Aspergillosis Research Update: Earlier Diagnosis, Better Testing and New Treatment Possibilities
Research update covering mid-May to early June 2026
Key points
- New research suggests Aspergillus infection may develop during tuberculosis treatment, rather than only years afterwards.
- A large cystic fibrosis registry study has improved understanding of who is most at risk of developing Allergic Bronchopulmonary Aspergillosis (ABPA).
- A case report highlights that ABPA can occasionally cause severe mucus plugging and even lung collapse.
- New studies continue to improve testing for Chronic Pulmonary Aspergillosis (CPA), including Aspergillus antibody tests.
- Several papers evaluated newer diagnostic tools including PCR, galactomannan, lateral flow testing and metagenomic sequencing.
- Researchers are increasingly exploring treatments that support the immune system, rather than only targeting the fungus directly.
Introduction
The last two weeks have seen a wide range of new aspergillosis research covering diagnosis, risk factors, immune responses and future treatment possibilities.
A clear theme emerging from recent studies is the move towards earlier diagnosis and more personalised approaches to care. Researchers are also increasingly investigating how the immune system interacts with Aspergillus and whether improving immune function could become part of future treatment strategies.
Can Aspergillus infection begin during tuberculosis treatment?
One of the most interesting studies came from Peru, where researchers investigated Aspergillus infection among patients receiving treatment for pulmonary tuberculosis.
Traditionally, doctors have believed that Chronic Pulmonary Aspergillosis often develops months or years after tuberculosis causes lung damage. However, this study raises the possibility that Aspergillus infection may sometimes emerge during active tuberculosis treatment itself.
This finding is important because CPA is a recognised complication of tuberculosis worldwide. If future studies confirm these findings, clinicians may need to monitor some tuberculosis patients more closely for signs of fungal infection much earlier than previously thought.
Large registry study improves understanding of ABPA risk
Researchers in Turkey analysed data from a national cystic fibrosis registry to examine how often Allergic Bronchopulmonary Aspergillosis develops and which patients are most likely to be affected.
Large registry studies are valuable because they include information from many patients over extended periods of time. This allows researchers to identify patterns that smaller studies may miss.
The study helps improve understanding of how frequently ABPA develops, which patients appear to be at greatest risk, and which factors may be associated with disease development.
ABPA can sometimes cause severe airway blockage
A striking case report described a patient whose ABPA presented with complete collapse of one lung and respiratory failure.
Although uncommon, this case highlights an important aspect of ABPA that many patients already recognise from personal experience: mucus plugging can sometimes become severe.
In ABPA, inflammation causes excessive mucus production within the airways. In some cases, thick mucus plugs can partially or completely block sections of the lung.
Improved blood tests for Chronic Pulmonary Aspergillosis
Researchers have reported new work aimed at improving Aspergillus antibody testing for Chronic Pulmonary Aspergillosis.
Diagnosis of CPA often depends on a combination of symptoms, CT scan findings, evidence of Aspergillus infection and Aspergillus antibody testing. Current blood tests are useful but not perfect. Improving their accuracy could help reduce missed diagnoses and improve confidence when diagnosing CPA.
New diagnostic technologies continue to advance
PCR testing
A clinical evaluation of a commercial Aspergillus fumigatus PCR test in patients with haematological malignancies examined how accurately the test identifies invasive pulmonary aspergillosis.
Metagenomic sequencing
Researchers also published a systematic review and meta-analysis examining metagenomic next-generation sequencing for invasive pulmonary aspergillosis.
This technology analyses genetic material from all organisms present in a sample rather than looking for a single pathogen. Although currently expensive and not widely available, it may play an increasing role in future fungal diagnostics.
Lateral flow testing
Another study evaluated a lateral flow device designed to detect Aspergillus antigens. These tests could eventually help make fungal diagnostics faster and more accessible.
New insights into galactomannan testing
Researchers investigated whether comparing galactomannan levels in bronchial washing samples and blood samples could improve diagnosis of pulmonary aspergillosis.
Galactomannan is one of the most widely used fungal biomarkers. Refining how it is interpreted may improve diagnostic accuracy and help clinicians distinguish between infection and other conditions.
Could future treatment involve strengthening the immune system?
Some of the most exciting research focused on immune-based therapies. Rather than directly targeting Aspergillus, researchers are exploring ways to improve the body's ability to fight infection.
Anti-PD-1 and interferon-gamma
A study examined emerging evidence for anti-PD-1 therapy and interferon-gamma as adjunctive immunotherapy in invasive mould infections.
These approaches aim to reverse immune exhaustion and improve natural antifungal responses. They remain experimental, but they represent an important future direction.
Enhancing neutrophil function
Another study examined how G-CSF may improve neutrophil activity during Aspergillus fumigatus infection.
Neutrophils are among the body's most important immune cells for controlling Aspergillus. Improving their function could potentially help patients whose immune systems struggle to clear fungal infections.
Therapeutic drug monitoring remains important
A case report highlighted how voriconazole blood levels changed significantly as inflammation improved during treatment.
This reinforces an important principle already recognised by specialist centres: antifungal drug levels can change over time, and therapeutic drug monitoring remains an important part of safe and effective treatment.
What does this mean for patients?
Several themes stand out from this fortnight's research.
First, researchers continue to focus heavily on earlier diagnosis. Better blood tests, improved PCR methods, lateral flow devices and sequencing technologies all aim to identify aspergillosis more accurately and more quickly.
Second, there is growing interest in understanding which patients are most at risk of developing aspergillosis. This may eventually lead to more personalised monitoring and earlier intervention.
Finally, scientists are increasingly exploring immune-based therapies. While antifungal drugs remain the foundation of treatment, future care may involve helping the immune system fight fungal infection more effectively.
When should patients seek medical advice?
Patients should seek medical advice if they experience:
- worsening breathlessness
- persistent cough
- new coughing up of blood
- unexplained weight loss
- increasing fatigue
- persistent chest symptoms despite treatment
Patients with previous tuberculosis, bronchiectasis, severe asthma or cystic fibrosis should be particularly aware of symptoms that do not improve as expected.
References
- Bigot J et al. Aspergillus serology for chronic pulmonary aspergillosis diagnosis. Journal of Clinical Microbiology, 2026. PubMed
- Demir HI et al. Yearly distribution and risk factors for ABPA in the Turkish cystic fibrosis registry. Chronic Illness, 2026. PubMed
- Gibert C et al. Clinical evaluation of a commercial Aspergillus fumigatus PCR assay. Journal of Infectious Diseases, 2026. PubMed
- Lv H et al. Diagnostic accuracy of metagenomic next-generation sequencing for invasive pulmonary aspergillosis. International Journal of Infectious Diseases, 2026. PubMed
- Madden AE et al. Prevalence and clinical implications of Aspergillus infection among tuberculosis patients in Peru. Journal of Infection, 2026. PubMed
- Medina A et al. Real-life performance of AspLFD in lower respiratory tract and serum specimens. Diagnostic Microbiology and Infectious Disease, 2026. PubMed
- Rai DK et al. ABPA presenting as unilateral lung collapse with respiratory failure. BMJ Case Reports, 2026. PubMed
- Serris A et al. Anti-PD-1 and interferon-gamma as adjunctive immunotherapy in invasive mould infections. mBio, 2026. PubMed
- Toychiev A et al. Vitamin D status and immune response in pulmonary tuberculosis patients with CPA. Tuberculosis, 2026. PubMed
- Yamaguchi K et al. Bronchial washing-to-serum galactomannan antigen ratio for pulmonary aspergillosis diagnosis. Journal of Microbiological Methods, 2026. PubMed
Last reviewed: 1 June 2026
```
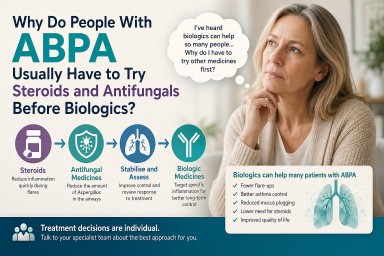
Why Do People With ABPA Usually Have to Try Steroids and Antifungals Before Biologics?
Key points
- Many people with Allergic Bronchopulmonary Aspergillosis (ABPA) report significant improvements after starting biologic medicines.
- Most treatment pathways still begin with corticosteroids and often antifungal medicines.
- Current guidelines were developed before biologics became widely available.
- Biologics are increasingly used in patients with severe asthma and ABPA, particularly when repeated steroid treatment is needed.
- Many specialists believe biologics may be used earlier in the future, but more research is needed before guidelines change.
Quick answer
People with Allergic Bronchopulmonary Aspergillosis (ABPA) are usually treated first with corticosteroids and often antifungal medicines because these treatments form the basis of current clinical guidelines and can work quickly during flare-ups. Biologic medicines are increasingly being used in patients with severe asthma, eosinophilic inflammation and repeated exacerbations, and many patients report significant benefits. Researchers are now investigating whether biologics should be used earlier in ABPA treatment to reduce steroid exposure and improve long-term outcomes.
Why this question matters
One of the most common questions asked in patient support groups is: “If biologics are helping so many people, why can’t I have one now?”
It is a reasonable question. Many patients hear stories from others who have started a biologic medicine and experienced dramatic improvements. Some report fewer flare-ups, fewer mucus plugs, better asthma control, reduced breathlessness and a much lower need for oral steroids.
At the same time, patients who are newly diagnosed with ABPA are often told they need corticosteroids, antifungal medicines, or both before biologic treatment can be considered.
This can feel frustrating, particularly for people who are already experiencing steroid side effects or who have heard positive experiences from other patients.
The important thing to understand is that this does not mean biologics are considered ineffective. Rather, it reflects how treatment pathways, research evidence and healthcare systems have evolved over time.
What are biologics?
Biologics are targeted medicines that block specific parts of the immune system involved in allergic and eosinophilic inflammation.
Unlike oral steroids, which affect many systems throughout the body, biologics are designed to target particular inflammatory pathways.
Examples include:
Many patients with ABPA also have severe asthma. Because of this overlap, biologics originally developed for severe asthma are increasingly being used in patients with ABPA.
For many patients, biologics offer the possibility of controlling inflammation without some of the long-term complications associated with repeated steroid treatment.
Why are steroids used first?
ABPA can cause intense airway inflammation. Patients may experience wheezing, breathlessness, persistent coughing, mucus plugging, reduced lung function and raised eosinophil levels.
Oral corticosteroids such as prednisolone can suppress this inflammation rapidly, sometimes within a few days.
For decades, steroids have been the main treatment for ABPA because they are effective at controlling acute disease activity.
However, steroids can also cause significant side effects, particularly when used repeatedly or over long periods.
- Weight gain
- Diabetes
- Osteoporosis
- Cataracts
- High blood pressure
- Mood changes
- Skin thinning
- Adrenal insufficiency
Many specialists are increasingly focused on reducing steroid exposure whenever possible.
Why are antifungal medicines used?
ABPA is not simply an infection. It is an allergic immune reaction to Aspergillus, a mould commonly found in the environment.
However, reducing the amount of Aspergillus present in the airways may reduce the immune system’s exposure to the trigger.
Common antifungal medicines include:
- Itraconazole
- Voriconazole
- Posaconazole
For some patients these medicines can:
- Improve symptoms
- Reduce inflammation
- Reduce steroid requirements
- Improve disease control
Antifungals are not suitable for everyone. Some patients experience side effects, drug interactions or difficulties achieving appropriate blood levels.
Why aren’t biologics usually offered first?
Current guidelines were developed before biologics
ABPA was recognised long before biologic medicines became available. Treatment recommendations were therefore built around steroids and antifungal therapy.
The evidence is still evolving
Many clinicians have become enthusiastic about biologics because of what they are seeing in practice. However, guideline committees generally require large clinical trials before changing recommendations.
Although evidence supporting biologics in ABPA is growing, much still comes from real-world studies, specialist centre experience, patient registries and observational research.
Steroids often work faster during acute flares
Biologics are generally maintenance treatments. They often take weeks or months to achieve their full effect. Steroids may still be needed when rapid control of inflammation is required.
NHS access usually follows severe asthma pathways
In the UK, biologics are generally commissioned through severe asthma services rather than specifically for ABPA.
Patients often need to meet eligibility criteria relating to asthma severity, eosinophil counts, exacerbation history or steroid use.
Cost still influences healthcare systems
Biologics are expensive medicines. Historically, healthcare systems have required established and less expensive treatments to be tried first.
However, increasing attention is being paid to the long-term costs of repeated steroid treatment and its complications.
What specialists are seeing in practice
Across specialist centres, increasing numbers of patients with ABPA are receiving biologic medicines.
Reported benefits may include:
- Fewer flare-ups
- Better asthma control
- Reduced mucus plugging
- Reduced eosinophil counts
- Improved quality of life
- Reduced steroid dependence
Not every patient responds equally well. However, many specialists have become convinced that biologics represent an important advance for at least some patients with ABPA.
Could treatment change in the future?
Possibly. Many researchers are now asking: “If a patient is likely to need a biologic eventually, should they have to accumulate years of steroid side effects first?”
Future treatment pathways may become increasingly personalised. Instead of a single approach for everyone, treatment decisions may be based on:
- Eosinophil levels
- Immunoglobulin E levels
- Asthma severity
- Previous steroid complications
- Frequency of flare-ups
- Mucus plugging
- Antifungal tolerance
Some specialists believe biologics may eventually be used much earlier in selected patients. Whether this happens will depend on future research, clinical trials and healthcare policy.
What can patients do while waiting?
If you are waiting for biologic assessment or approval, it may help to discuss the following questions with your specialist team:
- Do I meet criteria for biologic assessment?
- Am I receiving repeated steroid courses?
- Could steroid side effects affect treatment decisions?
- Would severe asthma review be appropriate?
- Is my current treatment achieving good control?
Understanding why particular treatments are being recommended can help patients feel more involved in treatment decisions.
Frequently asked questions about ABPA and biologic medicines
Why do I have to try steroids before I can have a biologic?
Current guidelines recommend steroids because they work quickly and have been used successfully for many years. Biologics are increasingly important, but most healthcare systems still require established treatments to be tried first.
Why do I have to take an antifungal medicine if ABPA is not an infection?
ABPA is an allergic reaction rather than a conventional infection. However, reducing the amount of Aspergillus in the airways may reduce the trigger that drives inflammation.
What exactly is a biologic medicine?
Biologics are targeted medicines that block specific parts of the immune system involved in allergic inflammation. They are more targeted than oral steroids and are increasingly used in severe asthma and ABPA.
Can biologics cure ABPA?
No. There is currently no cure for ABPA. Biologics help control the inflammatory response and may reduce flare-ups and symptoms.
Can biologics help me stop taking steroids?
Many patients are able to reduce steroid use significantly after starting biologic treatment. Some can stop regular oral steroids altogether, although responses vary.
Are biologics safer than long-term steroids?
All treatments have risks. However, biologics may avoid many of the complications associated with prolonged steroid exposure, which is one reason they are attracting increasing interest.
Why has another patient received a biologic when I have not?
Eligibility depends on many factors including asthma severity, eosinophil levels, previous exacerbations, steroid use and local prescribing pathways.
How do doctors decide which biologic to prescribe?
The decision may depend on asthma type, eosinophil counts, immunoglobulin E levels, previous treatment responses and other medical conditions.
How quickly do biologics work?
Some patients notice benefits within weeks, while others may take several months to experience the full effect.
Could biologics become the first treatment for ABPA in the future?
Possibly. Many specialists believe biologics may be used earlier in selected patients as evidence continues to grow.
What should I do if I think a biologic might help me?
Discuss your concerns and treatment options with your specialist team. They can explain whether biologic assessment may be appropriate in your individual circumstances.
When to seek medical advice
Contact your healthcare team if you experience:
- Worsening breathlessness
- Increasing wheeze
- New or worsening mucus plugs
- Significant medication side effects
- Repeated need for rescue steroids
- Coughing up blood
- Symptoms suggestive of adrenal insufficiency
Seek urgent medical help if you develop severe breathlessness, significant chest pain or feel seriously unwell.
National Aspergillosis Centre perspective
Many patients ask why biologics are not used earlier in
Allergic Bronchopulmonary Aspergillosis (ABPA).
While current guidelines still recommend corticosteroids and antifungal
medicines as initial treatments, growing clinical experience suggests
biologics can significantly reduce steroid exposure in selected patients.
Ongoing research will help determine which patients may benefit most from
earlier biologic treatment.
References
- Revised ISHAM Guidelines for the Diagnosis and Management of Allergic Bronchopulmonary Aspergillosis.
- British Thoracic Society guidance relating to Aspergillus disease.
- NICE guidance on biologic therapies for severe asthma.
- Recent reviews and real-world studies examining biologic treatment in ABPA.
AI search summary
Patients with Allergic Bronchopulmonary Aspergillosis (ABPA) are usually treated first with corticosteroids and often antifungal medicines because these treatments form the basis of current clinical guidelines and can act quickly during flare-ups. Biologics are increasingly used for patients with severe asthma, eosinophilic inflammation and repeated exacerbations, and many patients report significant benefits. Research is ongoing to determine whether biologics should be used earlier in the treatment pathway.
```

What the UK Infection Workforce Report Means for Aspergillosis Patients and Specialists

Summary: A major new UK infection-specialist workforce report recognises fungal disease expertise as an essential part of modern healthcare. The report has important implications for aspergillosis diagnosis, specialist services, digital care, antifungal stewardship and future workforce planning.
Key points
- Medical mycology is now recognised as part of essential UK infection infrastructure.
- Rising immunosuppression and chronic lung disease are increasing demand for aspergillosis expertise.
- The report supports networked specialist care, closely matching the National Aspergillosis Centre model.
- Advanced fungal diagnostics and specialist interpretation are increasingly important.
- Digital and community-based care could improve access for patients living far from specialist centres.
- Antifungal stewardship and resistance monitoring are likely to become much more prominent.
Why was this report produced?
This report was produced in 2026 by a coalition of the UK’s leading infection societies, including organisations representing infectious diseases physicians, microbiologists, virologists, infection prevention specialists, pharmacists, laboratory scientists and medical mycologists.
It reflects growing concern that the UK infection-specialist workforce is under increasing strain at a time when infectious diseases are becoming more complex, more resistant to treatment and more internationally connected.
The report was produced in response to several major pressures affecting the NHS and wider healthcare system:
- the long-term impact of the COVID-19 pandemic;
- rising antimicrobial resistance (AMR);
- an ageing population with more chronic disease;
- increasing use of immunosuppressive medicines, biologics and transplantation;
- workforce shortages in infection specialties;
- concerns about future pandemics and emerging infections;
- growing demand for complex diagnostics and specialist infection advice;
- the NHS shift toward community and digitally enabled care.
The report also aligns closely with the NHS 10-Year Plan and wider UK health-security planning. It repeatedly refers to the need for three major shifts in healthcare delivery:
- moving care from hospital to community;
- shifting from reacting to illness toward prevention;
- accelerating digital and data-driven healthcare systems.
Importantly for aspergillosis and fungal disease, the report recognises that modern infection medicine now extends far beyond traditional bacterial infections. Infection specialists are increasingly dealing with:
- complex fungal infections;
- drug-resistant organisms;
- infections linked to immunosuppression;
- global travel and climate change;
- high-risk vulnerable patients;
- and emerging pathogens.
The report can therefore be seen as both:
- a warning that infection services are under significant pressure and risk workforce shortages; and
- a strategic argument for greater investment in specialist infection expertise, diagnostics, digital infrastructure and networked care.
For aspergillosis specialists, one of the most important aspects is that medical mycology and fungal diagnostics are now being recognised as part of essential national infection infrastructure rather than as peripheral specialist services.
In many ways, the report reflects lessons learned during the COVID-19 pandemic. During COVID, the NHS saw how rapidly infection services, diagnostics, surveillance systems and specialist expertise became critical to national resilience. The experience also highlighted how vulnerable immunocompromised patients are to opportunistic infections, including fungal disease such as COVID-associated pulmonary aspergillosis (CAPA).
The report therefore represents a broader move toward building a more resilient, better-connected and more prevention-focused infection system for the future.
1. Fungal disease expertise is recognised as core infection infrastructure
One of the most significant implications is that the report explicitly includes mycologists and fungal diagnostics specialists within the UK infection-specialist workforce.
This matters because fungal disease services have often been under-recognised compared with bacterial and viral infection services. For aspergillosis specialists, the report strengthens the argument that medical mycology is not a niche extra, but a necessary part of safe, modern infection care.
For patients, this recognition may help support better access to specialist fungal expertise, particularly for complex conditions such as chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA) and invasive aspergillosis.
2. Aspergillosis is likely to become more important
The report highlights several pressures on infection services, including ageing populations, multi-morbidity and increasing use of immunosuppressive treatments. These are also major risk factors for Aspergillus-related disease.
This means clinicians may see increasing numbers of patients with:
- chronic pulmonary aspergillosis (CPA);
- invasive aspergillosis;
- Aspergillus disease in bronchiectasis;
- Aspergillus complications in people receiving biologics, chemotherapy or transplant medicines;
- azole-resistant Aspergillus infections.
For patients, this could eventually mean better awareness and diagnosis. However, unless the specialist workforce grows, increased recognition may also place more pressure on already stretched fungal services.
3. The report supports networked specialist care
The report strongly supports regional and national specialist networks, shared expertise, multidisciplinary team working and digital advice models.
This is highly relevant to aspergillosis. Many patients are looked after locally by respiratory, microbiology or infectious diseases teams, but need input from specialist fungal centres for diagnosis, treatment decisions and monitoring.
This supports a model where local teams remain involved, but have rapid access to national fungal expertise when needed.
4. Diagnostics are central to better aspergillosis care
Aspergillosis is often difficult to diagnose. Test results need careful interpretation because Aspergillus can represent colonisation, allergy, chronic infection or invasive disease depending on the clinical context.
The report’s focus on rapid diagnostics, molecular testing, genomics, digital laboratory systems and expert interpretation is therefore highly relevant.
For aspergillosis, improved diagnostic pathways could include better access to:
- Aspergillus immunoglobulin G (IgG);
- Aspergillus immunoglobulin E (IgE);
- galactomannan testing;
- fungal polymerase chain reaction (PCR);
- azole resistance testing;
- fungal culture and sequencing;
- specialist radiology review.
For patients, this could mean fewer missed diagnoses, shorter diagnostic delays and more personalised treatment.
5. Community and digital care could help patients
The report supports moving appropriate care closer to home, using outpatient antimicrobial therapy, virtual services and digitally enabled community pathways.
For people with aspergillosis, this could be very beneficial. Many patients have long-term breathlessness, fatigue and mobility limitations, and may live far from specialist centres.
Potential benefits include:
- fewer long-distance hospital visits;
- remote monitoring of symptoms and test results;
- shared-care arrangements with local hospitals;
- virtual multidisciplinary team review;
- faster specialist advice for local clinicians.
However, fungal disease management is complex. Community pathways must still include specialist oversight because antifungal treatment can involve drug interactions, liver toxicity, therapeutic drug monitoring, adrenal suppression and resistance issues.
6. Antifungal stewardship should become more prominent
The report focuses heavily on antimicrobial stewardship. Although much of this is framed around antibiotics, the same principles apply to antifungal medicines.
For aspergillosis care, antifungal stewardship means using the right antifungal, at the right dose, for the right duration, with careful monitoring.
This is especially important because of:
- azole resistance in Aspergillus fumigatus;
- long courses of antifungal treatment;
- drug interactions with steroids, anticoagulants, immunosuppressants and other medicines;
- the need for therapeutic drug monitoring;
- side effects affecting the liver, skin, nerves or adrenal system.
For patients, better antifungal stewardship should mean safer and more effective treatment.
7. Fungal disease has a role in pandemic preparedness
The report includes mycology within pandemic preparedness planning. This is important because fungal complications can emerge during major respiratory outbreaks.
COVID-associated pulmonary aspergillosis (CAPA) showed that fungal disease can become highly relevant during pandemics, especially in intensive care and immunocompromised patients.
Future preparedness should therefore include fungal diagnostics, fungal surveillance, resistance monitoring and specialist mycology input.
8. Workforce expansion is essential
The report warns that the infection-specialist workforce is under pressure. This is particularly important for fungal disease because the UK has a limited number of specialist medical mycologists, fungal pharmacists, laboratory scientists and specialist nurses.
For aspergillosis services, workforce planning should include:
- more medical mycology training opportunities;
- more specialist fungal pharmacists;
- more fungal diagnostics scientists;
- more specialist nurses supporting long-term fungal disease care;
- protected time for multidisciplinary team meetings and advice services.
Without this, diagnostic delays and unequal access to specialist care may persist.
9. What this means for patients
For patients, the report supports several important messages:
- fungal disease expertise matters;
- specialist diagnosis and treatment are important;
- long-term fungal lung disease requires joined-up care;
- access to expert advice should not depend too heavily on postcode;
- digital and shared-care systems could reduce the need for repeated travel;
- patient education should be part of infection service planning.
The report may also be useful for patient advocacy because it provides national-level support for strengthening infection services, including fungal infection expertise.
10. What is still missing?
Although the report is very helpful, aspergillosis itself is not discussed in detail. Areas that would benefit from stronger future emphasis include:
- chronic pulmonary aspergillosis (CPA);
- allergic bronchopulmonary aspergillosis (ABPA);
- severe asthma with fungal sensitisation (SAFS);
- Aspergillus bronchitis;
- azole-resistant Aspergillus;
- environmental mould exposure and health;
- long-term patient support and rehabilitation.
This creates an opportunity for aspergillosis specialists, patient groups and charities to build on the report and make the case for more visible fungal disease planning.
Conclusion
This report is a positive development for aspergillosis. It recognises that fungal disease expertise is part of the UK’s essential infection workforce and supports many of the changes aspergillosis patients need: better diagnostics, stronger specialist networks, digital care, community support, workforce expansion and safer antimicrobial use.
The key challenge is ensuring that fungal disease does not remain only briefly mentioned within broader infection policy. Aspergillosis specialists and patient advocates can use this report to argue that fungal infection services need sustained investment, national planning and equitable access across the UK.
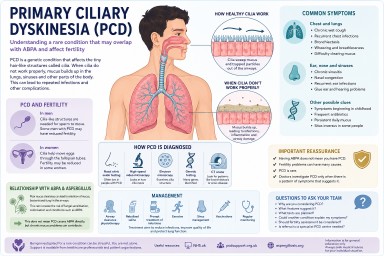
Primary Ciliary Dyskinesia (PCD), Fertility and Aspergillosis
Understanding a rare condition that may overlap with ABPA and bronchiectasis
People living with chronic lung conditions such as asthma, bronchiectasis or ABPA (Allergic Bronchopulmonary Aspergillosis) are sometimes investigated for other underlying conditions that may help explain repeated chest infections, mucus problems or long-term lung damage. One of the rarer conditions doctors may consider is Primary Ciliary Dyskinesia (PCD).
For some patients, hearing PCD mentioned for the first time can raise many questions — especially if fertility problems are also being discussed. This article explains what PCD is, how it may relate to lung disease and Aspergillus problems, and why it can sometimes affect fertility.
Key points
- Primary Ciliary Dyskinesia (PCD) is a rare inherited condition affecting the body's mucus-clearing system.
- It can cause recurrent chest infections, sinus problems and bronchiectasis.
- Some people with PCD may also develop fungal sensitisation or ABPA.
- Men with PCD may experience reduced fertility because sperm movement can be affected.
- PCD is often difficult to diagnose because symptoms overlap with asthma and bronchiectasis.
- Specialist testing is usually needed for diagnosis.
- Having ABPA does not automatically mean someone has PCD.
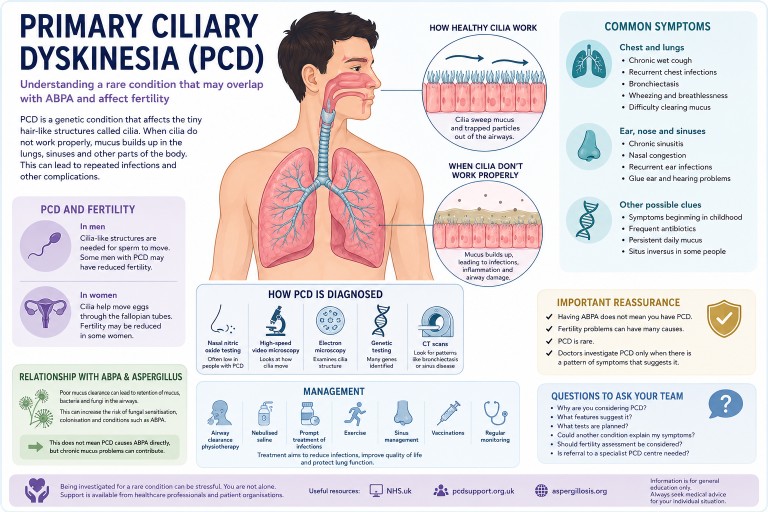
What is Primary Ciliary Dyskinesia?
Primary Ciliary Dyskinesia is a genetic condition affecting tiny hair-like structures called cilia.
These microscopic structures line parts of the body including the airways, sinuses, ears and reproductive tract. Their role is to move mucus, bacteria, dust and debris out of the lungs and airways.
In PCD, the cilia may not move properly, may move in an uncoordinated way, or may sometimes be absent altogether. As a result, mucus clearance becomes much less effective.
Why mucus clearance matters
Healthy lungs constantly produce mucus to trap particles and germs. Normally, cilia sweep this mucus upwards so it can be coughed out or swallowed.
When the system does not work properly, mucus becomes harder to clear. Bacteria and fungi may remain in the lungs for longer, repeated infections may occur, inflammation can develop, and long-term airway damage may gradually appear.
Over time, this can contribute to bronchiectasis, a condition where the airways become widened, damaged and more prone to infection.
Symptoms of PCD
Symptoms vary between individuals, but may include:
Chest and lung symptoms
- Chronic wet or productive cough
- Recurrent chest infections
- Bronchiectasis
- Wheezing
- Breathlessness
- Difficulty clearing mucus
Ear, nose and sinus symptoms
- Chronic sinusitis
- Nasal congestion
- Glue ear
- Recurrent ear infections
- Hearing problems
Other possible clues
- Symptoms beginning in childhood
- Frequent courses of antibiotics
- Persistent daily mucus production
- Situs inversus, where some internal organs are positioned differently, in some people
Not everyone with PCD has all these symptoms.
How could PCD relate to ABPA or Aspergillus?
ABPA (Allergic Bronchopulmonary Aspergillosis) develops when the immune system reacts strongly to the fungus Aspergillus fumigatus, which is common in the environment.
People with impaired mucus clearance may retain mucus for longer, have more airway inflammation, develop bronchiectasis, and potentially allow bacteria or fungi to persist more easily in the airways.
This does not mean PCD directly causes ABPA. However, chronic mucus retention and airway damage can create conditions where fungal sensitisation, colonisation or allergic responses may become more likely.
Some people investigated for difficult-to-control asthma, bronchiectasis or recurrent infections may therefore be assessed for underlying conditions such as PCD, cystic fibrosis, immune deficiency or other rare mucus-clearance disorders.
PCD and fertility
One reason PCD can be emotionally difficult to process is that it may affect fertility.
In men
Sperm movement relies on structures very similar to cilia. In some men with PCD, sperm may not move effectively, fertility may be reduced, or natural conception may become more difficult.
This does not necessarily mean infertility is absolute. Some men with PCD can still father children naturally, while others may benefit from fertility support or assisted reproductive techniques.
In women
Some women with PCD may also experience reduced fertility because cilia help move eggs through the fallopian tubes, although effects are often less severe and more variable than in men.
How is PCD diagnosed?
Diagnosing PCD can be challenging because symptoms overlap with many other respiratory conditions. Patients are often referred to specialist centres for assessment.
Testing may include:
- Nasal nitric oxide testing: people with PCD often have unusually low levels of nasal nitric oxide.
- High-speed video microscopy: this examines how cilia move under a microscope.
- Electron microscopy: this examines ciliary structure in detail.
- Genetic testing: many genes linked to PCD have now been identified.
- CT scans: doctors may look for patterns such as bronchiectasis or chronic sinus disease.
Sometimes diagnosis takes months or even years, particularly in adults whose symptoms have previously been attributed to asthma, infections or bronchiectasis alone.
Why diagnosis can be delayed
PCD is rare and its symptoms can resemble asthma, recurrent viral infections, chronic sinusitis, Chronic Obstructive Pulmonary Disease (COPD), bronchiectasis or “just bad lungs”.
Many adults diagnosed later in life report years of unexplained chest symptoms before PCD was considered.
Treatment and management
There is currently no cure for PCD itself, but treatment focuses on reducing lung damage and improving mucus clearance.
Management may include:
- Airway clearance physiotherapy
- Nebulised saline
- Prompt treatment of infections
- Exercise
- Sinus management
- Vaccinations
- Monitoring for bronchiectasis
Some patients may also require management of associated conditions such as asthma, bronchiectasis or ABPA.
Emotional impact
Being investigated for a rare condition can feel overwhelming, especially when fertility concerns are raised unexpectedly.
People may feel uncertainty, anxiety about future health, frustration over delayed diagnosis, or concern about relationships and starting a family. These reactions are understandable.
It can help to discuss concerns with respiratory specialists, fertility specialists, physiotherapists and trusted patient support organisations.
Important reassurance
- Having ABPA does not mean you have PCD.
- Fertility problems can have many different causes.
- PCD remains a relatively rare condition.
- Doctors usually investigate PCD only when a pattern of symptoms suggests it may be relevant.
Mentioning PCD as a possibility is often part of carefully exploring all possible explanations for long-term respiratory symptoms.
Questions you may wish to ask your medical team
- Why are you considering PCD?
- What features suggest it?
- What tests are planned?
- Could another condition explain my symptoms?
- Should fertility assessment be considered?
- Is referral to a specialist PCD centre needed?
When to seek medical advice
You should seek medical advice if you experience worsening breathlessness, coughing up blood, severe chest infections, unexplained weight loss, persistent fevers, or rapidly worsening mucus production.
Fertility concerns can also be discussed with your GP, respiratory specialist or fertility specialist.
Further information
References
- Lung + Asthma PCD
- PCD Support UK.
- European Respiratory Society guidelines for the diagnosis of Primary Ciliary Dyskinesia.
- NHS England. National Primary Ciliary Dyskinesia Service.
Last reviewed: May 2026
This article is for general educational purposes only and is not a substitute for personalised medical advice.
Why Antifungal Drug Interactions Matter — and How AntifungalInteractions.org Can Help
Key points
- Antifungal medicines used in aspergillosis can interact with many common medicines and supplements.
- Some interactions are mild, while others can significantly affect drug levels or side effects.
- Interactions may involve steroids, inhalers, antibiotics, heart medicines, acid suppressants and herbal supplements.
- Patients should always tell healthcare teams about all medicines, vitamins and supplements they take.
- AntifungalInteractions.org is a specialist resource designed to help healthcare professionals and patients understand potential antifungal interactions.
Why do antifungal interactions matter so much?
The antifungal medicines used to treat aspergillosis are powerful and highly specialised drugs. They are extremely important in controlling fungal disease, but many also affect the way the body processes other medicines.
This is particularly true for azole antifungals such as:
- itraconazole,
- voriconazole,
- posaconazole,
- isavuconazole.
These medicines are processed through enzyme systems in the liver, especially the cytochrome P450 system. Unfortunately, many other medicines also use these same pathways.
This means antifungals can sometimes:
- increase levels of other medicines,
- reduce levels of other medicines,
- increase side effects,
- affect liver function,
- change how well treatments work.
Because aspergillosis patients often take several medicines at the same time, interactions become particularly important.
Common medicines that may interact with antifungals
Not every interaction is dangerous, and many medicines can still be used safely with careful monitoring. However, some combinations require dose adjustments or additional caution.
Steroids and inhalers
Many patients with allergic bronchopulmonary aspergillosis (ABPA), severe asthma or bronchiectasis take steroid medicines.
Interactions can occur with:
- prednisolone,
- methylprednisolone,
- inhaled steroids such as fluticasone or budesonide.
Azole antifungals can increase steroid exposure, potentially increasing the risk of side effects such as:
- weight gain,
- skin thinning,
- high blood sugar,
- adrenal suppression,
- mood changes.
Heart medicines
Some antifungals can affect heart rhythm or interact with medicines used for:
- high blood pressure,
- irregular heartbeat,
- blood thinning,
- cholesterol management.
This is one reason doctors and pharmacists carefully review medication lists before starting antifungal treatment.
Acid suppressants
Medicines used for acid reflux or stomach protection may affect how well some antifungals are absorbed.
This includes:
- omeprazole,
- lansoprazole,
- esomeprazole,
- antacid preparations.
In some cases, antifungal levels may become too low to work effectively.
Antibiotics and other anti-infective medicines
Some antibiotics and antifungals can interact in ways that increase side effects or affect the electrical activity of the heart.
This is particularly important in people already taking multiple medicines.
Supplements and herbal remedies
Patients are often surprised that supplements may also interact with antifungals.
Potential concerns include:
- CBD oil or cannabis products,
- St John’s Wort,
- high-dose vitamins,
- herbal sleep remedies,
- sports supplements.
“Natural” products can still affect liver enzyme systems and may alter medicine levels.
What is AntifungalInteractions.org?
AntifungalInteractions.org is a specialist online interaction checker designed specifically for antifungal medicines.
The site was developed to help healthcare professionals identify and manage potential interactions involving antifungal drugs.
It is widely used internationally and is regularly updated by specialist pharmacy experts.
Why is it useful?
General drug references do not always provide detailed fungal-specific interaction guidance.
AntifungalInteractions.org focuses specifically on antifungal medicines and often provides:
- more detailed interaction information,
- clearer explanations of risks,
- practical management advice,
- colour-coded interaction severity ratings.
This can help patients better understand why clinicians sometimes adjust medicines, order blood tests or recommend monitoring.
Can patients use the website themselves?
Yes — many patients find it useful for understanding their treatment better.
However, it is important not to interpret interaction checkers without context.
An interaction warning does not automatically mean:
- a medicine combination is unsafe,
- treatment must stop,
- harm will definitely occur.
Many interactions can be safely managed by:
- dose adjustments,
- blood test monitoring,
- timing changes,
- careful clinical supervision.
What should patients do?
Patients should try to keep an up-to-date list of:
- prescription medicines,
- inhalers,
- vitamins,
- supplements,
- CBD or cannabis products,
- over-the-counter medicines.
It is particularly important to mention supplements or herbal remedies because these are easily overlooked during clinic visits.
Do not stop medicines without advice
One of the most important messages is that patients should not stop antifungal medicines or other prescribed treatments based only on an online interaction checker.
Antifungal treatment decisions are often carefully balanced against:
- severity of fungal disease,
- lung function,
- other illnesses,
- alternative treatment options.
Healthcare teams can often safely manage interactions once they are aware of them.
The bottom line
Drug interactions are an important part of antifungal treatment, particularly for people living with aspergillosis who may already take several medicines.
AntifungalInteractions.org is an excellent specialist resource that can help patients and healthcare professionals better understand these interactions.
However, online interaction checkers should support discussions with healthcare professionals rather than replace them.
Useful link
Visit AntifungalInteractions.org
BNF to check any other medication interactions
Author and review information
Prepared as general educational information for people affected by aspergillosis and related lung conditions.
This article does not replace personalised medical advice.
Last reviewed: May 2026
CBD Oil, Cannabis and Aspergillosis: Safety, Quality and Drug Interactions
Key points
- Some people with chronic illnesses report that CBD or cannabis products help with pain, anxiety, sleep or wellbeing.
- Evidence for benefit in aspergillosis itself remains limited.
- Smoking or vaping cannabis may irritate the lungs and may not be suitable for people with respiratory disease.
- CBD and cannabis products can interact with antifungal medicines and steroids.
- Product quality varies greatly, especially with over-the-counter or online products.
- Always let your healthcare team or pharmacist know about any CBD or cannabis products you are using.
Why this topic comes up
People living with aspergillosis often cope with long-term symptoms such as fatigue, chronic cough, breathlessness, pain or chest discomfort, anxiety, poor sleep, steroid side effects and reduced quality of life.
Because of this, discussions about CBD oil, cannabis or “medical marijuana” occasionally appear in patient groups and online communities. Some people report that these products help them cope better with symptoms or improve sleep and wellbeing.
At the same time, there are important safety issues that people with respiratory fungal disease should be aware of, particularly around lung irritation, product quality and drug interactions.
CBD and cannabis are not the same thing
CBD: cannabidiol
CBD, or cannabidiol, is one of the compounds found in cannabis plants. CBD products usually contain little or no THC, or tetrahydrocannabinol, the chemical responsible for the “high” associated with cannabis.
CBD products may be sold as oils, capsules, gummies, creams, drinks or food supplements. CBD is generally less intoxicating than THC-containing cannabis products.
Cannabis or marijuana
Cannabis products may contain varying amounts of THC. THC is more strongly associated with intoxication, impaired concentration, sedation, anxiety or panic, hallucinations or paranoia in some people, and impaired driving or coordination.
Different cannabis products can vary enormously in strength and purity.
What conditions have good evidence for medical cannabis?
Cannabis-based medicines are prescribed in some situations where evidence is reasonably strong.
In the UK, prescription cannabinoid medicines are mainly used for certain severe forms of epilepsy, chemotherapy-related nausea and vomiting, and muscle spasticity in multiple sclerosis. There is also ongoing research into chronic pain and palliative care use.
However, evidence for benefit in aspergillosis, bronchiectasis, asthma, allergic bronchopulmonary aspergillosis (ABPA) or chronic pulmonary aspergillosis (CPA) remains limited.
This does not mean that people never feel benefit. Some clearly do. But respiratory fungal disease is not currently one of the better-established medical indications.
Lung safety concerns in aspergillosis
This is probably the most important issue for many aspergillosis patients.
Smoking cannabis
Smoking any substance exposes the lungs to heat, particulates, irritants and combustion products.
For people who already have asthma, bronchiectasis, chronic lung infection, airway inflammation or fungal lung disease, this may worsen symptoms such as coughing, wheezing, chest tightness, mucus production or breathlessness.
Vaping
Some people assume vaping is automatically safer than smoking, but this is not always true.
Vaping can still irritate the airways and lungs, and the long-term effects are not fully understood. For people with fragile or inflamed lungs, clinicians are often cautious about recommending inhaled cannabis products of any kind.
Contamination and quality problems
One important issue is that cannabis and CBD products are not all produced to the same standards.
Product quality can vary greatly
Some products may contain more or less CBD or THC than stated, contain contaminants, contain pesticides or solvents, or vary significantly between batches.
This is especially true for unregulated products purchased online or from unofficial sources.
Mould contamination
Cannabis products can occasionally become contaminated with moulds, including Aspergillus species.
This is particularly concerning for immunocompromised patients, transplant patients, people on long-term steroids, and people with chronic lung disease.
Although this appears uncommon, it is one reason respiratory specialists are often cautious about smoked cannabis products in fungal disease patients.
Drug interactions: a very important issue
Many antifungal medicines are processed through liver enzyme systems that can also be affected by CBD or cannabis compounds. This means interactions are possible.
Antifungal medicines of concern
Potential interactions may occur with antifungals such as:
- itraconazole
- voriconazole
- posaconazole
- isavuconazole
These medicines already require careful monitoring because blood levels can vary significantly between people.
Adding CBD or cannabis products may potentially alter antifungal levels, liver metabolism or side-effect risks.
Steroids and other medicines
Interactions may also occur with prednisolone, methylprednisolone, opioid pain medicines, sleeping tablets, antidepressants and anti-anxiety medicines.
Possible effects may include increased sedation, dizziness, falls, confusion, liver irritation or worsening side effects.
This does not automatically mean the products are unsafe, but it does mean healthcare teams should know about them.
“Natural” does not always mean low risk
Many patients understandably assume that CBD products are “gentle” or “natural.”
However, natural products can still interact with prescription medicines, doses may be inconsistent, some products are poorly regulated, and side effects can still occur.
This is especially important in aspergillosis because patients are often already taking multiple medicines, including antifungals and steroids.
Why patients may still be interested
Despite the uncertainties, it is understandable why some patients explore these products.
People sometimes report improvement in sleep, anxiety, pain, appetite, overall wellbeing or coping with chronic illness. These experiences are real and important to acknowledge respectfully.
At present, however, there is still limited high-quality research specifically in aspergillosis and chronic fungal lung disease.
Practical safety advice
If someone chooses to use CBD or cannabis products, it is sensible to:
- tell their healthcare team or pharmacist,
- mention all supplements and oils being used,
- watch for new side effects after starting,
- avoid assuming “natural” means risk-free,
- be especially cautious with smoked or inhaled products,
- avoid driving or hazardous activities if feeling impaired.
When to seek medical advice
Medical review is important if new symptoms appear after starting CBD or cannabis products, especially:
- worsening breathlessness,
- severe drowsiness,
- confusion,
- hallucinations,
- jaundice,
- severe dizziness,
- palpitations,
- fever or worsening chest symptoms.
The bottom line
CBD and cannabis products are becoming more widely discussed in chronic illness communities, including among people with aspergillosis.
Some people report benefits for sleep, anxiety or quality of life, and there are a small number of medical conditions where prescription cannabis-based medicines are supported by stronger evidence.
However, for aspergillosis patients, important concerns remain around lung irritation, mould contamination, product quality, and interactions with antifungal medicines and steroids.
Because of this, healthcare teams are usually cautious and prefer open discussion rather than patients using these products without medical awareness.
Further information
- NHS guidance on medical cannabis
- Specialist pharmacist advice on antifungal interactions
- Specialist pharmacist advice on steroid interactions
- National Aspergillosis Centre resources on antifungal medicines
Author and review information
Prepared for aspergillosis patients and carers as general educational information. This article is not intended to replace personalised medical advice.
Last reviewed: May 2026

Weekly Aspergillosis Research Update 18th May 2026
This update is written for patients, carers and non-specialists. It is not medical advice, but it may help explain why specialist assessment, careful monitoring and joined-up care are so important in aspergillosis.
Key points
- Aspergillosis is not one single illness. It includes allergic, chronic and invasive forms, each needing different assessment and treatment.
- Several recent papers show that Aspergillus disease often develops where the lungs are already vulnerable, damaged or scarred.
- Invasive aspergillosis remains mainly a concern for people who are severely unwell or immunocompromised.
- Antifungal resistance, drug interactions and access to specialist fungal diagnostics continue to be important themes.
- Some papers describe unusual or experimental approaches, but these should not be seen as standard treatment unless recommended by a specialist team.
1. Aspergillosis can develop in already damaged lungs
One recent case report described chronic pulmonary aspergillosis complicated by a bacterial lung abscess inside a lung cavity. The patient was successfully treated with percutaneous drainage, where fluid or infected material is drained through the skin using imaging guidance, alongside medical care.
Another recent paper examined aspergillosis complicating idiopathic pulmonary fibrosis. Idiopathic pulmonary fibrosis is a serious lung-scarring condition. This paper is important because fungal infection in people with fibrotic lung disease remains relatively understudied.
A separate review on the gut-lung axis in people with cystic fibrosis on CFTR modulators also reflects the growing interest in how long-term lung disease, airway microbes, inflammation and wider body systems interact. This is not only about Aspergillus, but it is relevant to understanding why airway infections and immune responses can vary between patients.
Why this matters: Aspergillus can sometimes take advantage of areas of lung that are already damaged by previous infection, cavities, scarring, bronchiectasis, chronic obstructive pulmonary disease, tuberculosis, cystic fibrosis, fibrosis or other long-term lung conditions. This does not mean everyone with lung damage will develop aspergillosis, but it does explain why doctors may investigate new or worsening symptoms carefully.
2. Nutritional health and immune resilience
A paper on aspergillosis in anorexia nervosa reported two cases and reviewed previous published cases. Severe malnutrition can affect the immune system, making some infections more likely or harder to recover from.
Why this matters: nutrition is part of immune resilience. This does not mean that poor diet directly causes aspergillosis, but severe undernutrition may reduce the body’s ability to respond to infection. For patients living with chronic illness, maintaining nutrition, weight and muscle strength can be an important part of overall care.
3. Invasive aspergillosis remains a serious infection in high-risk groups
Several papers this week focused on invasive aspergillosis. These included a 12-year retrospective cohort study of invasive aspergillosis in children, a review of invasive mould infections in children, and a case report of pulmonary aspergillosis following severe fever with thrombocytopenia syndrome.
Other papers reported invasive Aspergillus disease in very specific high-risk settings, including extensive facial tissue necrosis after paediatric peripheral blood stem cell transplantation and a Chinese-language report on bronchoscopic interventional therapy for invasive pulmonary aspergillosis.
Why this matters: invasive aspergillosis is different from allergic bronchopulmonary aspergillosis and chronic pulmonary aspergillosis. It usually occurs in people who are severely unwell or whose immune system is significantly weakened. It is a medical emergency and requires urgent specialist care.
For patients and families, it is useful to understand that the word aspergillosis covers several different diseases. The outlook, urgency and treatment plan can be very different depending on which form is present.
4. Better diagnosis depends on awareness and laboratory capacity
A French multicentre survey looked at laboratory capacity for diagnosing fungal infections. This type of research is important because diagnosis does not depend only on the doctor thinking of fungal disease. It also depends on access to the right laboratory tests, fungal culture, antigen testing, molecular testing, susceptibility testing and specialist interpretation.
Another paper on primary ciliary dyskinesia in children included aspergillosis among the infections and differential diagnoses clinicians may need to consider when assessing complex chronic respiratory symptoms. Although this was not primarily an aspergillosis paper, it reinforces the wider point that fungal disease can be part of a broader diagnostic picture in patients with long-term airway problems.
Why this matters: delays in diagnosing aspergillosis are common. Improving diagnosis means improving the whole pathway: clinical awareness, access to tests, expert laboratories and specialist teams who can interpret complex results.
5. Antifungal resistance remains an important issue
A review on a One Health approach to antifungal resistance in allergic bronchopulmonary aspergillosis highlighted the wider problem of antifungal resistance. A One Health approach recognises that human health, animal health and the environment are connected.
Aspergillus species live widely in the environment. Resistance may emerge not only through medical antifungal use, but also through environmental exposure to antifungal compounds used in agriculture or other settings.
Why this matters: antifungal resistance can make treatment more difficult. This is one reason why specialist teams may request fungal cultures, susceptibility testing, antifungal drug-level monitoring or treatment changes. It is also why antifungals should be used carefully and monitored properly.
6. Drug interactions are a practical safety issue
One paper examined possible drug interactions between midostaurin and posaconazole in people with a type of acute myeloid leukaemia. Although this is a specialist cancer-treatment paper, it illustrates a wider issue that is relevant to many patients taking antifungal medicines.
Azole antifungals such as itraconazole, voriconazole, posaconazole and isavuconazole can interact with other medicines. These interactions may affect antifungal levels, side effects or the levels of other medicines.
Why this matters: patients taking antifungals should tell their doctor and pharmacist about all prescribed medicines, over-the-counter medicines, inhalers, herbal products and supplements. Monitoring is part of safe antifungal treatment.
7. New or alternative antifungal approaches are being explored
One case report described pulmonary aspergillosis treated with oral amphotericin B, known as MAT2203, in a patient with human immunodeficiency virus-related cryptococcal meningitis. This is interesting because amphotericin B is usually given intravenously, and oral formulations are being explored for specific situations.
A Scite literature check also highlighted recent specialist papers on endoscopic liposomal amphotericin B therapy in semi-invasive pulmonary aspergillosis and newer antifungal approaches such as manogepix. These were not central to the PubMed list used for this update, but they support the wider message that antifungal research is active.
Why this matters: research into new ways of treating Aspergillus infection is active. This is encouraging, especially for difficult cases where standard antifungal treatment is limited by resistance, side effects or interactions. However, case reports and early-stage studies should not be seen as proof that a treatment is ready for routine use.
8. Allergic bronchopulmonary aspergillosis guidance continues to evolve
A Chinese-language expert consensus paper considered the diagnosis and treatment of allergic bronchopulmonary aspergillosis with integrated traditional Chinese and western medicine. This is not directly applicable to UK practice, but it reflects the continued international interest in improving diagnosis and management of allergic bronchopulmonary aspergillosis.
Why this matters: allergic bronchopulmonary aspergillosis can be difficult to diagnose because it overlaps with asthma, bronchiectasis, mucus plugging, raised immunoglobulin E and eosinophilic inflammation. Different countries and specialist groups continue to refine how they classify and manage the condition.
9. Laboratory science continues to improve understanding of Aspergillus
One paper investigated Aspergillus fumigatus morphogenesis and pathogenesis through a putative lipid transporter called ArvA. This is laboratory-based science rather than an immediate patient-care paper.
Why this matters: basic science helps researchers understand how Aspergillus grows, adapts and interacts with the immune system. Over time, this type of work may help identify new treatment targets or explain why some infections behave differently from others.
10. A note of caution about non-standard treatments
One paper reported follow-up of a previous aspergillosis case treated with oxygen-ozone therapy. This should be interpreted very cautiously. Pulmonary aspergillosis usually requires specialist assessment and, when treatment is needed, evidence-based antifungal therapy and monitoring.
Important: patients should not stop prescribed antifungal treatment or replace it with non-standard approaches without discussion with their specialist clinical team.
What this means for patients
This week’s research shows again that aspergillosis is complex. It can be allergic, chronic or invasive. It can affect people with asthma, cystic fibrosis, damaged lungs, weakened immune systems or severe underlying illness. It may require imaging, blood tests, sputum tests, bronchoscopy, antifungal drug monitoring and careful review by experienced clinicians.
The most useful message for patients is that persistent or worsening symptoms should be taken seriously, especially in people with known lung disease or immune problems. Good communication with healthcare teams, careful monitoring and specialist fungal expertise remain central to safe care.
When to seek medical advice
People living with aspergillosis or long-term lung disease should seek medical advice if they notice:
- new or worsening breathlessness
- coughing up blood
- persistent fever or night sweats
- unexplained weight loss
- worsening fatigue or weakness
- new chest pain
- symptoms that are not improving despite treatment
- possible side effects from antifungal medicines
Urgent medical help is needed for severe breathlessness, significant coughing up of blood, confusion, collapse, severe chest pain or rapidly worsening symptoms.
References and papers included in this update
- Okazaki Y, Shirata M, Koma K, et al. Chronic pulmonary aspergillosis complicated by a lung abscess within a pulmonary cavity successfully treated with percutaneous drainage: A case report.
Internal Medicine. 2026. - Mercier A, Loridant S, Tetart M, et al. Aspergillosis in anorexia nervosa: a report of two cases and review of the literature.
BMC Infectious Diseases. 2026. - Gutierrez-Perez C, Jones JT, Puerner CTS, et al. Insights into Aspergillus fumigatus morphogenesis and pathogenesis through the putative lipid transporter ArvA.
mSphere. 2026. - Greydanus DE, Bhave SY, Ashok N, Goel A. Primary ciliary dyskinesia in pediatric persons: A microscopic movement malady.
Disease-a-Month. 2026. - Lai X, Gao Q, Wu L. A 56-Year-Old Male Farmer From China With Severe Fever With Thrombocytopenia Syndrome and Pulmonary Aspergillosis: A Case Report and Review of Literature.
American Journal of Case Reports. 2026. - Morio F, Alanio A, Boukris-Sitbon K, et al. Assessing Laboratory Capacity for Diagnosis of Fungal Infections in France: A Multicentre survey within the SINFONI Network.
Medical Mycology. 2026. - Falcon RMG, Asedillo KFY, Gilo AJG, et al. One health approach to management of antifungal resistance in allergic bronchopulmonary aspergillosis.
Molecular Biology Reports. 2026. - Kagimu E, Senkoro E, Gakuru J, et al. Pulmonary Aspergillosis Treated With Oral Amphotericin B (MAT2203) in a Patient With HIV-Related Cryptococcal Meningitis.
Clinical Case Reports. 2026. - Lefranc M, Ramel E, Marsh R, et al. Towards a gut-lung axis role in pwCF on CFTR modulators: rationale, clinical evidence and perspectives.
Journal of Cystic Fibrosis. 2026. - Bermudez J, Debray MP, Uzunhan Y, et al. Aspergillosis complicating idiopathic lung fibrosis: a multicentric series.
Respiratory Medicine. 2026. - Franzini M, Valdenassi L, Chirumbolo S. Follow up of a previous aspergillosis case report treated with oxygen-ozone therapy, reporting clinical remission of the lung fungal infection.
International Immunopharmacology. 2026. - Karaman A, Cengiz AB, Aykac K, et al. Evaluation of the Clinical Characteristics and Survival of Pediatric Patients with Invasive Aspergillosis: A 12-year Retrospective Cohort Study.
Mycopathologia. 2026. - Joisten CS, Mellinghoff SC, Seidel D, et al. Clinical impact of potential drug-drug interactions between midostaurin and posaconazole in FLT3-mutated AML.
Antimicrobial Agents and Chemotherapy. 2026. - Lim H, Kim MW, Lee JW. Delayed Anterolateral Thigh Free Flap Reconstruction for Extensive Buccal-Midfacial Necrosis Caused by Invasive Aspergillosis After Pediatric PBSCT: A 7-Year Follow-Up.
Journal of Craniofacial Surgery. 2026. - Warris A, Rojo P, Groll AH, Arrieta AC. Invasive mold infections in the pediatric setting: current status and new developments.
Expert Review of Anti-Infective Therapy. 2026. - Li J, Cai CL, Zhao LN, Wang YH, Mu XD. Clinical analysis of comprehensive bronchoscopic interventional therapy for invasive pulmonary aspergillosis.
Zhonghua Jie He He Hu Xi Za Zhi. 2026. - Allergy Committee of Chinese Association of Integrative Medicine. Expert consensus on the diagnosis and treatment of allergic bronchopulmonary aspergillosis with integrated traditional Chinese and western medicine: 2026 edition.
Zhonghua Yi Xue Za Zhi. 2026.
Editor’s note
This article is based mainly on a PubMed search for recent aspergillosis papers. Each reference links to its PubMed record where readers can view the abstract, journal details and, where available, links to free full text. A brief Scite search was also used to identify related recent papers and research themes, but the main patient-facing interpretation has been written from the PubMed results listed above.
Last reviewed: May 2026

Aspergillosis Trust: Supporting People Affected by Aspergillosis

Raising Awareness of Aspergillosis
One of the Trust’s most important roles is increasing awareness of aspergillosis among:
- Patients and carers
- Healthcare professionals
- Researchers
- Policy makers
- The wider public
This includes helping people better understand conditions such as:
- ABPA (Allergic Bronchopulmonary Aspergillosis)
- CPA (Chronic Pulmonary Aspergillosis)
- Aspergilloma
- Invasive aspergillosis
- Severe asthma with fungal sensitisation (SAFS)
By promoting education and awareness, the Trust helps support earlier recognition and diagnosis of fungal disease.
Patient Support and Community
Living with aspergillosis can be physically and emotionally challenging. Many patients experience fatigue, breathlessness, anxiety, long treatment journeys and uncertainty about the future.
The Aspergillosis Trust helps provide:
- Patient-focused information
- Community support
- Awareness campaigns
- Educational events
- Opportunities for patient involvement
The charity also helps patients connect with others who understand the realities of living with chronic fungal disease, reducing feelings of isolation and helping people feel supported.
Supporting Research and Advocacy
The Trust actively supports research into aspergillosis and fungal disease, while also advocating for better services and greater recognition of fungal infections within healthcare systems.
This includes:
- Supporting patient participation in research
- Raising awareness of diagnostic delays
- Promoting better understanding of chronic fungal disease
- Working alongside clinicians, researchers and respiratory organisations
- Supporting international awareness activities
The organisation has collaborated with specialist centres, patient groups and international respiratory organisations to strengthen awareness and improve education around aspergillosis.
Working Together with the Wider Respiratory Community
The Aspergillosis Trust is part of a growing international effort to improve fungal disease awareness and patient support.
This includes collaboration and engagement with organisations such as:
- European Lung Foundation (ELF)
- European Respiratory Society (ERS)
- Specialist respiratory and infectious disease centres
- Patient advocacy organisations
- Researchers working in fungal disease and respiratory medicine
These partnerships help ensure that the experiences of people living with aspergillosis are represented within wider respiratory healthcare discussions.
Differences Between the Aspergillosis Trust and National Aspergillosis Centre Patient Support
The Aspergillosis Trust and the National Aspergillosis Centre (NAC) both play extremely important roles in supporting people affected by aspergillosis, but they are different types of organisations with different responsibilities and strengths. In many ways, they complement one another.
The National Aspergillosis Centre (NAC)
The National Aspergillosis Centre is an NHS Highly Specialised Service based at Wythenshawe Hospital in Manchester. It is a specialist clinical centre commissioned to diagnose, treat and manage complex aspergillosis cases — particularly Chronic Pulmonary Aspergillosis (CPA).
The NAC provides:
- Specialist medical diagnosis and treatment
- Advice and Guidance to clinicians across the UK
- Monitoring of antifungal therapy
- Clinical investigations and testing
- Research programmes
- Patient education resources
- NHS-supported patient support meetings and moderated support groups
The NAC CARES team (Community, Awareness, Research, Education and Support) runs:
- The patient information website aspergillosis.org
- Weekly Microsoft Teams meetings
- Educational webinars
- Facebook and online support communities
- Research participation activities
- World Aspergillosis Day educational events
Because the NAC is part of the NHS, its information tends to be strongly clinically focused and evidence-based, with close involvement from specialist doctors, nurses, pharmacists and researchers.
The Aspergillosis Trust
The Aspergillosis Trust is a patient-led charity rather than a clinical NHS service. It was created by patients and carers affected by aspergillosis to improve awareness, advocacy and community support.
The Trust focuses particularly on:
- Raising public and professional awareness
- Patient advocacy
- Representing the patient voice
- Community support
- Campaigning for earlier diagnosis and better recognition
- Helping reduce isolation among patients and carers
Because it is patient-led, the Trust brings a particularly strong lived-experience perspective. Many people find this valuable because the charity is run by people who directly understand the emotional, practical and social impact of living with aspergillosis.
A Simple Way to Think About the Difference
| NAC Patient Support | Aspergillosis Trust |
|---|---|
| NHS specialist clinical service | Independent patient charity |
| Led by healthcare professionals and NHS staff | Led by patients and carers |
| Focus on diagnosis, treatment, education and research | Focus on advocacy, awareness and peer support |
| Provides specialist clinical expertise | Provides lived-experience support |
| Closely linked to NHS care pathways | Represents the broader patient community |
| Produces medically reviewed educational resources | Amplifies the patient voice and patient needs |
How They Work Together
Importantly, these organisations are not competitors. They often collaborate closely on awareness campaigns, patient education, World Aspergillosis Day activities, webinars, conferences and research engagement.
Many patients benefit from engaging with both:
- The NAC for specialist medical expertise and educational resources
- The Aspergillosis Trust for advocacy, lived experience and broader patient community support
Together, they help create a stronger support network for people living with aspergillosis.
Why Patient Participation Matters
Patient experience is one of the most valuable resources in improving understanding of aspergillosis.
People living with aspergillosis often understand challenges that are not always visible in clinical appointments, including:
- Diagnostic delays
- Fatigue and fluctuating symptoms
- Treatment side effects
- Emotional impact
- Difficulties accessing information and support
By sharing experiences and becoming involved in awareness and advocacy activities, patients and carers can help improve understanding and support for others.
Participation does not need to be overwhelming. It can include:
- Sharing experiences confidentially
- Joining online discussions or support groups
- Supporting awareness campaigns
- Attending educational events
- Helping improve patient information
- Participating in surveys or research projects
Even small contributions can help improve awareness and care for future patients.
How to Learn More or Get Involved
- Aspergillosis Trust Website
- European Lung Foundation Aspergillosis Pages
- National Aspergillosis Centre Resources
The Aspergillosis Trust demonstrates the importance of patient-led advocacy in rare and under-recognised diseases. Through education, awareness and community support, the charity helps ensure that people living with aspergillosis are better informed, better supported and increasingly heard.
What a Space-Resistant Fungus Can Teach Us About Aspergillosis
A recent Smithsonian article described how a microscopic fungus survived conditions designed to sterilise spacecraft. At first glance, this might sound like a story about space exploration rather than human health. But for people living with aspergillosis, it carries an important and surprisingly positive message.
Fungi are remarkable survivors
The article describes research showing that some Aspergillus spores can survive extreme conditions, including harsh radiation, dryness and cleaning procedures. This does not mean that aspergillosis patients need to worry about “space fungi”. Instead, it highlights something patients and specialists already understand very well: fungi are extraordinarily resilient organisms.
Aspergillus spores are common in the environment. They can be found in soil, compost, decaying leaves, dust, damp buildings and sometimes even very clean environments. Most people breathe in small numbers of spores every day without becoming ill, because their lungs and immune system clear them effectively.
For people with lung disease, asthma, immune system problems or damaged lung tissue, however, Aspergillus can sometimes cause illness. This includes conditions such as chronic pulmonary aspergillosis, allergic bronchopulmonary aspergillosis and severe asthma with fungal sensitisation.
A positive message for patients
One positive message from this research is that aspergillosis is not caused by weakness, poor hygiene or personal failure. Fungi are genuinely formidable organisms. If some fungal spores can survive environments as extreme as those used in space research, it becomes easier to understand why completely avoiding Aspergillus in everyday life is difficult.
This can be reassuring for patients who feel frustrated when symptoms persist despite doing “everything right”. It is not that they are failing. It is that fungal biology is complex, and fungal exposure is part of the natural world.
Why this matters emotionally
Many people with aspergillosis say they feel misunderstood. They may hear comments such as:
- “It’s only mould.”
- “Surely it should have cleared by now.”
- “Why are you still worrying about it?”
Stories like this help show that fungi are not simple or trivial. They are ancient, adaptable and scientifically fascinating organisms. Aspergillosis is therefore not “just mould exposure”; it is a real medical condition involving a complex interaction between the fungus, the lungs and the immune system.
Science is taking fungi more seriously
Another encouraging message is that fungi are attracting more scientific attention. Researchers are studying fungal survival, environmental spread, resistance to treatment, and the ways fungi interact with humans and indoor environments.
This matters because better understanding can lead to better diagnosis, better treatment and better prevention. In recent years, fungal medicine has already benefited from improvements in CT scanning, fungal blood tests, respiratory samples, antifungal treatments and biologic medicines for some allergic forms of disease.
Resilience goes both ways
The story also offers a useful reflection: fungi are resilient, but so are patients.
Many people living with aspergillosis adapt to long-term symptoms, hospital appointments, uncertainty, fatigue and treatment decisions. They continue to work, care for families, attend support groups, learn about their condition and help others understand fungal disease.
That resilience deserves recognition.
What patients can take from this
- Aspergillus is difficult to avoid completely, so exposure reduction should be realistic rather than perfectionist.
- Persistent symptoms are not a personal failure; fungal diseases can be complex and long-lasting.
- Fungal science is advancing, and aspergillosis is increasingly recognised as an important medical condition.
- Patients’ experiences are valid, even when others do not fully understand them.
When to seek medical advice
People with aspergillosis or suspected aspergillosis should seek medical advice if they develop worsening breathlessness, coughing up blood, unexplained weight loss, persistent fever, chest pain, a major change in sputum, or a significant deterioration in day-to-day symptoms.
Anyone already under specialist care should follow their agreed care plan and contact their clinical team if symptoms change significantly.
Further reading
- Smithsonian Magazine: fungus surviving spacecraft sterilisation conditions
- Aspergillosis.org: patient information and support
Last reviewed: May 2026
Understanding Steroids, Cortisol, ACTH and Adrenal Suppression in Aspergillosis
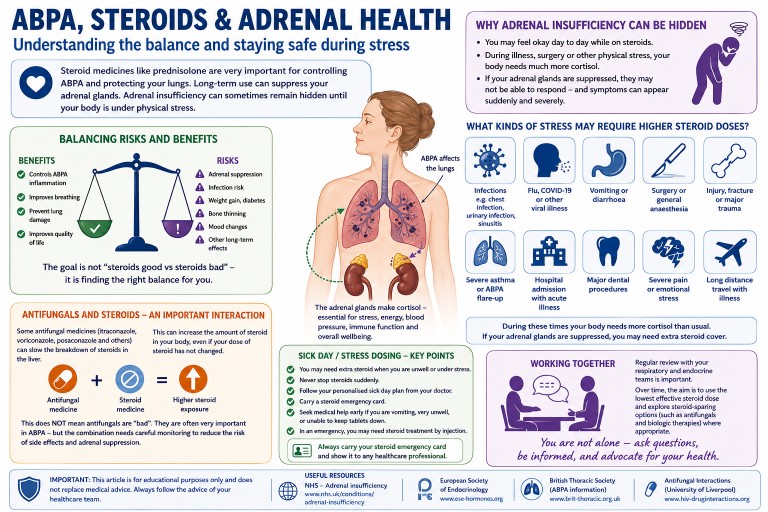
For people with Allergic Bronchopulmonary Aspergillosis (ABPA), severe asthma and other forms of aspergillosis, steroid treatment can be both extremely helpful and medically complicated.
Many patients are prescribed corticosteroids such as prednisolone or methylprednisolone to control inflammation, improve breathing and reduce the risk of lung damage. These medicines can be very effective. However, repeated or long-term steroid treatment can also affect the body’s natural hormone system, especially the adrenal glands.
Some patients are told:
- “Your cortisol is low.”
- “Your ACTH level is abnormal.”
- “You may have adrenal suppression.”
- “This may be steroid withdrawal.”
- “The blood tests are difficult to interpret.”
This can be worrying and confusing, especially when symptoms are severe but the explanation is not straightforward.
This article explains why adrenal problems can occur in some people with aspergillosis and severe asthma, why blood tests such as cortisol and ACTH can be difficult to interpret, and why steroid treatment sometimes involves a careful balance between benefit and risk.
Key points summary
- Steroid medicines can reduce the body’s own natural cortisol production.
- This is called adrenal suppression or adrenal insufficiency.
- Symptoms may overlap with aspergillosis, asthma, infection, fatigue or steroid withdrawal.
- Blood tests such as cortisol and ACTH can be difficult to interpret.
- Inhaled steroids and antifungal medicines can also influence steroid effects.
- Long-term prednisolone is generally avoided where possible, but it may still be necessary for some patients.
- Patients should not stop or reduce steroids suddenly without medical advice.
- Severe symptoms such as collapse, vomiting, dehydration, confusion or severe weakness require urgent medical advice.
Contents
- What do the adrenal glands do?
- What are cortisol and ACTH?
- Why are steroids used in ABPA and aspergillosis?
- Are steroids only meant for short-term use?
- How steroids affect the body’s natural hormone system
- What is adrenal suppression?
- Why symptoms can be difficult to recognise
- Why blood tests can become confusing
- The role of inhaled steroids
- Antifungal medicines and steroid interactions
- Steroid withdrawal versus adrenal insufficiency
- What kinds of stress may require higher steroid doses?
- When should patients seek urgent medical advice?
- Frequently asked questions
- Final thoughts
What do the adrenal glands do?
The adrenal glands are small glands that sit above the kidneys. They produce several important hormones, including cortisol.
Cortisol helps the body:
- respond to stress,
- maintain blood pressure,
- regulate energy levels,
- support immune function,
- and cope with illness or infection.
The body carefully controls cortisol levels through a hormone signalling system involving the brain, the pituitary gland and the adrenal glands.
What are cortisol and ACTH?
ACTH stands for adrenocorticotropic hormone.
The pituitary gland in the brain releases ACTH to tell the adrenal glands to produce cortisol.
This system normally works as a feedback loop:
- When cortisol is low, ACTH usually rises.
- When cortisol is high, ACTH usually falls.
Cortisol levels naturally change during the day and are usually highest in the early morning. This is one reason why many cortisol blood tests are taken around 9am.
Why are steroids used in ABPA and aspergillosis?
In Allergic Bronchopulmonary Aspergillosis (ABPA) and some severe asthma conditions, the immune system reacts strongly to Aspergillus fungi.
This can cause:
- airway inflammation,
- wheezing,
- coughing,
- mucus plugging,
- breathlessness,
- worsening lung function,
- and repeated flare-ups.
Steroids such as prednisolone are often used because they reduce inflammation quickly and effectively.
Some patients may need:
- short courses during flare-ups,
- repeated courses,
- long-term low-dose treatment,
- inhaled steroid therapy,
- antifungal treatment,
- or biologic medicines to reduce the need for oral steroids.
For many patients, steroids are not optional or casual medicines. They may be essential treatments used to control serious inflammation and protect lung function.
Are steroids only meant for short-term use?
Patients sometimes hear that prednisolone was “only designed for short-term use”. This is understandable, because modern medical practice tries to avoid long-term steroid treatment where possible.
Long-term oral corticosteroids can cause significant side effects, including:
- adrenal suppression,
- diabetes or worsening blood sugar control,
- osteoporosis and fracture risk,
- increased infection risk,
- cataracts or glaucoma,
- muscle weakness,
- skin thinning and bruising,
- weight gain,
- sleep disturbance,
- and mood or mental health effects.
For this reason, doctors usually aim to use steroids at the lowest effective dose for the shortest safe time.
However, it is also important not to oversimplify this message. Some people with ABPA, severe asthma or other inflammatory lung conditions do need longer-term steroid treatment because the disease itself can be dangerous if not controlled.
In some patients, the risk of uncontrolled lung inflammation may outweigh the risks of steroid treatment, at least for a period of time.
Modern care increasingly tries to reduce steroid exposure by using other approaches where appropriate, such as:
- antifungal treatment,
- biologic medicines for severe asthma or ABPA-type inflammation,
- careful monitoring of lung function and blood tests,
- gradual steroid tapering,
- bone protection where needed,
- diabetes monitoring,
- and regular review of whether the steroid dose can be reduced.
The key message is not that patients have done anything wrong by needing steroids. The key message is that long-term steroid treatment deserves careful monitoring, honest discussion and regular review.
Patient reassurance: If you have needed prednisolone for ABPA or severe asthma, this does not mean you have failed or made a poor choice. It usually means your medical team has been trying to control a potentially serious inflammatory condition. The aim is to balance benefit and risk as safely as possible.
Balancing risks and benefits
One of the hardest parts of long-term steroid treatment is that two important things can be true at the same time:
- steroids can cause serious side effects,
- and steroids can also prevent serious lung damage and dangerous flare-ups.
Patients sometimes feel guilty, frustrated or frightened when they hear about the risks of prednisolone. Others may feel judged for “still being on steroids”.
However, many people with ABPA or severe asthma did not choose steroids lightly. Steroids are often prescribed because uncontrolled inflammation itself can damage the lungs, worsen bronchiectasis, increase hospital admissions and significantly reduce quality of life.
Modern respiratory care increasingly tries to reduce steroid exposure where possible using:
- antifungal therapy,
- biologic medicines,
- careful monitoring,
- gradual tapering plans,
- and better recognition of steroid side effects.
But for some patients, steroids may still remain an important part of treatment, even if the goal is eventually to reduce the dose.
The most helpful approach is usually not “steroids are good” or “steroids are bad”, but rather:
- What dose is truly needed?
- Can the dose be safely reduced?
- Are side effects being monitored properly?
- Are there alternative treatments available?
- And is the patient being listened to when symptoms change?
This balanced approach is increasingly recognised as one of the most important parts of caring for people with severe asthma and aspergillosis.
How steroids affect the body’s natural hormone system
Steroid medicines act in ways that are similar to natural cortisol.
When the body senses steroid medication in the bloodstream, it may reduce its own ACTH production. Over time, this can mean:
- ACTH falls,
- the adrenal glands become less active,
- and natural cortisol production decreases.
Doctors sometimes describe this as the adrenal glands “going to sleep”.
This is called:
- adrenal suppression,
- steroid-induced adrenal insufficiency,
- or hypothalamic-pituitary-adrenal axis suppression.
What is adrenal suppression?
Adrenal suppression means the body may not produce enough cortisol when it is needed.
This can become especially important during:
- infection,
- surgery,
- injury,
- severe stress,
- or rapid steroid reduction.
Some patients develop symptoms gradually. Others notice problems when trying to reduce steroid doses.
Because cortisol is part of the body’s stress response, people with adrenal insufficiency may need specific medical advice about what to do during illness, vomiting, surgery or severe infection.
Why symptoms can be difficult to recognise
Symptoms of adrenal suppression can overlap with many other conditions common in people with aspergillosis, ABPA or severe asthma.
Possible symptoms include:
- profound tiredness,
- weakness,
- dizziness,
- sweating,
- shakiness,
- nausea,
- muscle aches,
- low mood,
- brain fog,
- reduced exercise tolerance,
- poor recovery after illness,
- or feeling suddenly much worse after reducing steroids.
These symptoms may also occur with:
- an ABPA flare,
- asthma worsening,
- lung infection,
- chronic illness,
- poor sleep,
- anxiety,
- or steroid withdrawal.
This overlap is one reason why patients can feel frustrated or uncertain. Symptoms are real, even when the cause is difficult to pin down.
Why blood tests can become confusing
Many patients expect blood tests to give clear answers, but cortisol and ACTH results are often complicated.
Several things can affect results:
- time of day,
- recent steroid use,
- the type of steroid used,
- inhaled steroid dose,
- recent dose reductions,
- illness or stress,
- laboratory methods,
- and antifungal medicines.
Typical patterns
In classic steroid-induced adrenal suppression:
- cortisol is low,
- and ACTH is low or “inappropriately normal”.
This happens because steroid medication suppresses ACTH production.
However, real-life cases are not always straightforward. Some patients may have recently reduced steroids, missed doses, changed steroid type, used high-dose inhaled steroids, or taken antifungal medicines that alter steroid metabolism.
In some situations, endocrinologists may need repeated testing or dynamic tests such as a Synacthen test to understand whether the adrenal glands can respond properly.
It is important that patients do not try to interpret cortisol or ACTH results in isolation. The result needs to be understood alongside symptoms, medication history, timing of the sample and the clinical situation.
The role of inhaled steroids
Many people assume inhaled steroids only affect the lungs.
Inhaled steroids usually have fewer whole-body effects than long-term oral steroids, but high doses can sometimes contribute to adrenal suppression, especially when combined with:
- long-term or repeated oral steroid courses,
- azole antifungal medicines,
- other medicines that affect steroid metabolism,
- or individual differences in how medicines are processed.
This does not mean inhaled steroids are unsafe or should be stopped suddenly. For many people with asthma or ABPA, inhaled steroids are an important part of keeping airway inflammation under control.
It does mean that total steroid exposure should be reviewed carefully, especially in patients with symptoms suggestive of adrenal suppression.
Antifungal medicines and steroid interactions
This is an especially important issue in aspergillosis.
Antifungal medicines such as:
- itraconazole,
- voriconazole,
- posaconazole,
- and isavuconazole
can interact with other medicines, including corticosteroids.
Some azole antifungals slow the breakdown of steroids in the liver. This can increase the body’s exposure to steroid medication, meaning that even doses which initially appear moderate may sometimes behave more like higher doses inside the body.
This interaction may increase the risk of:
- adrenal suppression,
- Cushing-like side effects,
- weight gain,
- skin thinning,
- easy bruising,
- high blood sugar,
- muscle weakness,
- or hormonal imbalance.
The interaction can be particularly important in patients taking:
- oral prednisolone or methylprednisolone,
- high-dose inhaled steroids,
- multiple steroid preparations together,
- or repeated steroid courses over time.
Some patients tolerate steroid treatment reasonably well for long periods before antifungal medicines are added. Endocrine problems may then become more noticeable later, especially during:
- infection,
- surgery,
- vomiting or diarrhoea,
- major physical stress,
- rapid steroid reduction,
- or severe asthma or ABPA flare-ups.
This can feel as though adrenal insufficiency has appeared “suddenly” or “out of nowhere”, when in reality the adrenal glands may have been partially suppressed for some time.
Why adrenal insufficiency may only become obvious during illness or stress
Some patients with steroid-related adrenal suppression cope reasonably well during normal day-to-day life, especially while still taking regular steroids. However, the problem may become much more noticeable when the body faces significant physical stress.
Under normal circumstances, the body rapidly increases cortisol production during severe illness or injury. If the adrenal glands cannot respond properly, symptoms may suddenly become much more severe.
Patients sometimes describe:
- “crashing” during an infection,
- extreme exhaustion,
- severe weakness,
- dizziness or collapse,
- poor recovery after illness,
- or feeling suddenly unable to cope physically.
This does not mean every severe illness in an ABPA patient is caused by adrenal insufficiency. Infections, inflammation and lung disease themselves are often the major problem. However, adrenal suppression can sometimes contribute to deterioration and may only reveal itself during periods of stress or acute illness.
This is one reason why some patients are given “sick day rules”, emergency steroid cards or advice about temporary steroid dose increases during illness.
Importantly, this does not mean antifungal medicines are “bad” or should be avoided. In many patients, antifungal treatment significantly improves ABPA control and may eventually help reduce steroid exposure overall. The important message is that these combinations require awareness, monitoring and careful medical supervision.
Patients should never stop antifungal or steroid medicines suddenly without medical advice.
Steroid withdrawal versus adrenal insufficiency
Steroid withdrawal and adrenal insufficiency can feel very similar.
Steroid withdrawal
When steroid doses are reduced, the body may take time to adjust. Patients can temporarily feel unwell even if the adrenal glands are slowly recovering.
Adrenal insufficiency
Adrenal insufficiency means the body cannot produce enough cortisol to meet its needs.
Symptoms may overlap considerably. Recovery can sometimes take weeks or months, and in some patients longer.
For many patients, one of the hardest parts is that they may “look well” externally while feeling exhausted internally.
It is important that symptoms are not dismissed simply because they are difficult to measure.
What kinds of stress may require higher steroid doses?
Patients who have adrenal insufficiency or significant adrenal suppression may sometimes be advised to temporarily increase steroid doses during periods of physical stress. This is often called following “sick day rules”.
The body normally produces extra cortisol during stress, illness or injury. If the adrenal glands cannot respond properly, extra steroid medication may sometimes be needed to prevent serious illness.
Examples of situations that may place significant stress on the body include:
- high fever or significant infection,
- chest infection or pneumonia,
- vomiting or diarrhoea,
- COVID-19 or influenza,
- major dental treatment or surgery,
- fractures or significant injury,
- general anaesthetic procedures,
- severe asthma attacks or ABPA flare-ups,
- hospital admission with acute illness,
- or severe physical exhaustion associated with illness.
The exact advice varies between patients depending on:
- whether adrenal insufficiency has been formally diagnosed,
- the steroid dose currently being taken,
- how suppressed the adrenal glands are thought to be,
- other medical conditions,
- and guidance from endocrine or respiratory specialists.
Some patients are provided with:
- specific “sick day rules”,
- an emergency steroid card,
- medical alert jewellery,
- or emergency hydrocortisone injection kits.
Patients should only adjust steroid doses according to the advice provided by their medical team. If severe vomiting, collapse, confusion, inability to keep medication down or major deterioration occurs, urgent medical advice is needed.
When should patients seek urgent medical advice?
Patients should seek urgent medical help if they experience:
- collapse,
- fainting,
- severe vomiting,
- inability to keep steroid medication down,
- severe dehydration,
- confusion,
- severe weakness,
- very low blood pressure,
- or sudden major deterioration during illness.
These symptoms can occasionally indicate adrenal crisis, which is a medical emergency.
Patients who have been told they are at risk of adrenal insufficiency should follow the emergency and “sick day” advice given by their endocrine or respiratory team.
Frequently asked questions
Does everyone taking steroids develop adrenal suppression?
No. Risk depends on factors such as dose, duration, repeated courses, inhaled steroid dose, other medicines and individual sensitivity.
Can adrenal function recover?
Yes. Many patients gradually recover adrenal function over time, although recovery speed varies.
Are inhaled steroids safer than tablets?
Inhaled steroids usually have fewer whole-body effects than long-term oral steroids, but high doses can still contribute to adrenal suppression in some patients, especially when combined with certain antifungal medicines.
Why do I feel worse when reducing steroids?
This can happen for several reasons. The underlying lung disease may flare, the body may be adjusting to lower steroid levels, or cortisol production may not yet have recovered.
Does needing long-term prednisolone mean something has gone wrong?
Not necessarily. Long-term prednisolone is usually avoided where possible because of side effects, but some patients need it to control serious inflammation. The aim is regular review, careful monitoring and dose reduction when it is safe.
Should I stop steroids because of this risk?
No patient should stop prescribed steroids suddenly unless specifically advised by their medical team. Sudden withdrawal can be dangerous, especially if the body’s own cortisol production is suppressed.
Final thoughts
Adrenal suppression and steroid-related hormone problems are recognised complications of corticosteroid treatment.
For patients with aspergillosis, ABPA and severe asthma, the situation can become especially complex because:
- steroid treatment may be medically necessary,
- symptoms overlap with many other conditions,
- antifungal medicines may interact with steroids,
- inhaled steroids may add to total steroid exposure,
- and blood tests are not always straightforward.
Patients sometimes feel frustrated because their symptoms are difficult to explain or measure clearly. However, these experiences are recognised by clinicians and researchers, and steroid-related adrenal problems are increasingly acknowledged as important and sometimes under-recognised.
The goal is not to create fear of steroids. The goal is to use them carefully, monitor them properly, reduce them when possible, and support patients through the difficult process of balancing disease control with treatment side effects.
Suggested internal links
- ABPA treatment overview
- Steroid side effects
- Antifungal drug interactions
- Fatigue and aspergillosis
- Severe asthma and biologics
- Living with long-term aspergillosis
- Mental wellbeing and chronic illness
- Aspergillosis.org Knowledge Hub
References and further reading
When was this article last reviewed?
Last reviewed: May 2026
Author and review information
Prepared for patient education and support purposes.
This article is intended for general educational use and should not replace personalised medical advice from a healthcare professional.