Damp, Mould and Aspergillosis: A Practical Guide for Patients Worried About Their Home
People with aspergillosis, asthma, bronchiectasis, chronic lung disease, allergies, or a weakened immune system are often understandably concerned about whether dampness or mould in the home could be affecting their health.
This guide explains:
- what signs to look for
- what practical steps may help
- the limitations of mould air testing
- who is most likely to provide reliable professional help
- and what support may be available for tenants.
Key points
- Dampness and mould can matter for people with respiratory disease.
- The most important question is usually: why is moisture present?
- Air sampling and mould spore counts have major limitations and should not be relied on alone.
- A “normal” air test does not reliably prove that a home is free from damp or hidden mould.
- The best assessments usually focus on building defects, condensation, ventilation, leaks and moisture sources.
- For complex problems, experienced chartered building professionals and occupational/environmental hygienists are often more useful than simple “mould testing” services.
- Dust and dirt accumulation may contribute to mould growth and respiratory irritation, especially in damp environments.
- Recent UK housing guidance increasingly recognises the health impact of damp and mould.
Why damp and mould matter
Fungi are a normal part of the environment. Tiny fungal spores are present in outdoor air, soil, gardens, compost and many indoor spaces. Most people breathe in small numbers of spores every day without becoming ill.
However, persistent dampness indoors can allow mould growth to increase. This may worsen irritation, allergy, asthma symptoms or respiratory symptoms in some people.
People who may be more sensitive include those with:
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Chronic Pulmonary Aspergillosis (CPA)
- Severe Asthma with Fungal Sensitisation (SAFS)
- bronchiectasis
- Chronic Obstructive Pulmonary Disease (COPD)
- cystic fibrosis
- severe asthma
- significant allergies
- or a weakened immune system.
Signs your home may have a damp problem
Visible signs
- black, green or white mould growth
- condensation on windows
- damp patches
- peeling wallpaper or paint
- bubbling plaster
- staining on walls or ceilings
- warped wood
- persistent condensation
Smell
A persistent musty, earthy or “damp” smell can sometimes indicate hidden moisture or mould growth, even when little is visible.
Possible building causes
- leaks from roofs, gutters or plumbing
- poor ventilation
- condensation
- cold external walls
- thermal bridging
- rising damp
- penetrating damp
- blocked air vents
- drying clothes indoors without enough ventilation.
Can dust and dirt make mould problems worse?
Yes. Accumulated dust and dirt can sometimes contribute to indoor mould problems, especially when combined with moisture or high humidity.
Dust is not simply “dirt” — it often contains:
- skin cells
- textile fibres
- pollen
- bacteria
- fungal spores
- organic material
- and microscopic debris.
When dust accumulates in damp or poorly ventilated areas, it can provide nutrients that allow mould growth to establish more easily on surfaces.
This is particularly common:
- behind furniture placed against cold walls
- around windows
- on curtains and blinds
- inside wardrobes
- under beds
- around ventilation grilles
- and in areas with condensation.
For people with asthma, allergy or aspergillosis, heavy dust accumulation may also worsen irritation or respiratory symptoms independently of visible mould.
Symptoms that may be triggered or worsened
Damp or mould exposure may contribute to:
- coughing
- wheezing
- chest tightness
- breathlessness
- increased sputum
- nasal irritation
- sinus symptoms
- eye irritation
- fatigue
- worsening asthma control
- increased allergy symptoms.
Symptoms may be more noticeable in certain rooms, overnight, during winter, after rainfall, or when ventilation is poor.
However, symptoms alone cannot prove that mould exposure is the cause. Many respiratory conditions can cause similar symptoms, so medical advice is important if symptoms are worsening.
Should you get air testing done?
Many companies offer indoor air sampling, mould spore counts or fungal testing. Patients often hope this will provide reassurance or proof that a home is safe.
Unfortunately, air sampling has important limitations.
Limitations of air sampling
- There are no universally agreed “safe” mould spore levels for homes.
- Results can vary enormously throughout the day.
- Outdoor air can strongly influence indoor results.
- Cleaning, vacuuming, opening windows or walking around can alter results.
- A short air sample may not represent usual exposure.
- Hidden damp or mould may not show up in an air sample.
- A “normal” air test does not reliably prove that a building is free from damp or mould problems.
Air sampling may sometimes be useful when carried out by experienced specialists as part of a wider investigation. However, it should not be used as the only basis for deciding whether a home is safe or whether remediation has worked.
What usually matters most?
The key question is usually:
Why is moisture present in the home?
Without moisture, significant mould growth usually cannot continue. Therefore, the most important step is to identify and correct the source of dampness.
This may involve:
- repairing leaks
- improving ventilation
- reducing condensation
- correcting insulation or thermal bridging problems
- repairing gutters, roofs or plumbing
- addressing overcrowding or excessive indoor humidity.
What you can do yourself
Improve ventilation
- Use extractor fans in bathrooms and kitchens.
- Open windows when practical and safe.
- Do not block air vents.
- Ventilate after showering, cooking or drying clothes.
Reduce indoor humidity
- Dry clothes outdoors where possible.
- Use lids on pans while cooking.
- Avoid drying clothes on radiators without ventilation.
- Consider a humidity monitor.
- Aim to avoid persistently high indoor humidity.
A dehumidifier may help reduce humidity in some situations, but it does not fix the underlying cause of dampness if there is a leak, structural defect or ventilation problem.
Reduce dust accumulation
- Clean regularly using methods that minimise dust disturbance.
- Pay particular attention to hidden or poorly ventilated areas.
- Move furniture slightly away from cold external walls where possible.
- Reduce clutter that traps dust and moisture.
- Wash soft furnishings and curtains regularly if practical.
Clean small areas carefully
Small areas of surface mould can sometimes be cleaned carefully using appropriate cleaning products. Avoid dry brushing or actions that disturb mould and release spores into the air.
People with significant lung disease, severe asthma, severe allergy or aspergillosis may prefer somebody else to carry out cleaning to reduce exposure.
Large, recurring or hidden mould problems usually need professional assessment.
Who is most likely to provide reliable help?
The most useful professionals are usually those who investigate the building and the source of moisture, not just the air.
For complex damp or mould problems, more robust help may come from:
- experienced chartered building surveyors
- building pathology specialists
- chartered building engineers
- occupational hygienists
- environmental hygienists with experience in indoor air quality and moisture assessment.
Relevant UK professional bodies
- Royal Institution of Chartered Surveyors (RICS)
- Chartered Institute of Building (CIOB)
- Chartered Association of Building Engineers (CABE)
- British Occupational Hygiene Society (BOHS)
Some damp and remediation companies may also be associated with the Property Care Association (PCA). This may indicate relevant industry training, but membership alone does not guarantee expertise. Experience and independence still matter.
Is impartial advice available?
Sometimes. People are often unsure where to obtain trustworthy, independent advice about damp and mould.
Possible sources of impartial guidance may include:
- local council Environmental Health departments
- housing officers (for tenants)
- Citizens Advice services
- NHS guidance
- UK Health Security Agency (UKHSA) guidance
- recognised professional bodies.
Local councils may sometimes inspect severe housing conditions, particularly where:
- children or vulnerable adults are involved
- landlords are failing to act
- there is extensive visible mould
- or housing conditions may present health hazards.
Support varies considerably between areas, and services are often stretched, but councils can sometimes require landlords to take action where housing conditions are unsafe.
Awaab’s Law and what it may mean for tenants
For people living in rented accommodation, especially social housing, recent changes in UK housing law may provide stronger protection where damp and mould problems are affecting health.
Awaab’s Law was introduced following the death of two-year-old Awaab Ishak in Rochdale after prolonged exposure to severe mould in social housing.
The law strengthens expectations that social landlords:
- investigate damp and mould complaints promptly
- assess potential risks to health
- carry out repairs within defined timescales
- and respond more urgently where vulnerable people are involved.
This is particularly important for people with:
- aspergillosis
- asthma
- bronchiectasis
- Chronic Obstructive Pulmonary Disease (COPD)
- cystic fibrosis
- or weakened immune systems.
What tenants should do
If you are concerned about damp or mould in rented accommodation, it may help to:
- report problems formally and in writing where possible
- keep photographs and dates
- record repeated complaints
- document worsening conditions
- keep copies of correspondence
- retain relevant medical letters if symptoms are worsening.
Where severe respiratory disease is present, medical evidence may help demonstrate vulnerability and the need for urgent action.
Important limitations
Awaab’s Law does not mean that every mould problem becomes an emergency or that all homes can be repaired immediately. Housing shortages, structural problems, funding limitations and contractor delays still affect what can be achieved.
However, the law has strengthened the expectation that damp and mould complaints should be taken seriously and addressed promptly, particularly where vulnerable people are affected.
NICE guidance and UK guidance
The National Institute for Health and Care Excellence (NICE) has increasingly recognised the importance of indoor air quality and housing conditions in respiratory health.
In addition, the UK Health Security Agency (UKHSA) has published major guidance emphasising that:
- damp and mould should be addressed promptly
- visible mould should not be ignored
- people with respiratory disease may be more vulnerable
- and simply blaming lifestyle alone is often inappropriate.
Recent UK guidance has increasingly shifted away from treating damp and mould purely as cosmetic issues, recognising their potential health impacts — especially for vulnerable people.
Questions to ask before paying for an assessment
- What qualifications and experience do you have in damp, mould and building moisture problems?
- Are you independent, or do you also sell remediation work?
- Will you investigate moisture sources, ventilation and building defects?
- Will I receive a written report explaining the likely cause?
- How will you decide whether remediation has worked?
- Will you explain the limitations of any air sampling?
- Do you use air sampling as part of a wider assessment, or as the main test?
Be cautious if...
- the assessment mainly consists of a quick air sample
- dramatic health claims are made
- the report presents spore counts as a simple “safe/unsafe” result
- expensive remediation is recommended immediately
- the company creates pressure to buy treatment packages
- there is little attention to leaks, condensation, ventilation or building defects.
How do you know remediation has worked?
Success should usually be judged by practical outcomes, including:
- visible mould has been removed safely
- the source of moisture has been corrected
- damp patches are drying out
- musty smells have reduced
- ventilation has improved
- humidity is better controlled
- mould does not quickly return
- symptoms improve over time, where mould exposure was contributing.
Repeat air sampling alone is not a reliable way to prove that a home is safe.
When to seek medical advice
People with aspergillosis or other lung conditions should seek medical advice if they experience:
- worsening breathlessness
- coughing blood
- rapidly worsening asthma symptoms
- fever or signs of infection
- unexplained weight loss
- significant deterioration in chest symptoms
- new or worsening fatigue with chest symptoms.
If symptoms appear linked to a damp or mouldy environment, discuss this with your healthcare team. They may not be able to assess the building, but they can help assess your health and whether your respiratory condition is changing.

Related information on Aspergillosis.org
- Reducing mould exposure
- Damp homes and health study
- What is aspergillosis?
- Living with aspergillosis
- Patient information hub
Useful resources
- UK Health Security Agency: Damp and mould guidance
- NICE: Indoor air quality at home
- NICE: Excess winter deaths and illness and the health risks associated with cold homes
- UK Government: Awaab’s Law factsheet
- Shelter UK: Damp and mould in rented homes
- Citizens Advice: Housing disrepair
Sir David Attenborough at 100: Inspiring Wonder in Nature and Fungi
Celebrating 100 years of Sir David Attenborough and his extraordinary contribution to understanding nature, fungi and the living world.Today marks the 100th birthday of David Attenborough — a remarkable milestone for someone who has spent a lifetime helping the world see nature differently.
For many of us interested in fungi and aspergillosis, his work has also helped shine a light on a kingdom of life that was too often overlooked. Through documentaries exploring fungi, moulds, forests and hidden ecosystems, he helped bring the extraordinary world of fungi into homes around the globe — revealing not just beauty, but the vital role fungi play in life on Earth.
At a time when awareness of fungal disease and environmental mould exposure remains so important, that contribution matters greatly.
Happy 100th Birthday Sir David — and thank you for a century of curiosity, education and wonder.

Blue inhalers, combination inhalers and aspergillosis: what patients need to know
Blue reliever inhalers, such as salbutamol or Ventolin, remain important medicines and can be lifesaving during asthma symptoms or an asthma attack. However, asthma guidelines have changed because doctors now recognise that relying too heavily on a blue inhaler can be a sign that the underlying airway inflammation is not being well controlled.
What is a blue inhaler?
A blue inhaler usually contains a medicine called a short-acting beta2 agonist, often shortened to SABA. Salbutamol is the best-known example.
These inhalers work quickly by relaxing the muscles around the airways. This can relieve wheeze, chest tightness and breathlessness within minutes. However, a blue inhaler does not treat the airway inflammation that often drives asthma symptoms.
You can read more about reliever inhalers from Asthma + Lung UK.
Why are asthma guidelines changing?
Asthma is not just a condition of narrowed airways. It is also an inflammatory condition. A reliever inhaler may make breathing feel easier for a short time, but if inflammation is not treated, asthma may remain poorly controlled.
Frequent use of a blue reliever inhaler can therefore be a warning sign. It may mean that asthma treatment needs reviewing, especially if someone is needing their reliever often, waking at night, having flare-ups, or finding their normal activities limited.
The updated NICE/BTS/SIGN asthma guideline supports greater use of treatment plans that combine symptom relief with anti-inflammatory treatment.
What are AIR and MART inhalers?
Some patients are now prescribed a combination inhaler that contains:
- a fast-acting reliever medicine to open the airways
- an inhaled corticosteroid to reduce inflammation
These approaches are known as:
- AIR – Anti-Inflammatory Reliever
- MART – Maintenance and Reliever Therapy
With these plans, the combination inhaler may be used when symptoms occur. In MART, it is also used regularly every day as maintenance treatment.
The important difference is that when symptoms increase, the patient receives more anti-inflammatory treatment as well as more reliever medicine. This aims to reduce the cycle of worsening symptoms, repeated blue inhaler use, and untreated inflammation.
Useful patient information is available from Asthma + Lung UK on AIR inhalers and MART inhalers.
Does this mean everyone should stop using their blue inhaler?
No. This is the most important point.
The new guidance does not mean that every patient must immediately stop using a blue inhaler. It also does not mean that blue inhalers are “bad” or banned.
For many people, nothing will change straight away. Some patients will remain on their current inhalers. Others may be changed to an AIR or MART plan after review by their GP, asthma nurse or respiratory specialist.
Will some patients have their blue inhaler taken away?
Sometimes, but not always.
If a patient is moved onto an AIR or MART plan, their combination inhaler may become both their preventer and their reliever. In that situation, they may no longer routinely need a separate blue inhaler.
However, some patients may still keep a blue inhaler as backup, and others may continue with separate preventer and reliever inhalers. This depends on the individual patient, their diagnosis, their inhalers, and their asthma action plan.
Not all combination inhalers can be used as relievers. Only specific inhalers containing a fast-acting medicine such as formoterol are suitable for AIR or MART use. Patients should only use inhalers in this way if they have been specifically prescribed and instructed to do so.
Why this is more complicated for aspergillosis patients
People with aspergillosis-related lung disease often have more complex respiratory problems than standard asthma alone.
This may include:
- ABPA (Allergic Bronchopulmonary Aspergillosis)
- severe asthma with fungal sensitisation
- bronchiectasis
- mucus plugging
- chronic airway infection or fungal colonisation
- reduced lung reserve or scarring
For these patients, breathlessness is not always caused by asthma-type inflammation alone. It may also be related to mucus, infection, bronchiectasis, fungal activity, or structural lung damage.
This means that simply taking more inhaler may not always address the real cause of worsening symptoms.
Steroids: useful but needing balance
Inhaled corticosteroids can be very helpful in asthma and ABPA because they reduce airway inflammation. Good control of inflammation may reduce symptoms, flare-ups and the need for oral steroid courses.
However, steroid exposure also needs careful management in aspergillosis patients. Higher steroid doses may increase the risk of side effects such as oral thrush and, in some situations, may affect the balance between inflammation control and fungal growth.
This does not mean patients should avoid inhaled steroids. It means that treatment should be individualised and reviewed by a clinician who understands the patient’s full lung condition.
What should aspergillosis patients do?
- Do not stop your blue inhaler suddenly if it has been prescribed for you.
- Do not change your preventer or steroid inhaler without medical advice.
- Check your own asthma action plan. Make sure you know which inhaler is for daily prevention and which one is for symptoms.
- Ask whether your combination inhaler is suitable for AIR or MART use. Do not assume that all combination inhalers can be used this way.
- Request a review if you are using your reliever inhaler frequently, symptoms are worsening, or you are unsure what to do.
When to seek urgent help
Seek urgent medical help if your breathlessness is severe, your reliever is not helping as expected, you are struggling to speak in full sentences, your lips or fingers look blue, or your symptoms are rapidly worsening.
Follow your personal asthma action plan. If you think you are having an asthma attack, do not delay seeking emergency help.
The key message
The new guidance is not simply about “taking away blue inhalers”. It is about recognising that asthma symptoms often reflect airway inflammation, and that some patients do better when symptom relief and anti-inflammatory treatment are given together.
For people with aspergillosis, the message is especially important: inhaler treatment should be reviewed in the context of the whole lung condition, not changed because of a headline.
If you are unsure about your inhalers, speak to your GP, asthma nurse, respiratory consultant or aspergillosis team.
Further reading
Dry Mouth, Aspergillosis and Dental Health
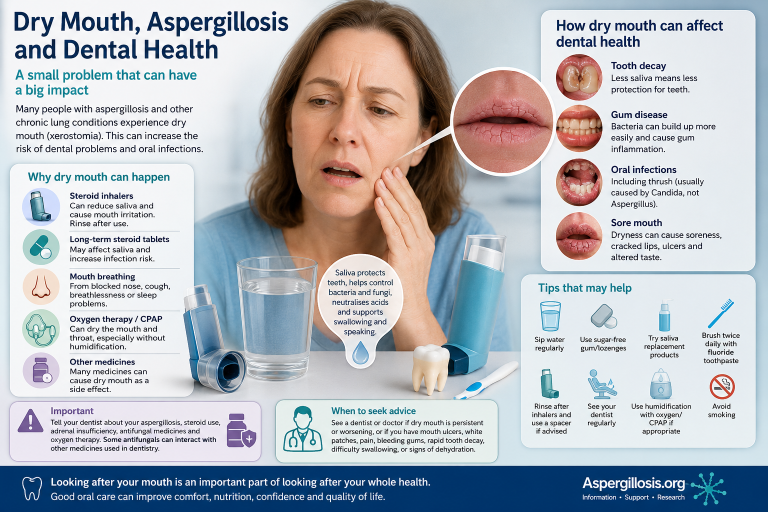
Why oral health problems may be more common than many patients expect
People living with aspergillosis often focus understandably on symptoms such as breathlessness, coughing, fatigue, wheezing or chest infections. However, many patients also notice problems affecting the mouth, throat and teeth — particularly dry mouth, soreness, altered taste and worsening dental health.
Although Aspergillus itself does not usually directly infect the mouth, the wider effects of chronic respiratory disease, medications and long-term treatment can sometimes have a significant impact on oral health and wellbeing.
Key points
- Dry mouth is commonly reported by patients with chronic respiratory disease and aspergillosis.
- Saliva is important for protecting teeth and gums.
- Steroid inhalers, mouth breathing and oxygen therapy can all contribute to dryness.
- Long-term dry mouth may increase the risk of tooth decay, gum disease and oral infections.
- Good oral hygiene and regular dental care are especially important.
- Dentists should be informed about antifungal medications and steroid treatment.
Why does dry mouth happen?
Dry mouth, sometimes called xerostomia, occurs when the mouth does not produce enough saliva or when saliva does not protect the mouth as effectively as usual.
Saliva plays several important roles. It helps protect teeth from decay, controls bacteria and fungi, reduces acidity in the mouth, supports swallowing and speech, and protects the delicate tissues inside the mouth.
When saliva levels fall, patients may notice:
- a sticky or dry feeling in the mouth;
- waking with a dry mouth;
- difficulty swallowing dry foods;
- sore gums, tongue or throat;
- bad breath;
- cracked lips;
- increased thirst;
- altered taste;
- mouth soreness or burning.
Why might aspergillosis patients be affected?
In many cases, the problem is not caused directly by Aspergillus itself. Instead, several factors linked to respiratory disease and treatment may combine together.
Steroid inhalers
Inhaled corticosteroids are commonly used in asthma, Allergic Bronchopulmonary Aspergillosis (ABPA), severe eosinophilic lung disease and other respiratory conditions.
These medicines are important and should not be stopped without medical advice, but they can sometimes contribute to mouth irritation, dryness, hoarseness, oral thrush and throat discomfort.
Using a spacer device, where appropriate, and rinsing the mouth after inhaler use may help reduce some local side effects.
Long-term steroid tablets
Some patients with aspergillosis or severe asthma have taken oral steroid tablets such as prednisolone, sometimes for prolonged periods. Long-term steroid exposure may affect immunity and can increase the risk of infections such as oral thrush.
Some patients may also develop adrenal suppression or adrenal insufficiency after prolonged steroid exposure. Patients with known adrenal insufficiency should make sure their dentist and healthcare team are aware before significant dental treatment or procedures.
Mouth breathing
Many people with chronic respiratory disease breathe through their mouth more often, especially overnight. This may happen because of blocked nose, sinus disease, breathlessness, coughing, asthma symptoms or poor sleep.
Over time, regular mouth breathing can dry the mouth and throat, especially during the night.
Oxygen therapy and CPAP
Supplemental oxygen and continuous positive airway pressure (CPAP) devices may dry the upper airways, particularly if humidification is not used.
Some patients notice dry lips, sore throat, dry nose, thick mucus or increased mouth discomfort overnight.
Medication side effects
A number of commonly prescribed medicines may contribute to dry mouth. These can include antihistamines, antidepressants, some pain medicines, bronchodilators and some blood pressure medicines.
The combined effect of several medicines may become significant, especially in people managing complex long-term health conditions.
Why does dry mouth matter for dental health?
Dry mouth is more than simply uncomfortable. Saliva normally helps protect the teeth and gums. Without enough saliva, plaque bacteria can grow more easily, acids remain in contact with teeth for longer, enamel may weaken and gums may become inflamed.
Some patients are surprised by how quickly dental problems can develop after periods of illness, long-term treatment or persistent dry mouth.
Possible problems include:
- tooth decay;
- gum disease;
- sensitive teeth;
- mouth ulcers;
- oral thrush;
- cracked lips;
- denture discomfort;
- difficulty eating or speaking comfortably.
Oral thrush and fungal infections
Patients with aspergillosis sometimes worry that oral fungal infections mean Aspergillus is spreading in the mouth. In most cases, oral thrush is caused by Candida yeast rather than Aspergillus.
Symptoms of oral thrush may include white patches, soreness, redness, altered taste, painful swallowing or cracking at the corners of the mouth.
Steroid inhalers and dry mouth can both increase the risk of thrush. Patients should seek medical or dental advice if symptoms persist or recur.
Important information for dentists
Patients should inform their dentist about:
- their aspergillosis diagnosis;
- inhaled or oral steroid use;
- adrenal insufficiency or adrenal suppression;
- antifungal medicines;
- oxygen therapy or CPAP use;
- significant breathlessness or difficulty lying flat.
This is important because some antifungal medicines, including itraconazole, voriconazole and posaconazole, can interact with other medicines. Dentists and doctors can help check for possible interactions when procedures, antibiotics, pain relief or sedation are being considered.
Practical tips that may help
Some patients find the following measures helpful:
- sip water regularly;
- avoid excessive alcohol and caffeine;
- use sugar-free gum or lozenges if suitable;
- ask a pharmacist or dentist about saliva replacement sprays, gels or mouthwashes;
- rinse the mouth after steroid inhalers;
- use a spacer device if recommended;
- brush twice daily with fluoride toothpaste;
- clean between teeth if able;
- attend regular dental reviews;
- avoid smoking;
- discuss persistent symptoms with a GP, dentist, pharmacist or specialist team.
Patients using oxygen or CPAP may wish to ask their respiratory team whether humidification is appropriate.
When to seek medical or dental advice
Seek advice if dry mouth is persistent, worsening or causing problems with eating, sleeping, swallowing or speaking.
Medical or dental review is particularly important if there are mouth ulcers, white patches, bleeding gums, rapid tooth decay, severe soreness, repeated oral thrush, signs of dehydration, dizziness or marked weakness.
Patients with adrenal insufficiency, severe respiratory disease or complex medication regimens should make sure healthcare professionals are aware before major dental procedures.
A commonly overlooked part of chronic illness
Living with aspergillosis often involves managing far more than lung symptoms alone. Dry mouth and dental health problems may seem minor at first, but over time they can affect comfort, nutrition, sleep, confidence, communication and overall quality of life.
Recognising these issues early may help patients seek support sooner and reduce longer-term complications.
Further information
Author and review information
Prepared by: National Aspergillosis Centre CARES Team / Aspergillosis Website Editorial Team
Last reviewed: May 2026
References and further reading
- NHS information on dry mouth and oral thrush.
- Dental and oral medicine guidance on xerostomia and prevention of tooth decay.
- Respiratory guidance on inhaled corticosteroids and inhaler technique.
- Medicines information for azole antifungals and corticosteroids.
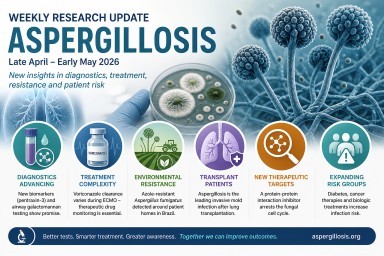
Weekly Aspergillosis Research Update April - May 2026
Search term: aspergillosis
Period covered: late April–early May 2026
Key highlights this week
- Diagnostics: new evidence for pentraxin-3 and airway galactomannan testing.
- Treatment: voriconazole dosing may be difficult during ECMO and needs close monitoring.
- Resistance: azole-resistant Aspergillus fumigatus detected around patient homes in Brazil.
- Transplant medicine: aspergillosis remains the dominant invasive mould infection after lung transplantation.
- Future therapies: early laboratory work identifies a possible new antifungal drug target.
1. New diagnostic marker: pentraxin-3 for invasive pulmonary aspergillosis
Sun C et al. Diagnostic value of pentraxin 3 in plasma and bronchoalveolar lavage fluid for invasive pulmonary aspergillosis in non-neutropenic patients: a prospective multicenter clinical study. Emerging Microbes & Infections, 2026.
View on PubMed – PMID: 42054395
This prospective multicentre study looked at pentraxin-3 in blood and bronchoalveolar lavage fluid as a diagnostic marker for invasive pulmonary aspergillosis in patients who are not neutropenic.
Why it matters: diagnosing invasive aspergillosis can be especially difficult in patients outside the classic high-risk groups. This study supports the wider move toward combining tests and biomarkers rather than relying on one result alone.
2. Galactomannan testing in tracheobronchial aspirates after lung transplant
Monforte A et al. Diagnostic value of galactomannan in tracheobronchial aspirate for Aspergillus infection in lung transplant recipients (the GALACTBAS study). Journal of Clinical Microbiology, 2026.
View on PubMed – PMID: 42059612
This study assessed whether galactomannan testing in tracheobronchial aspirates can help diagnose Aspergillus infection in lung transplant recipients.
Why it matters: aspergillosis after lung transplantation often involves the airways. Testing airway samples may support earlier diagnosis and may sometimes be less invasive than deeper lung sampling.
3. Voriconazole levels may vary during ECMO
Yusuff H et al. Time-varying voriconazole clearance during extracorporeal membrane oxygenation. Antimicrobial Agents and Chemotherapy, 2026.
View on PubMed – PMID: 42059809
This paper looked at voriconazole clearance in critically ill patients receiving extracorporeal membrane oxygenation (ECMO).
Why it matters: voriconazole is commonly used to treat invasive aspergillosis, but drug levels can be unpredictable in critical illness. This supports the importance of therapeutic drug monitoring so dosing can be adjusted safely and effectively.
4. Azole-resistant Aspergillus found around patient homes in Brazil
de Barros Rodrigues DK et al. Environmental circulation of Aspergillus fumigatus with reduced susceptibility to agricultural triazole in Brazil: clonal dissemination of potentially resistant genotypes. Mycoses, 2026.
View on PubMed – PMID: 42037564
This study investigated environmental Aspergillus fumigatus around the homes of two patients with suspected aspergillosis caused by resistant isolates.
Why it matters: the findings add to concern that antifungal resistance can arise and circulate in the environment, including through exposure to agricultural triazoles. This is important because azole resistance can make aspergillosis harder to treat.
5. Invasive mould infections after lung transplantation: aspergillosis dominates
Pennington KM et al. Impact of invasive mold infection-coded diagnoses on utilization, costs, and mortality after lung transplantation. Chest, 2026.
View on PubMed – PMID: 42061698
This study assessed invasive mould infection-coded diagnoses after lung transplantation. Aspergillosis was the most common invasive mould infection reported.
Why it matters: lung transplant recipients remain among the highest-risk groups for severe aspergillosis. The study reinforces the need for prevention, early recognition, rapid diagnosis and specialist management.
6. A possible new antifungal target in Aspergillus fumigatus
Storer ISR et al. A protein-protein interaction inhibitor arrests the cell cycle in Aspergillus fumigatus. mBio, 2026.
View on PubMed – PMID: 42053292
This laboratory study explored a compound that interferes with protein-protein interactions and can arrest the cell cycle in Aspergillus fumigatus.
Why it matters: current antifungal options remain limited, and resistance is a growing problem. Early-stage work like this may help identify future antifungal drug classes.
7. Diabetes and fungal infection risk
Kaur H et al. Fungal infections in diabetes mellitus. Indian Journal of Medical Microbiology, 2026.
View on PubMed – PMID: 42061613
This review discusses fungal infections in people with diabetes, including mucormycosis, aspergillosis and cryptococcosis.
Why it matters: diabetes can affect immune function and increase susceptibility to some infections. For patients with existing lung disease, good diabetes management may be one part of reducing overall infection risk.
8. Aspergillosis during cancer immunotherapy
Niravath P et al. A Phase II Study of Docetaxel and Pembrolizumab plus Interleukin 12 Gene Therapy in Nonmetastatic, Anthracycline-Refractory Triple-Negative Breast Cancer (INTEGRAL). Clinical Cancer Research, 2026.
View on PubMed – PMID: 41661218
This cancer therapy study includes a reported case of pulmonary aspergillosis and respiratory failure during treatment.
Why it matters: modern cancer treatments can alter infection risk in complex ways. Aspergillosis should remain on the radar in patients who become unwell during or after intensive cancer therapy.
Other papers noted this week
- Canakinumab safety pharmacovigilance analysis – relevant to biologic therapy safety and infection monitoring. PMID: 41998856
- Canine sinonasal radiotherapy study – includes nasal aspergillosis in dogs, but is mainly veterinary/radiotherapy focused. PMID: 42007656
- Mucormycosis retrospective study – relevant to invasive fungal disease burden but not directly focused on aspergillosis. PMID: 42050055
Overall message
This week’s papers show how aspergillosis research is moving in several important directions at once: better diagnostic markers, more personalised antifungal dosing, growing concern about environmental resistance, and continued recognition of high-risk groups such as transplant recipients, critically ill patients and people with complex immune or metabolic conditions.
For patients, the main message is that aspergillosis is a complex condition and testing or treatment decisions often need specialist interpretation. No single test result tells the whole story; clinicians usually combine symptoms, scans, culture results, biomarkers and risk factors before deciding on diagnosis and treatment.
Reducing Exposure to Mould (Aspergillus) at Home
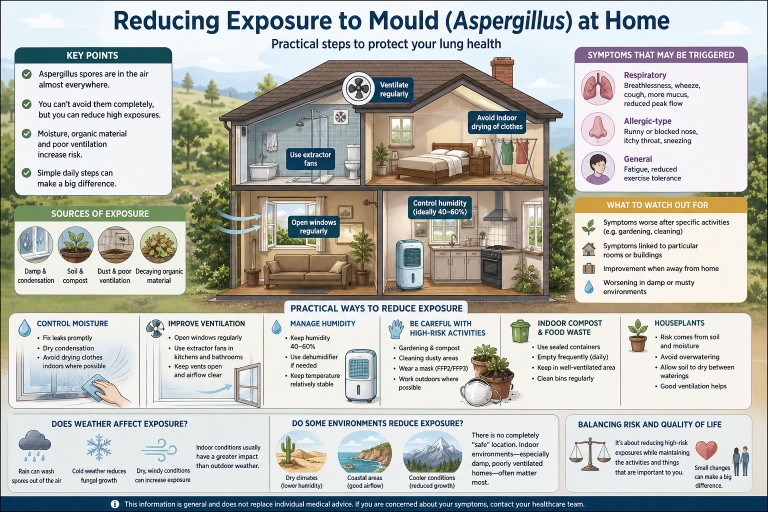
Audience: Patients with aspergillosis (including Allergic Bronchopulmonary Aspergillosis and Chronic Pulmonary Aspergillosis), carers, and non-specialist cliniciansIf you have aspergillosis, reducing exposure to environmental moulds such as Aspergillus can help minimise symptoms and reduce the risk of flare-ups.This guide brings together practical, evidence-informed advice based on environmental studies and clinical experience at specialist centres such as the National Aspergillosis Centre (Manchester, UK).
🔑 Key Points
- Aspergillus spores are present in the air almost everywhere.
- Complete avoidance is not possible—focus on reducing higher-level exposures.
- The most important drivers are moisture, organic decay, and disturbance.
- Indoor exposure is often more important than outdoor exposure.
- Simple environmental and behavioural changes can significantly reduce risk.
🌍 Where does mould exposure come from?
Aspergillus is a common environmental mould. It grows on organic material and releases microscopic spores into the air.
Common sources include:
- Damp walls, ceilings, and condensation
- Soil, compost, and plant material
- Dust and poorly ventilated spaces
- Food waste and decaying organic matter
Spores are always present at low levels. Problems arise when concentrations increase, particularly in enclosed or damp environments.
⚖️ Who is most affected?
Reducing exposure is particularly relevant for people with:
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Chronic Pulmonary Aspergillosis (CPA)
- Asthma or bronchiectasis
- Reduced immune function
Individual sensitivity varies. Some people notice clear environmental triggers, while others are less affected by day-to-day variation.
⚠️ What symptoms can mould exposure trigger?
Exposure may trigger or worsen symptoms by increasing airway inflammation or allergic responses.
Respiratory symptoms
- Increased breathlessness
- Wheezing or chest tightness
- Persistent or worsening cough
- Increased or thicker mucus
- Reduced peak flow (if monitored)
Allergic-type symptoms
- Nasal congestion or runny nose
- Itchy throat
- Sneezing
General symptoms
- Fatigue
- Reduced exercise tolerance
In ABPA, exposure may contribute to flare-ups. In CPA, changes may be more gradual.
👀 What should you watch out for?
Patterns are often more informative than single exposures.
- Symptoms worsening after specific activities (e.g. gardening, cleaning)
- Symptoms linked to particular rooms or buildings
- Improvement when away from home
- Worsening in damp or musty environments
Keeping a simple symptom diary can sometimes help identify triggers.
Important: Not all symptoms are due to mould exposure—other factors such as infection or asthma control may also play a role.
🏠 Reducing mould in your home
1. Control moisture (most important factor)
- Fix leaks promptly (pipes, roofs, windows)
- Dry condensation from windows and walls
- Avoid prolonged indoor drying of clothes where possible
Moisture is the key driver of mould growth—reducing it addresses the root cause.
2. Improve ventilation
- Open windows regularly (even short periods can help)
- Use extractor fans in kitchens and bathrooms
- Avoid blocking vents or airflow pathways
Ventilation removes spores and reduces humidity at the same time.
3. Manage condensation
- Maintain a relatively stable indoor temperature
- Use lids when cooking
- Consider dehumidifiers in problem areas
🌬️ Ventilation, filtration and humidity
Ventilation (first priority)
Ventilation is usually the most effective intervention because it removes airborne spores and reduces moisture.
Dehumidifiers
Dehumidifiers reduce indoor humidity (target around 40–60%), making conditions less favourable for mould growth.
HEPA air purifiers
HEPA filters can remove airborne particles, including fungal spores. However, they do not address the source of mould and are best used alongside other measures.
Practical approach: address moisture and ventilation first, then consider additional filtration if needed.
🌦️ Does weather affect mould exposure?
- Rain can reduce airborne spores by washing them out of the air
- Cold conditions reduce fungal growth
- Dry, windy weather can increase exposure by disturbing dust and soil
However, indoor conditions usually have a greater impact than outdoor weather.
🌍 Do some environments reduce exposure?
Some environments may be associated with lower exposure:
- Dry climates (lower humidity)
- Coastal areas (good airflow and dilution)
- Cooler conditions (reduced fungal growth)
There is no completely “safe” location, and indoor conditions often matter more than geography.
🌿 Activities and exposure
Some activities can temporarily increase exposure:
- Gardening or handling compost
- Cleaning dusty areas
- Handling stored materials
Precautions:
- Wear a well-fitted mask (FFP2 or FFP3)
- Carry out dusty tasks outdoors where possible
- Avoid enclosed, poorly ventilated spaces
🗑️ Indoor compost bins and food waste
Food waste provides an ideal environment for mould growth.
Risk increases when waste is stored indoors for prolonged periods, particularly in warm conditions.
- Empty bins frequently (ideally daily)
- Use sealed containers
- Keep in well-ventilated areas
- Clean bins regularly
🌱 Houseplants
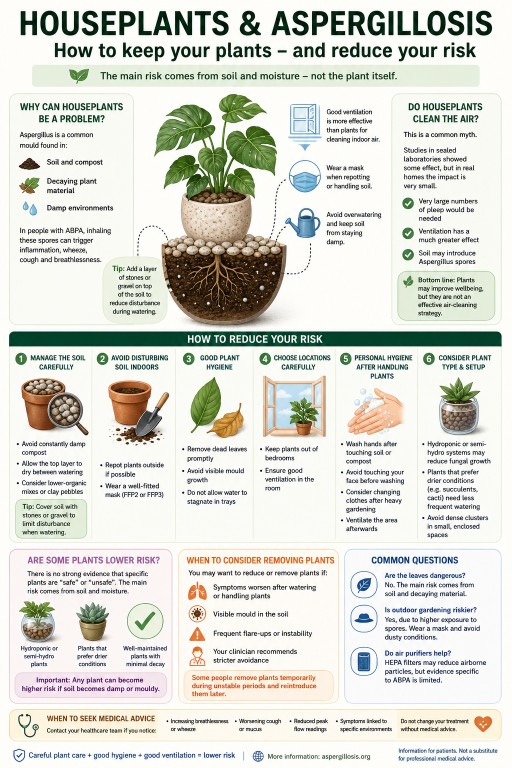
The main risk comes from soil and moisture rather than the plant itself.
👉 Read full guide on houseplants and aspergillosis
⚖️ Balancing risk and quality of life
It is important to balance exposure reduction with maintaining normal daily activities.
- Gardening can often continue with precautions
- Houseplants can often be kept safely
- Focus on reducing higher-risk exposures rather than avoiding everything
⚠️ When to seek medical advice
- Increasing breathlessness
- Worsening cough or mucus
- Reduced peak flow
- Symptoms clearly linked to environment
Seek urgent advice for:
- Rapid breathlessness
- Chest pain
- Coughing blood
📚 Further reading
👩⚕️ Author & Review
Developed using patient questions and reviewed in line with National Aspergillosis Centre practice (Manchester, UK).
This information is general and does not replace individual medical advice.

Houseplants and Aspergillosis: Do You Need to Get Rid of Them?
Audience: Patients with aspergillosis (including Allergic Bronchopulmonary Aspergillosis), carers, and non-specialist cliniciansHouseplants are a common concern for people with
aspergillosis, particularly those with
Allergic Bronchopulmonary Aspergillosis (ABPA).If you’ve asked this question, you’re not alone—many patients raise it in our
patient questions and discussions.
🔑 Key Points
- Houseplants can be a source of Aspergillus spores, mainly from soil.
- Most people with ABPA do not need to remove all plants.
- The main risk comes from damp soil and disturbance.
- Simple precautions can significantly reduce exposure.
- How plants are cared for matters more than the type of plant.
Contents
- Why houseplants can be a problem
- How big is the risk?
- Do houseplants clean the air?
- Can I safely keep my plants?
- How to reduce risk
- Are some plants lower risk?
- When to consider removing plants
- Common questions
- When to seek medical advice
- References
🌱 Why can houseplants be a problem?
Aspergillus is a common environmental mould found in:
- Soil and compost
- Decaying plant material
- Damp indoor environments
For people with Allergic Bronchopulmonary Aspergillosis (ABPA), inhaling spores can trigger airway inflammation, wheeze, cough, and breathlessness.
The main risk comes from soil rather than the plant itself.
⚖️ How big is the risk?
The risk varies depending on:
- How stable your condition is
- The number of plants
- Ventilation in your home
- How plants are maintained
Specialist centres such as the National Aspergillosis Centre (NAC) recommend a
risk reduction approach rather than complete avoidance.
You can read more in our guide to
reducing mould exposure.
Important: There is limited direct research linking houseplants to worsening ABPA. Advice is based on environmental studies and clinical experience.
🌿 Do houseplants clean the air?
You may have heard that houseplants “clean the air.” This idea comes from laboratory studies, including research by
:contentReference[oaicite:0]{index=0}, conducted in sealed environments.
In real homes, the effect is minimal.
- Very large numbers of plants would be needed
- Ventilation has a much greater impact
- Soil may introduce Aspergillus spores
For a broader explanation, see our
aspergillosis overview.
Bottom line: Plants may improve wellbeing, but they are not an effective air-cleaning strategy.
🌿 Can I safely keep my houseplants?
In many cases, yes.
Many people with ABPA keep houseplants without problems when their condition is stable and plants are well maintained.
However, some individuals are more sensitive, so a personalised approach is important.
✅ How to reduce your risk
1. Manage the soil carefully
- Avoid constantly damp compost
- Allow the top layer to dry between watering
- Consider lower-organic substrates (e.g. clay pebbles)
Tip from patients: Adding a layer of stones or gravel on top of the soil can reduce disturbance during watering and may help limit release of fungal spores.
2. Avoid disturbing soil indoors
- Repot plants outside if possible
- Wear a well-fitted mask (FFP2 or FFP3)
3. Maintain good plant hygiene
- Remove dead leaves promptly
- Avoid visible mould growth
- Do not allow stagnant water
4. Choose locations carefully
- Keep plants out of bedrooms
- Ensure good ventilation
5. Personal hygiene after handling plants
- Wash hands after handling soil or compost
- Avoid touching your face before cleaning hands
- Consider changing clothes after heavy gardening
- Ventilate the area after indoor plant work
These steps form part of a wider approach to
reducing environmental exposure.
🌿 Are some plants lower risk for ABPA?
There is no strong evidence that specific plants are “safe” or “unsafe.” The main risk comes from soil and moisture.
Some setups may be lower risk in practice:
- Hydroponic or semi-hydroponic plants
- Plants that prefer drier conditions (e.g. succulents)
- Well-maintained plants with minimal decaying material
Important: Any plant can become higher risk if soil becomes damp or mouldy.
If unsure, you may wish to review
clinical guidance or discuss with your care team.
🚩 When should I consider removing plants?
- Symptoms worsen after watering or handling plants
- Visible mould in soil
- Frequent flare-ups
- Clinical advice recommends stricter avoidance
Some people remove plants temporarily during unstable periods and reintroduce them later.
❓ Common questions
Are leaves dangerous?
No—the main risk comes from soil and decaying material.
Is outdoor gardening riskier?
Yes, due to higher exposure. Wearing a mask is recommended.
Do air purifiers help?
HEPA filters may reduce airborne particles, but evidence specific to ABPA is limited.
⚠️ When to seek medical advice
- Increasing breathlessness or wheeze
- Worsening cough or mucus
- Reduced peak flow
- Symptoms linked to specific environments
Do not change treatment without medical advice.
📚 References & Further Reading
- What is aspergillosis?
- Reducing exposure to mould
- World Health Organization – Indoor air quality guidance
- UK Health Security Agency – Damp and mould health risks
👩⚕️ Author & Review
Developed for patient education in line with UK specialist practice (National Aspergillosis Centre, Manchester).
This information is general and does not replace individual medical advice.
Looking for more answers? Visit our
patient questions hub.
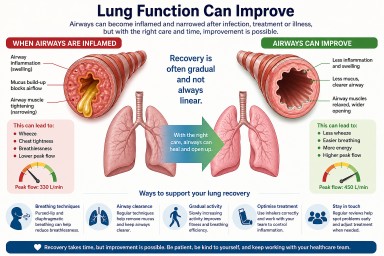
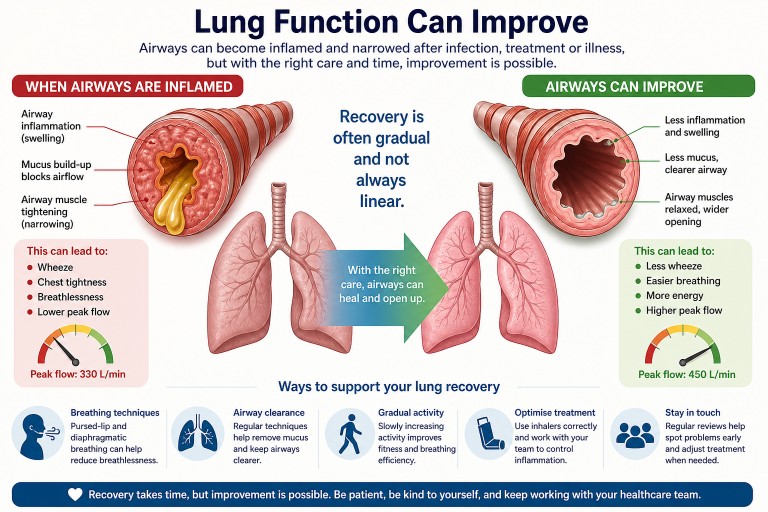
Can Lung Function Improve After Infection or Treatment?
Last reviewed: May 2026
Audience: Patients, carers, and non-specialists
Key Points
- Lung function often can improve after infections, chemotherapy, or inflammation—but recovery may take weeks to months.
- A drop in peak flow usually reflects airway narrowing, inflammation, or mucus, not always permanent damage.
- Normal oxygen levels (e.g. 95–100%) are reassuring and suggest gas exchange is still working well.
- Symptoms like breathlessness and wheeze can persist even while the lungs are gradually recovering.
- If symptoms are not improving, further assessment may help identify treatable causes.
Contents
- Can lung function recover?
- Why has my lung function dropped?
- Why does recovery feel slow or “stuck”?
- What might help?
- Breathing techniques in detail
- When might further tests be needed?
- Common questions
- When to seek medical advice
Can lung function recover?
In many cases, yes—lung function can improve after a significant illness such as a chest infection, chemotherapy, or inflammation affecting the airways.
However, recovery is often gradual and not always straightforward. It may take:
- Several weeks after an infection
- Several months after more severe illness or treatment
It is also common for symptoms to fluctuate during recovery rather than steadily improve.
Why has my lung function dropped?
A reduction in peak flow or increased breathlessness does not always mean permanent damage. Common causes include:
- Airway inflammation (swelling inside the breathing tubes)
- Mucus build-up, which can block airflow
- Airway narrowing or spasm, similar to asthma
- Post-infectious sensitivity (airways remain irritated after infection)
- Reduced fitness after illness (deconditioning)
In some patients, conditions such as Allergic Bronchopulmonary Aspergillosis (ABPA) or other airway diseases can contribute to ongoing symptoms.
Important: If oxygen levels remain normal (for example, around 97%), this suggests that the lungs are still transferring oxygen effectively, which is reassuring.
Why does recovery feel slow or “stuck”?
Many people feel frustrated because they are doing everything “right” but not seeing improvement. This is very common.
Possible reasons include:
- Residual mucus that is difficult to clear
- Ongoing low-level inflammation
- Airways that remain sensitive after infection
- Effects of steroid treatment, especially during dose changes
- Fatigue and reduced activity levels
Recovery can happen slowly in the background, even when symptoms remain noticeable.
What might help?
Different approaches may support recovery. These should be discussed with your clinical team where appropriate.
1. Airway clearance
- Regular airway clearance techniques can help remove mucus
- Some people benefit from devices that assist mucus clearance
2. Breathing techniques
Breathing techniques can help reduce breathlessness and improve control. A more detailed guide is provided below.
3. Gradual activity
- Slowly increasing activity levels can rebuild strength
- Pacing is important—avoid pushing too hard too quickly
4. Optimising treatment
- Ensuring inhaler technique is correct
- Reviewing whether airway inflammation is fully controlled
Breathing Techniques in Detail
Breathing techniques can help reduce breathlessness, improve airflow, and make breathing feel more controlled—especially when airways are inflamed or narrowed.
They do not treat the underlying condition directly, but they can improve symptoms, confidence, and daily activity.
Pursed-Lip Breathing
What it does: Helps keep airways open for longer during breathing out, reducing air trapping and easing breathlessness.
How to do it:
- Breathe in slowly through your nose (about 2 seconds)
- Purse your lips (as if whistling)
- Breathe out slowly through your lips (about 4 seconds)
- Keep the breath out gentle, not forced
When to use it:
- During breathlessness
- With activity (e.g. walking, stairs)
- To regain control of breathing
Tip: Aim for a longer out-breath than in-breath.
Diaphragmatic (Belly) Breathing
What it does: Encourages more efficient breathing using the diaphragm rather than upper chest muscles.
How to do it:
- Sit or lie comfortably
- Place one hand on your chest, one on your abdomen
- Breathe in through your nose and allow your abdomen to rise
- Breathe out slowly (through pursed lips if helpful)
Tip: Keep shoulders relaxed and avoid lifting the chest.
Breathing Control (for flare-ups)
- Pause and rest
- Breathe slowly through the nose
- Breathe out gently through relaxed or pursed lips
- Release tension in shoulders and neck
Helpful positions:
- Sitting leaning forward with arms supported
- Standing leaning on a surface
“Blow as You Go”
Use during activity:
- Breathe in before effort
- Breathe out during effort (e.g. standing up, climbing)
This helps prevent breath-holding and reduces strain.
Important: These techniques should feel comfortable and controlled. If symptoms worsen, stop and rest.
When might further tests be needed?
If symptoms are persistent, worsening, or not improving as expected, your clinical team may consider:
- Spirometry (lung function tests)
- Imaging such as a chest CT scan
- Assessment for:
- Airway inflammation
- Bronchiectasis
- Fungal-related lung disease
Common Questions
Does a drop in peak flow mean permanent damage?
No. Peak flow mainly reflects how open your airways are and can improve with treatment.
Why do I feel breathless if my oxygen levels are normal?
Breathlessness is often caused by airway narrowing or inefficient breathing, not low oxygen.
Can lungs fully recover?
Some people return to their previous baseline. Others improve significantly but may not reach exactly the same level.
When to seek medical advice
- Worsening breathlessness
- Increasing wheeze or chest tightness
- New or persistent cough
- Changes in sputum (including blood)
- No improvement over time
If symptoms suddenly worsen, seek urgent medical attention.
Final Thoughts
A drop in lung function after infection or treatment can feel worrying, but it often reflects treatable airway changes. Improvement is possible, although recovery may take time.
Staying in contact with your healthcare team helps ensure that any ongoing issues are identified and managed appropriately.
References & Further Reading
- British Thoracic Society (BTS) guidance
- European Respiratory Society (ERS) patient resources
- National Aspergillosis Centre patient information
This article is for general information only and does not replace medical advice. Always consult your healthcare team.
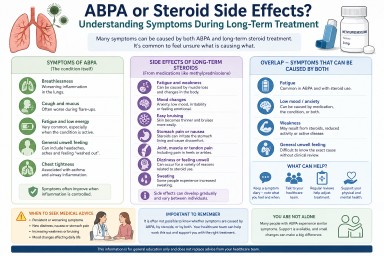
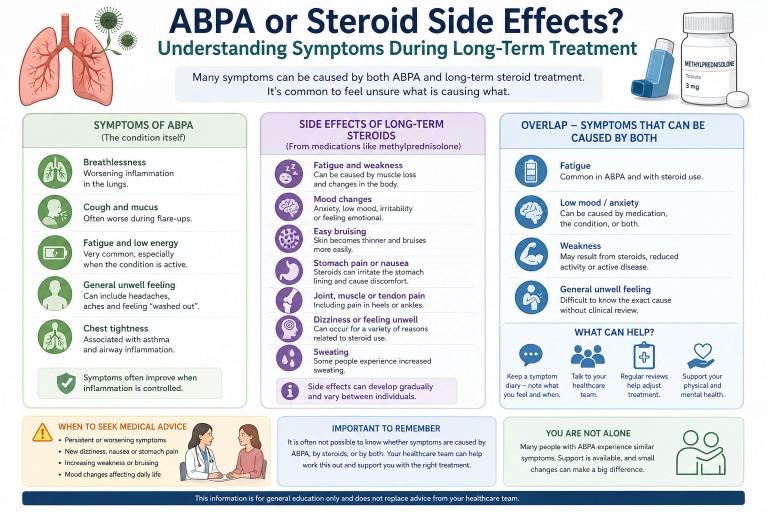
ABPA or Steroid Side Effects? Understanding Symptoms During Long-Term Treatment
Last reviewed: April 2026
Many people living with Allergic Bronchopulmonary Aspergillosis (ABPA) who take long-term steroids find it difficult to tell whether their symptoms are caused by the condition or the treatment.
Symptoms in ABPA can come from both the condition and long-term steroid treatment. Fatigue, weakness, mood changes, and general unwellness are common to both, making it difficult to identify a single cause without clinical review.
This is especially true for people taking corticosteroids such as methylprednisolone or prednisolone.

---
Key Points
- ABPA and steroid treatment can cause overlapping symptoms.
- Fatigue, low mood, and general unwellness can come from either the condition or medication.
- Long-term corticosteroid use can cause additional side effects.
- It is common to feel unsure what is causing symptoms.
- Ongoing or worsening symptoms should be discussed with your healthcare team.
---
Why is it hard to tell the difference?
ABPA is an immune-driven lung condition that causes inflammation. Treatment often includes corticosteroids such as methylprednisolone or prednisolone, which reduce inflammation but can also affect many systems in the body.
This means that:
- The disease itself can cause symptoms
- The treatment can also cause symptoms
As a result, people often experience a combination of both.
---
Symptoms caused by ABPA
ABPA commonly affects the lungs but can also cause more general symptoms.
- Fatigue and low energy
- Breathlessness
- Cough and mucus production
- Chest tightness
- General feeling of being unwell
Fatigue can be particularly prominent, especially during flare-ups.
---
Side effects of long-term steroids
Corticosteroids such as methylprednisolone are highly effective treatments, but long-term use can lead to a range of side effects.
- Fatigue and weakness (including muscle loss)
- Mood changes (anxiety, low mood, irritability)
- Easy bruising (skin becomes thinner)
- Stomach irritation or pain
- Dizziness or feeling unwell
- Sweating
- Bone or joint discomfort
Learn more about treatment approaches in aspergillosis treatment options.
---
Where symptoms overlap
Some symptoms can be caused by both ABPA and steroid treatment, making them difficult to interpret.
| Symptom | Possible cause |
|---|---|
| Fatigue | ABPA inflammation or steroid effects |
| Low mood / anxiety | Medication effects or impact of chronic illness |
| Weakness | Muscle loss from steroids or reduced activity |
| General unwell feeling | Both |
This overlap is one of the most challenging aspects of long-term management.
🔎 Not sure what’s causing your symptoms?
Many people with ABPA feel exactly the same—this overlap is one of the most common challenges during long-term treatment.
---
Understanding specific symptoms
Some symptoms are more commonly linked to treatment effects:
- Easy bruising – often related to steroid use
- Heel or ankle pain – may relate to tendon or joint effects
- Stomach pain – can be linked to steroid irritation
Other symptoms, such as fatigue, dizziness, and nausea, may have multiple possible causes.
Because of this, it is often not possible to attribute symptoms to a single cause without clinical review.
---
When to seek medical advice
You should contact your healthcare team if you experience:
- Persistent or worsening fatigue
- New dizziness or nausea
- Ongoing stomach pain
- Increasing weakness
- Mood changes affecting daily life
These symptoms do not necessarily indicate a serious problem, but they may mean that treatment or support needs to be reviewed.
---
Summary
In ABPA, symptoms such as fatigue, weakness, and low mood can arise from both the condition and its treatment. Long-term steroid use can add additional effects, making it difficult to distinguish between causes.
If symptoms are persistent or worsening, it is important to discuss them with your healthcare team so that appropriate adjustments or support can be considered.
---
Further Reading
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Treatment of Aspergillosis
- Weight Loss and Weakness in Aspergillosis
---
Author & Review
Prepared for aspergillosis.org to support patient understanding. Content reflects current clinical knowledge and patient-reported experience.
Disclaimer
This information is for general education only and does not replace advice from your healthcare team.
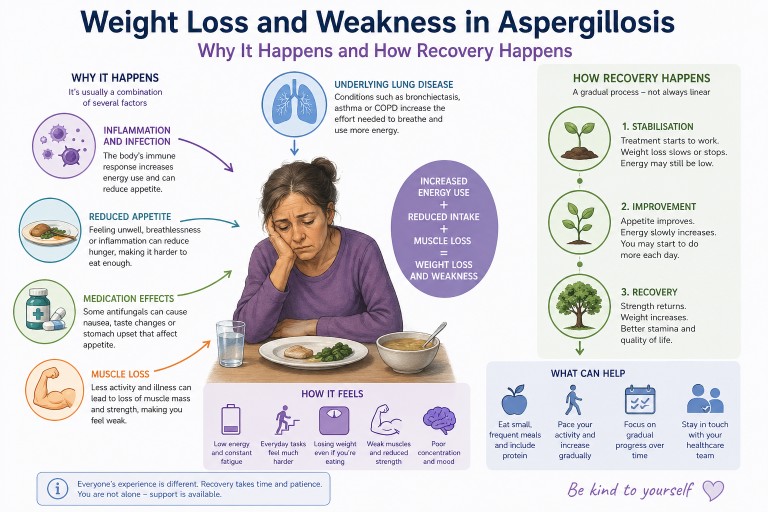
Weight Loss and Weakness in Aspergillosis: Why It Happens, How It Feels, and What Helps Recovery
Last reviewed: April 2026
Unexpected weight loss and severe weakness are among the most worrying symptoms people report after being diagnosed with aspergillosis. Many describe feeling unlike themselves—physically drained, thinner than they have ever been, and struggling with everyday activities.
This article explains why this happens, what is going on in the body, and what recovery typically looks like.
---
Key Points
- Weight loss and fatigue are common in aspergillosis, particularly early in the illness or during flare-ups.
- They are usually caused by a combination of inflammation, increased energy use, reduced appetite, and muscle loss.
- Medication side effects can contribute but are rarely the main cause.
- Many people improve over time, but recovery is usually gradual and can take weeks to months.
- Stabilising weight is often the first important step before regaining strength.
---
Contents
- Why does aspergillosis cause weight loss?
- What is happening inside the body?
- Which types of aspergillosis are affected?
- Why does it feel so severe?
- Does it get better?
- What can help day to day?
- Nutrition and rebuilding strength
- When to seek medical advice
- Common questions
---
Why does aspergillosis cause weight loss?
Weight loss in aspergillosis is rarely due to a single cause. Instead, it is usually the result of several overlapping processes.
1. Increased energy use (hypermetabolism)
When the body is dealing with infection or inflammation, it requires more energy. This is sometimes described as a hypermetabolic state.
- The immune system is active and consumes energy
- The body produces inflammatory signals
- Breathing effort may increase
This means you may be burning more calories than usual—even at rest.
2. Reduced appetite
Many people notice they are eating less, sometimes without realising it. This may be due to:
- Feeling unwell or fatigued
- Shortness of breath when eating
- Changes in appetite driven by inflammation
3. Medication effects
Some treatments can affect appetite or digestion. For example:
- Antifungal medications such as itraconazole or voriconazole may cause nausea or taste changes
- Steroids may increase appetite but can also contribute to muscle weakness over time
Medication effects vary widely and are usually only part of the overall picture.
4. Muscle breakdown
During illness, the body may break down muscle to meet energy needs. This can happen quickly, especially if activity levels fall.
This leads to:
- Loss of strength
- Reduced stamina
- A feeling of being “weak” rather than just lighter
5. Underlying lung disease
Many people with aspergillosis also have conditions such as bronchiectasis, asthma, or chronic obstructive pulmonary disease (COPD). These can increase the effort required for breathing and contribute to ongoing energy use.
---
What is happening inside the body?
Several biological processes contribute to weight loss and fatigue:
- Inflammatory signalling: The immune system releases chemical signals that affect metabolism and appetite
- Catabolism: The body breaks down tissues (including muscle) to release energy
- Energy imbalance: More energy is used than consumed
This combination can make weight loss feel rapid and difficult to control.
---
Which types of aspergillosis are affected?
These symptoms are most commonly seen in:
- Chronic Pulmonary Aspergillosis (CPA)
- Allergic Bronchopulmonary Aspergillosis (ABPA), particularly during flare-ups
However, not everyone experiences weight loss, and severity varies.
---
Why does it feel so severe?
Many people describe this stage as one of the most difficult parts of their illness. This is because several factors are happening at once:
- Physical energy is reduced
- Muscle strength has declined
- The body is under ongoing stress
- Recovery has not yet begun
This can make everyday activities—such as walking, cooking, or even eating—feel unusually difficult.
---
Does it get better?
In many cases, yes—there is gradual improvement over time, especially once treatment begins to control the condition.
Recovery often follows a pattern:
- Initial phase: weight loss and severe fatigue
- Stabilisation: weight loss slows or stops
- Recovery: gradual return of strength and energy
This process is usually slow and uneven, with good and bad days.
---
What can help day to day?
1. Focus on maintaining nutrition
- Eat small amounts regularly rather than large meals
- Choose foods that are easy to prepare and eat
- Include protein to support muscle maintenance
2. Pace activity carefully
- Gentle movement can help maintain strength
- Avoid pushing too hard, as this can worsen fatigue
- Increase activity gradually as energy improves
3. Look at trends over time
It can be helpful to focus on gradual changes such as:
- Weight stabilising
- Small improvements in energy
---
Nutrition and rebuilding strength
Recovery often happens in stages:
- Stage 1: Stabilising weight
- Stage 2: Gradually increasing intake
- Stage 3: Rebuilding muscle and strength
Regaining muscle mass takes time and usually follows once the underlying condition is better controlled.
---
When to seek medical advice
You should contact your healthcare team if you experience:
- Continued or rapid weight loss
- Increasing weakness
- Difficulty eating or swallowing
- New or worsening symptoms
This may indicate the need for additional support or adjustment of treatment.
---
Common questions
Is weight loss just due to poor appetite?
No. Reduced appetite is only one factor. Increased energy use and muscle loss are also important contributors.
Are medications the main cause?
Medications can contribute, but they are rarely the main reason for weight loss.
Will I regain my strength?
Many people do regain strength over time, although recovery is usually gradual.
Why does recovery take so long?
The body needs time to reduce inflammation, restore energy balance, and rebuild muscle.
---
Summary
Weight loss and weakness in aspergillosis are common and can feel severe, particularly early in the illness. They are usually caused by a combination of increased energy use, reduced appetite, muscle loss, and underlying lung disease.
Although recovery can take time, many people improve gradually as treatment takes effect.
---
Further Reading
- Chronic Pulmonary Aspergillosis (CPA)
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Treatment of Aspergillosis
---
Author & Review
Prepared for aspergillosis.org to support patient understanding. Content reflects current clinical knowledge and patient-reported experience.
Disclaimer
This page is for general information only and does not replace advice from your healthcare team.