commonly cause a fine shaking of the hands.
- Antifungal medicines can sometimes contribute to tremor directly or through drug interactions.
- Biologic treatments used for severe asthma are not usually a cause of tremor and may sometimes reduce tremor indirectly by lowering steroid or reliever inhaler use.
- Most tremors in this setting do not mean the underlying disease is worsening.
- A new tremor should still be mentioned to a healthcare professional, especially if it is worsening, happens at rest, or comes with stiffness, slowness or balance problems.
Contents
- What is a tremor?
- Why can it happen in lung conditions?
- What sort of tremor might it be?
- What is essential tremor?
- Is it Parkinson’s disease?
- Do biologics play a part?
- Will it get worse?
- What can help?
- When to seek medical advice
- Common questions
- References
If you are newly diagnosed, you may find it helpful to start with our overview of what aspergillosis is and how it affects the lungs, as well as our broader guide to information for patients and carers.
What is a tremor?
A tremor is an involuntary shaking movement. It most often affects the hands, but it can also affect the head, jaw or voice. People may notice it when holding a cup, using cutlery, writing, typing, or holding their arms out in front of them.
Tremor can be worrying, especially if it is new. Some people fear it means their infection is spreading, their lungs are failing, or they are developing Parkinson’s disease. In most people with respiratory conditions, that is not the case.
Why can it happen in lung conditions?
For most people with aspergillosis, asthma, Chronic Obstructive Pulmonary Disease (COPD) or tuberculosis (TB), tremor is usually explained by one or more of the following:
1. Medications
This is the most common explanation. Reliever inhalers such as salbutamol are well known to cause a fine tremor, especially in the hands. Steroids can also make people feel shaky, wired, weak or restless. In people with aspergillosis, antifungal medicines such as itraconazole or voriconazole may sometimes contribute to tremor or make it more noticeable, particularly if they interact with other medicines.
If you are taking antifungal medication, you may also find it helpful to read our guide to antifungal treatments and side effects, including how different drugs can interact with each other.
2. Breathlessness, stress and adrenaline
When the body is under strain, trembling can become more noticeable. Breathlessness, anxiety, poor sleep, infection, inflammation and exhaustion can all amplify the body’s normal background tremor.
3. Fatigue and muscle weakness
Muscles that are tired or weakened tend to shake more easily. This can happen in chronic respiratory disease, after infections, during recovery, or after long periods of reduced activity.
People living with long-term conditions such as Chronic Pulmonary Aspergillosis (CPA) may experience fatigue and reduced muscle strength, both of which can make tremor more noticeable.
4. An unrelated tremor condition
Some people have a separate condition such as essential tremor. This may have been mild for years and only become noticeable during a period of illness, stress, treatment changes or increased reliever inhaler use.
5. Less common neurological causes
Less commonly, tremor may be due to a neurological condition such as Parkinson’s disease or to another medical problem such as thyroid disease, low blood sugar, or medication side effects from medicines unrelated to the lungs. This is why a new tremor should not be ignored, even though the cause is often straightforward.
What sort of tremor might it be?
The type of tremor can give useful clues.
Action or postural tremor
This is the most common type in people with lung disease. It appears when using the hands or holding them in a position, such as lifting a drink, eating, writing, or stretching the arms out. This pattern often fits tremor linked to salbutamol, stress, fatigue, steroids, or essential tremor.
Enhanced physiological tremor
Everyone has a tiny natural tremor. Illness, adrenaline, fatigue, caffeine, poor sleep, fever, pain and some medicines can make it much more obvious. This often causes a fine, fast, variable shakiness.
Essential tremor
This is a common neurological condition that usually causes shaking during movement or when holding a posture. It often affects both hands and may slowly become more noticeable over time.
Rest tremor
This happens when the hand is fully relaxed and not being used. A true rest tremor is less typical of inhaler- or stress-related shaking, so it deserves more careful assessment.
What is essential tremor?
Essential tremor is one of the most common movement disorders. It usually affects both hands, although one side can be worse than the other. It tends to happen during action rather than complete rest. Some people also notice tremor of the head or voice.
Essential tremor is not caused by aspergillosis, asthma, Chronic Obstructive Pulmonary Disease (COPD) or tuberculosis (TB). However, illness, tiredness, anxiety, reliever inhalers and medication changes can all make an underlying essential tremor more obvious.
For many people, essential tremor remains mild for years. It can slowly worsen over time, but it does not usually turn into Parkinson’s disease.
Is it Parkinson’s disease?
Most tremor in respiratory patients is not Parkinson’s disease. Parkinson’s disease usually causes a different pattern, often with tremor at rest, stiffness, slowness, reduced arm swing, or changes in walking. A tremor that only happens after inhaler use or when someone is tired, anxious or unwell is less suggestive of Parkinson’s disease.
That said, not every tremor in a person with lung disease should be blamed on medications. If the tremor is clearly happening at rest, is becoming more obvious over time, or is linked with stiffness or slowed movement, it should be assessed properly.
Do biologics play a part?
Biologic treatments used for severe asthma and some cases of Allergic Bronchopulmonary Aspergillosis (ABPA), such as omalizumab, mepolizumab, benralizumab and dupilumab, are not usually associated with tremor. They are much less likely to cause shaking than reliever inhalers or steroids.
If you are receiving advanced asthma treatments, you can read more in our guide to biologic therapies for asthma and ABPA, which explains how these treatments work and what side effects to expect.
In practice, biologics may sometimes help indirectly. If they improve asthma control, reduce flare-ups, lower oral steroid use, or reduce the need for frequent salbutamol, tremor may improve rather than worsen.
If someone develops shaking while on a biologic, it is usually sensible to look first at the broader picture: reliever inhaler use, steroid dose, antifungal treatment, other medicines, fatigue, anxiety, and whether the tremor started after a different medication change.
Will it get worse?
Often, the answer is reassuring: not necessarily.
If the tremor is linked to salbutamol or another medicine
It may improve once the dose is reduced, the timing is adjusted, the medicine is changed, or the underlying breathing problem is better controlled. Some medication-related tremors fluctuate rather than steadily worsening.
If the tremor is linked to illness, fatigue or stress
It often comes and goes. It may be worse during flare-ups, infections, poor sleep, low mood, pain or periods of worry, and better on good days.
If it is essential tremor
Essential tremor can slowly progress over time, but this usually happens over years rather than days or weeks. Many people remain stable for long periods.
If it is Parkinson’s disease or another neurological cause
That requires separate assessment. It is much less common than action tremor related to medicines or illness in respiratory patients, but it should be considered when the pattern fits.
Overall, a tremor does not usually mean aspergillosis, asthma, Chronic Obstructive Pulmonary Disease (COPD) or tuberculosis (TB) is worsening in the lungs.
If your symptoms have been difficult to control, it may also help to read why chest infections do not always improve with antibiotics, particularly in conditions such as aspergillosis.
What can help?
- Notice when the tremor happens: after inhalers, when tired, during stress, or all the time.
- Keep a note of recent treatment changes, including inhalers, steroids, antifungals and any new tablets.
- Check whether the tremor happens during action, at rest, or both.
- Try to reduce obvious triggers where possible, such as exhaustion, missed meals, dehydration and excess caffeine.
- Ask for a medication review if the tremor is new or troublesome.
- If you have asthma or Chronic Obstructive Pulmonary Disease (COPD), discuss whether frequent reliever inhaler use means your maintenance treatment needs reviewing.
When to seek medical advice
Speak to your healthcare team if:
- the tremor is new, persistent, or getting worse
- it started after a change in medication
- it is affecting eating, drinking, writing or daily activities
- it happens when your hands are fully at rest
- you also notice stiffness, slowed movement, poor balance, falls, or changes in walking
- you feel generally unwell, confused, very weak, or have other new neurological symptoms
Reassurance for patients and carers
Tremor can be unsettling, but it is common and often explainable. In people living with aspergillosis, asthma, Chronic Obstructive Pulmonary Disease (COPD) or tuberculosis (TB), the cause is usually medication effects, body stress, fatigue, or an unrelated essential tremor rather than the lung condition itself damaging the nervous system.
That means there is often room to improve things: inhalers can be reviewed, other medicines checked, triggers reduced, and the tremor pattern assessed properly. Most importantly, a tremor does not automatically mean the worst.
Related topics:
Common questions
Does aspergillosis itself cause tremor?
Usually no. Tremor in people with aspergillosis is much more likely to be related to medication, fatigue, illness, anxiety, or a separate tremor condition.
Can salbutamol make you shake?
Yes. This is a very well recognised side effect. It usually causes a fine tremor in the hands.
Can antifungal treatment cause tremor?
It can in some people, either directly or through interactions with other medicines. If tremor appears after starting or changing antifungal treatment, it is worth raising.
Do biologics usually cause tremor?
No. Biologics are not a common cause of tremor and may sometimes reduce tremor indirectly by improving control and reducing the need for steroids or frequent reliever inhalers.
Will this definitely get worse?
No. Many tremors stay mild, fluctuate, or improve when the cause is identified and managed.
References
- British National Formulary (BNF) – Salbutamol
Describes common side effects of beta-2 agonists, including tremor and shakiness.
https://bnf.nice.org.uk/drugs/salbutamol/ - NHS – Tremor
Overview of tremor types, causes, and when to seek medical advice.
https://www.nhs.uk/conditions/tremor/ - NHS / Neurology Guidance – Essential Tremor
Clinical overview of essential tremor, including action/postural tremor characteristics and distinction from Parkinson’s disease.
https://rightdecisions.scot.nhs.uk/neurology-pathways-including-headache/gp-factsheets/essential-tremor/ - Electronic Medicines Compendium (eMC) – Voriconazole (Vfend) Summary of Product Characteristics
Details neurological side effects and drug interaction potential of voriconazole.
https://www.medicines.org.uk/emc/product/7981/smpc - Electronic Medicines Compendium (eMC) – Itraconazole Summary of Product Characteristics
Provides prescribing information, including neurological effects and interactions.
https://www.medicines.org.uk/emc/search?q=itraconazole - NICE Guidance – Asthma (NG80)
Covers pharmacological management of asthma, including use of bronchodilators and biologics.
https://www.nice.org.uk/guidance/ng80 - NICE Technology Appraisals – Biologic therapies for severe asthma
Includes guidance on omalizumab, mepolizumab, benralizumab and dupilumab.
https://www.nice.org.uk/guidance/ta278 - NHS – Parkinson’s Disease
Overview of symptoms including resting tremor, stiffness and slowed movement.
https://www.nhs.uk/conditions/parkinsons-disease/
Author note: This article is for general education and is not a substitute for individual medical advice. People with new, worsening or unexplained tremor should discuss it with their usual healthcare professional.
You can explore more topics like this in our latest patient questions and answers, where we regularly explain common symptoms and concerns raised by people living with aspergillosis and other lung conditions.
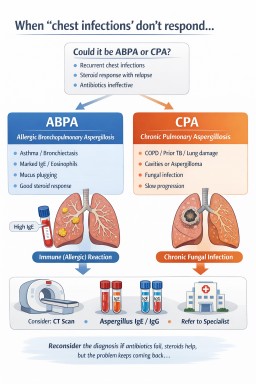
When ‘chest infections’ don’t respond: when to suspect ABPA or CPA (Clinical perspective)
Patients presenting with recurrent “chest infections” that do not respond to antibiotics are common in primary and secondary care. In a subset of these cases, the underlying cause may not be bacterial, but related to fungal disease or immune-mediated responses to Aspergillus.
This article summarises when to suspect allergic bronchopulmonary aspergillosis (ABPA) or chronic pulmonary aspergillosis (CPA), and how to move from repeated empirical treatment to a more structured diagnostic approach.
Key clinical message
Repeated antibiotic-treated exacerbations with limited response, particularly when symptoms improve with steroids and then relapse, should prompt reconsideration of the diagnosis.
When to suspect ABPA or CPA
Consider aspergillosis-related disease in patients with:
- Recurrent “chest infections” with poor or inconsistent antibiotic response
- Steroid-responsive symptoms with relapse on reduction or cessation
- Persistent or unexplained radiological abnormalities
- Underlying lung disease:
- Asthma
- Bronchiectasis
- Chronic obstructive pulmonary disease (COPD)
- Previous tuberculosis or lung damage
- Raised or previously documented abnormalities in:
- Total IgE
- Eosinophils
- Aspergillus-specific markers (if previously tested)
These features are not diagnostic in isolation but should raise suspicion when seen together.
ABPA vs CPA: clinical distinction
| Feature | ABPA | CPA |
|---|---|---|
| Primary mechanism | Immune-mediated (allergic) | Chronic fungal infection |
| Typical background | Asthma, bronchiectasis | Structural lung disease, prior TB, COPD |
| Steroid response | Often marked | Variable (may improve symptoms but not disease) |
| Antibiotic response | Limited | Limited |
| Radiology | Mucus plugging, bronchiectasis | Cavities, fungal balls, fibrosis |
Common pitfalls in practice
- Repeated empirical antibiotics despite poor response
- Short courses of steroids without a long-term management plan
- Reliance on chest X-ray alone in persistent or atypical cases
- Failure to recognise patterns across multiple consultations or admissions
These patterns can lead to prolonged diagnostic delay, which is well described in CPA and ABPA.
Suggested diagnostic approach
1. Reassess the working diagnosis
When standard treatment fails, explicitly reconsider whether the presentation remains consistent with bacterial infection.
2. Imaging
- Escalate from chest X-ray to CT thorax where appropriate
- Look for:
- Cavitation
- Fungal ball (aspergilloma)
- Mucus plugging
- Bronchiectasis
3. Blood tests
- Total IgE
- Eosinophil count
- Aspergillus-specific IgE and IgG (where available)
4. Microbiology / further testing
Depending on context, consider sputum culture, fungal markers, or specialist input.
The steroid–relapse pattern
A common clinical scenario:
Exacerbation → steroids → improvement → relapse
This should raise suspicion of an underlying inflammatory or fungal-driven process rather than recurrent bacterial infection alone.
When to consider referral
Referral to a specialist centre (e.g. National Aspergillosis Centre, Manchester) may be appropriate where:
- Diagnosis remains uncertain
- Symptoms are persistent or progressive despite treatment
- Antifungal therapy is being considered or not tolerated
- Radiology suggests CPA or complex disease
Referral decisions should be made in the context of overall patient condition, comorbidities, and goals of care.
Why diagnosis is often delayed
- Overlap with common respiratory conditions
- Partial response to standard therapies
- Fragmentation across care settings
- Limited exposure to aspergillosis in routine practice
Recognising the pattern is often the key step in reducing delay.
Practical takeaways
- If antibiotics are not working, reconsider the diagnosis
- If steroids repeatedly improve symptoms, ask why
- Use CT imaging to clarify persistent abnormalities
- Aim for a clear, shared management plan
Guidelines and further reading
- British Thoracic Society. Clinical Statement on Aspergillus-related chronic lung disease
- ISHAM Working Group. Guidelines for ABPA diagnosis and management
- Denning DW et al. Chronic pulmonary aspergillosis guidelines
Further professional resources
Aspergillosis.org – Information for healthcare professionals
This article is intended for educational purposes and should be interpreted in the context of individual clinical judgement.
When ‘chest infections’ don’t respond: when to suspect ABPA or CPA (Patient guide)
Patients presenting with recurrent “chest infections” that do not respond to antibiotics are common in primary and secondary care. In a subset of these cases, the underlying cause may not be bacterial, but related to fungal disease or immune-mediated responses to Aspergillus.
This article summarises when to suspect allergic bronchopulmonary aspergillosis (ABPA) or chronic pulmonary aspergillosis (CPA), and how to move from repeated empirical treatment to a more structured diagnostic approach.
Key clinical message
Repeated antibiotic-treated exacerbations with limited response, particularly when symptoms improve with steroids and then relapse, should prompt reconsideration of the diagnosis.
When to suspect ABPA or CPA
Consider aspergillosis-related disease in patients with:
- Recurrent “chest infections” with poor or inconsistent antibiotic response
- Steroid-responsive symptoms with relapse on reduction or cessation
- Persistent or unexplained radiological abnormalities
- Underlying lung disease:
- Asthma
- Bronchiectasis
- Chronic obstructive pulmonary disease (COPD)
- Previous tuberculosis or lung damage
- Raised or previously documented abnormalities in:
- Total IgE
- Eosinophils
- Aspergillus-specific markers (if previously tested)
These features are not diagnostic in isolation but should raise suspicion when seen together.
ABPA vs CPA: clinical distinction
| Feature | ABPA | CPA |
|---|---|---|
| Primary mechanism | Immune-mediated (allergic) | Chronic fungal infection |
| Typical background | Asthma, bronchiectasis | Structural lung disease, prior TB, COPD |
| Steroid response | Often marked | Variable (may improve symptoms but not disease) |
| Antibiotic response | Limited | Limited |
| Radiology | Mucus plugging, bronchiectasis | Cavities, fungal balls, fibrosis |
Common pitfalls in practice
- Repeated empirical antibiotics despite poor response
- Short courses of steroids without a long-term management plan
- Reliance on chest X-ray alone in persistent or atypical cases
- Failure to recognise patterns across multiple consultations or admissions
These patterns can lead to prolonged diagnostic delay, which is well described in CPA and ABPA.
Suggested diagnostic approach
1. Reassess the working diagnosis
When standard treatment fails, explicitly reconsider whether the presentation remains consistent with bacterial infection.
2. Imaging
- Escalate from chest X-ray to CT thorax where appropriate
- Look for:
- Cavitation
- Fungal ball (aspergilloma)
- Mucus plugging
- Bronchiectasis
3. Blood tests
- Total IgE
- Eosinophil count
- Aspergillus-specific IgE and IgG (where available)
4. Microbiology / further testing
Depending on context, consider sputum culture, fungal markers, or specialist input.
The steroid–relapse pattern
A common clinical scenario:
Exacerbation → steroids → improvement → relapse
This should raise suspicion of an underlying inflammatory or fungal-driven process rather than recurrent bacterial infection alone.
When to consider referral
Referral to a specialist centre (e.g. National Aspergillosis Centre, Manchester) may be appropriate where:
- Diagnosis remains uncertain
- Symptoms are persistent or progressive despite treatment
- Antifungal therapy is being considered or not tolerated
- Radiology suggests CPA or complex disease
Referral decisions should be made in the context of overall patient condition, comorbidities, and goals of care.
Why diagnosis is often delayed
- Overlap with common respiratory conditions
- Partial response to standard therapies
- Fragmentation across care settings
- Limited exposure to aspergillosis in routine practice
Recognising the pattern is often the key step in reducing delay.
Practical takeaways
- If antibiotics are not working, reconsider the diagnosis
- If steroids repeatedly improve symptoms, ask why
- Use CT imaging to clarify persistent abnormalities
- Aim for a clear, shared management plan
Guidelines and further reading
Which guideline should I use?
In UK practice, the British Thoracic Society (BTS) statement provides the most directly applicable clinical guidance. The ISHAM guidelines offer detailed international consensus, particularly for ABPA. Both are complementary and widely used.
- British Thoracic Society (BTS)
Clinical Statement on Aspergillus-related chronic pulmonary disease
UK guidance covering diagnosis and management of ABPA, CPA, and related conditions.
View BTS clinical statement
- International Society for Human and Animal Mycology (ISHAM)
Revised clinical practice guidelines for allergic bronchopulmonary aspergillosis/mycoses
International consensus guidance on diagnosis, classification, and management of ABPA.
View ISHAM guideline (European Respiratory Journal)
- Chronic Pulmonary Aspergillosis (CPA) guidelines
Denning DW et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management
View PubMed record
Further professional resources
For clinician-focused guidance, referral pathways, and educational material:
https://aspergillosis.org/information-for-professionals/
This article is intended for educational purposes and should be interpreted in the context of individual clinical judgement.
Weekly Aspergillosis Research Update (7–11 April 2026)
Last reviewed: April 2026
Audience: Patients, carers, GPs, specialist nurses, and healthcare professionals
Key Points (Summary)
- Invasive pulmonary aspergillosis (IPA) can closely mimic other serious infections, including miliary tuberculosis, particularly in highly immunocompromised patients.
- Metagenomic next-generation sequencing (mNGS) is emerging as a valuable diagnostic tool in complex or unclear cases, though it is not yet widely available.
- Bruton tyrosine kinase (BTK) inhibitors are associated with a measurable risk of invasive fungal infections, with aspergillosis the most frequently reported.
- Host genetics (e.g. toll-like receptor variants) may influence susceptibility to invasive fungal disease, but this is not yet used clinically.
- Azole antifungal drugs remain high-risk for drug–drug interactions, particularly in patients receiving cancer therapies.
- Basic science research continues to identify new fungal targets and pathways, which may inform future treatments.
Contents
- Diagnosis and difficult cases
- Treatment-related risk and immunosuppression
- Genetics and susceptibility
- Asthma and Aspergillus sensitisation
- Drug interactions
- Emerging research and future treatments
- What this means for patients
- When to seek medical advice
Diagnosis and difficult cases
When aspergillosis looks like something else
A case report
(Ji H et al., 2026 – full text)
describes a patient with acute leukaemia who developed widespread “miliary” lung nodules—an imaging pattern classically associated with tuberculosis.
Despite this, the final diagnosis was invasive pulmonary aspergillosis (IPA).
Clinical interpretation
- Radiological appearances in immunocompromised patients can be non-specific.
- Aspergillosis may present without classic features such as halo signs or cavitation.
- Coinfection (e.g. TB + fungal disease) can further complicate interpretation.
This reinforces an important principle in clinical practice: lack of response to treatment should prompt reconsideration of the diagnosis.
The emerging role of mNGS
In this case, metagenomic next-generation sequencing (mNGS) helped establish the diagnosis by detecting fungal DNA directly from clinical samples.
Strengths of mNGS
- Broad pathogen detection (fungi, bacteria, viruses)
- Useful in culture-negative infections
- Can identify unexpected pathogens
Current limitations
- Limited availability outside specialist centres
- Cost and turnaround time
- Interpretation challenges (distinguishing infection from colonisation)
Bottom line: mNGS is promising, but currently complements rather than replaces standard diagnostics (culture, PCR, antigen testing).
Treatment-related risk and immunosuppression
BTK inhibitors and invasive fungal infection
A systematic review and meta-analysis
(PMID: 41954633)
including over 23,000 patients found that:
- Aspergillosis was the most commonly reported invasive fungal infection
- Central nervous system involvement was reported in a subset
Why BTK inhibitors increase risk
- They impair B-cell signalling
- They affect macrophage and neutrophil function
- This reduces the body’s ability to control fungal spores
Clinical implications
- Risk stratification is important
- Some patients may require antifungal prophylaxis
- Early recognition of symptoms is critical
This aligns with increasing recognition that modern targeted therapies can have unintended immunological effects.
Genetics and susceptibility
The role of innate immunity
A systematic review
(PMID: 41962654)
examined toll-like receptor (TLR) polymorphisms and fungal infection risk.
TLRs are part of the innate immune system and are responsible for recognising fungal components such as:
- β-glucans
- Cell wall proteins
Key insight
- Certain genetic variants were more frequently reported in patients with invasive aspergillosis
Important context:
- This does not yet translate into routine testing
- It may become relevant in the future for personalised risk prediction
Asthma and Aspergillus sensitisation
A 12-week prospective study
(PMID: 41949214)
found that:
- ~29% of asthma patients were sensitised to Aspergillus fumigatus
- No significant short-term differences in outcomes were seen compared to non-sensitised patients
Interpretation
- Sensitisation alone does not necessarily indicate active disease
- Clinical context remains critical
Important distinction:
- Sensitisation = immune response to Aspergillus
- ABPA (Allergic Bronchopulmonary Aspergillosis) = a specific inflammatory disease requiring treatment
Drug interactions
Itraconazole and erlotinib interaction
A case report
(PMID: 41953502)
demonstrated increased exposure to erlotinib when co-administered with itraconazole.
Mechanism
- Itraconazole inhibits CYP3A4
- This reduces drug metabolism
- Drug levels rise, increasing risk of toxicity
Clinical message
- Always review medications when starting antifungals
- Particular caution is needed in cancer, transplant, and multi-morbid patients
Useful tool:
Antifungal Interactions Checker
Emerging research and future treatments
Epigenetic regulation in Aspergillus fumigatus
A study
(PMID: 41928566)
identified the role of HosA in regulating fungal growth and virulence.
This type of work helps identify:
- Potential drug targets
- Mechanisms of antifungal resistance
New experimental antifungal compounds
A review
(Full text (PMC))
discusses sodium new houttuyfonate (SNH), which has shown activity in animal models of invasive aspergillosis.
Important caution:
- This is early-stage research
- It is not available as a treatment
What this means for patients
- Aspergillosis can sometimes be difficult to diagnose, especially if symptoms overlap with other conditions.
- If treatment is not working, your medical team may need to review or repeat tests.
- Some medications (especially for cancer or immune conditions) can increase risk of fungal infection.
- Antifungal medications are effective but require careful monitoring for interactions.
- New research is promising, but most advances take time to reach routine care.
When to seek medical advice
Seek medical attention urgently if you have:
- Worsening breathlessness
- Persistent fever
- Coughing up blood
- New chest pain
- Symptoms not improving with treatment
If you are immunocompromised, symptoms may progress quickly and should be assessed promptly.
References
- Ji H et al. Front Fungal Biol, 2026
- Srisurapanont K et al. Blood Adv, 2026
- Pereira Staiger MF et al. Clin Microbiol Infect, 2026
- Yokota H et al. Case Rep Oncol Med, 2026
- Chauhan NK et al. Monaldi Arch Chest Dis, 2026
- Zhou Z et al. Virulence, 2026
- Fang L et al. Front Pharmacol, 2026
Author & Review
This article is part of the Aspergillosis.org weekly research update series. It is intended for general educational purposes and reflects a structured summary of recent research.
Disclaimer: This content is not a substitute for medical advice. Always consult your healthcare team for individual care decisions.