
About the National Aspergillosis Centre (NAC)
The UK's specialist centre for aspergillosis
The National Aspergillosis Centre (NAC) is a specialist NHS service based at Wythenshawe Hospital in Manchester, part of Manchester University NHS Foundation Trust.
NAC provides expert assessment, diagnosis, treatment and long-term management for people with complex forms of aspergillosis, particularly Chronic Pulmonary Aspergillosis (CPA). The centre also supports healthcare professionals across the United Kingdom with specialist advice, guidance and multidisciplinary case discussion.
Alongside its clinical work, NAC supports research, education and patient engagement, helping improve understanding and care of aspergillosis nationally and internationally.
National Aspergillosis Centre at a glance
| Service | National Aspergillosis Centre (NAC) |
| Location | Wythenshawe Hospital, Manchester |
| Organisation | Manchester University NHS Foundation Trust |
| Specialty | Complex aspergillosis care |
| National role | NHS specialist referral service |
| Supports | Patients and healthcare professionals across the UK |
What is aspergillosis?
Aspergillosis is a group of conditions caused by fungi from the Aspergillus family. These fungi are commonly found in the environment, and most people breathe in Aspergillus spores every day without becoming ill.
In some circumstances, however, Aspergillus can cause disease. This may occur because of underlying lung disease, asthma or allergic conditions, a weakened immune system, structural lung damage or previous lung infections.
Which conditions does NAC help manage?
Chronic Pulmonary Aspergillosis (CPA)
CPA is a long-term fungal infection of the lungs that can develop in people who already have lung damage or cavities caused by previous illness.
Allergic Bronchopulmonary Aspergillosis (ABPA)
ABPA is an allergic reaction to Aspergillus that most commonly affects people with asthma or cystic fibrosis.
Aspergillus bronchitis
Aspergillus bronchitis is a chronic airway infection in which Aspergillus is repeatedly identified in the airways and contributes to ongoing respiratory symptoms.
Other complex Aspergillus-related conditions
- Aspergillus nodules
- Severe Asthma with Fungal Sensitisation (SAFS)
- complex diagnostic cases
- difficult-to-treat aspergillosis
- antifungal treatment complications
- therapeutic drug monitoring
Not all patients with aspergillosis need referral to NAC. Many people receive excellent care through local respiratory, infectious diseases, allergy or severe asthma services.
How do referrals work?
Patients are normally referred by a healthcare professional. Referrals may come from respiratory physicians, infectious diseases specialists, immunologists, severe asthma services or general practitioners working with specialist teams.
NAC also supports clinicians through remote advice services and multidisciplinary discussions, helping many patients receive specialist input without needing regular travel to Manchester.
What happens at a NAC appointment?
Every patient is different, but assessment may include:
- review of symptoms and medical history
- review of computed tomography (CT) scans and other imaging
- blood test review
- review of microbiology and fungal test results
- assessment of antifungal treatment
- therapeutic drug monitoring
- discussion of future treatment options
Patients often continue to receive much of their care locally, with specialist recommendations provided by NAC.
Specialist aspergillosis care across the UK
Although NAC is the UK's national specialist centre for chronic aspergillosis, specialist care is also provided through many hospitals and specialist services across the country.
Depending on the condition involved, patients may receive care from respiratory medicine services, bronchiectasis clinics, severe asthma centres, infectious diseases departments, allergy services or immunology services.
The most appropriate service depends on the type of aspergillosis and the patient's individual circumstances.
Research and innovation
Research is a central part of the work carried out by NAC and its partners. Areas of ongoing research include improved diagnostics, new antifungal medications, biologic therapies, therapeutic drug monitoring, imaging, disease monitoring, patient experience and clinical trials.
Education and patient support
The National Aspergillosis Centre is committed to helping patients and carers understand their condition and access reliable information.
Resources available through aspergillosis.org include:
- over 1,000 patient information articles
- condition-specific Knowledge Hubs
- support meetings
- recorded educational talks
- patient stories
- research updates
- guidance for carers and families
Working together
Effective aspergillosis care relies on collaboration between patients, carers, local healthcare teams and specialist services.
NAC works closely with healthcare professionals, researchers, patient organisations and charities to improve awareness, diagnosis, treatment and support for people living with aspergillosis.
Frequently asked questions
What is the National Aspergillosis Centre?
The National Aspergillosis Centre is a specialist NHS service based at Wythenshawe Hospital in Manchester. It provides expert care and advice for complex forms of aspergillosis, especially Chronic Pulmonary Aspergillosis.
Where is NAC located?
NAC is based at Wythenshawe Hospital in Manchester, part of Manchester University NHS Foundation Trust.
Who can be referred to NAC?
Patients with complex or difficult-to-manage aspergillosis may be referred by a healthcare professional. Many referrals involve Chronic Pulmonary Aspergillosis, but NAC also provides advice for other Aspergillus-related conditions.
Can I refer myself to NAC?
Patients are normally referred by a healthcare professional. If you believe specialist input may be helpful, discuss this with your clinical team.
Do I have to live near Manchester?
No. Patients are referred from throughout the United Kingdom, and NAC also supports clinicians remotely.
Does everyone with aspergillosis need NAC?
No. Many patients are managed successfully by local specialist teams. NAC is primarily involved in complex cases and specialist advice.
Does NAC only treat CPA?
No. Although NAC is especially known for Chronic Pulmonary Aspergillosis, it also provides advice and support for a range of complex Aspergillus-related conditions.
What happens during a NAC appointment?
A NAC appointment may include review of symptoms, scans, blood tests, microbiology results, antifungal treatment, drug levels and future treatment options.
Does NAC provide patient support?
Yes. Through aspergillosis.org and the NAC CARES programme, patients and carers can access educational resources, support meetings and community activities.
Suggested links
- Manchester University NHS FT Aspergillosis for full details, referral
- What is aspergillosis?
- Chronic Pulmonary Aspergillosis (CPA)
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Aspergillus bronchitis
- Aspergillosis Knowledge Hub
- Find an aspergillosis clinic
- Support meetings and community
- Information for professionals
- Latest articles and research updates
About this page
This page was prepared by the National Aspergillosis Centre CARES team to explain the role of the National Aspergillosis Centre and how specialist aspergillosis care is provided within the UK healthcare system.
Last reviewed: June 2026

Why the UK’s Infection Specialist Workforce Matters to People Living with Aspergillosis

A new national report has called for urgent action to strengthen and modernise the UK’s infection-specialist workforce. The report, Infection Prevention and Management in the UK: The Infection-Specialist Workforce, was published by the Healthcare Infection Society and partner organisations across the infection community.
At first glance, workforce planning may sound like an issue mainly for hospitals, universities, laboratories and policymakers. However, for people living with aspergillosis and other complex fungal diseases, the availability of specialist expertise can directly affect diagnosis, treatment, access to advice and long-term outcomes.
Why this matters to patients
Aspergillosis is not a single disease. It includes conditions such as Allergic Bronchopulmonary Aspergillosis (ABPA), Chronic Pulmonary Aspergillosis (CPA), Aspergillus bronchitis and invasive aspergillosis.
These conditions are often complex, uncommon and difficult to recognise. Many patients describe long journeys to diagnosis, sometimes involving repeated chest infections, worsening asthma, unexplained fatigue, weight loss, breathlessness, abnormal scans or uncertainty about the meaning of test results.
When specialist infection, respiratory, laboratory and mycology expertise is difficult to access, patients may face longer waits for diagnosis, referral and treatment decisions.
Why this matters to professionals
The report highlights the central role of the infection-specialist workforce in clinical care, diagnostics, infection prevention and control, antimicrobial stewardship, public health and system preparedness.
This workforce includes infectious diseases physicians, clinical microbiologists, virologists, medical mycologists, infection prevention specialists, specialist nurses, antimicrobial pharmacists, biomedical scientists and clinical scientists.
For fungal disease, this multidisciplinary expertise is essential. Diagnosing and managing aspergillosis often requires careful interpretation of clinical history, imaging, fungal culture, Aspergillus antibody testing, galactomannan, molecular diagnostics, antifungal drug levels, susceptibility results and treatment toxicity monitoring.
What workforce shortages can mean in practice
For patients with aspergillosis, workforce pressures may contribute to:
- Delays in recognising possible fungal disease.
- Delays in referral to specialist services.
- Variation in access to expertise between regions.
- Longer waits for interpretation of specialist tests.
- Reduced capacity for multidisciplinary team discussion.
- Greater pressure on specialist centres and laboratories.
- Delays in accessing newer diagnostics, antifungal treatments or clinical trials.
For professionals, these pressures can make already complex work more difficult. Clinicians may be managing patients with rare fungal disease alongside heavy general respiratory, microbiology, infectious diseases or laboratory workloads. Specialist advice networks and reference services therefore become increasingly important.
The importance of medical mycology
Fungal diseases remain under-recognised compared with many bacterial and viral infections, despite causing serious illness in people with chronic lung disease, immune suppression, transplantation, cancer treatment or prolonged critical illness.
Medical mycology is a highly specialised area. It supports accurate diagnosis, antifungal treatment selection, interpretation of complex tests and recognition of emerging resistance. Without sufficient mycology expertise, advances in fungal diagnostics and treatment may not reach patients quickly or consistently.
The role of specialist centres
The UK benefits from specialist services such as the National Aspergillosis Centre, which provides expert assessment, multidisciplinary review and advice for patients with complex forms of aspergillosis.
However, specialist centres cannot work in isolation. Earlier recognition by GPs, respiratory teams, radiologists, microbiologists, infectious diseases teams and local laboratories is vital. Strong referral pathways help patients reach the right expertise at the right time.
For rare fungal diseases, national specialist centres and local services need to function as part of a connected system rather than as separate parts of care.
A patient safety and equity issue
Access to infection expertise is also an equity issue. Patients should not face very different chances of diagnosis or specialist input depending on where they live.
Strengthening the infection-specialist workforce could help reduce variation in care, support earlier diagnosis and improve access to expert advice across the UK.
Looking ahead
New antifungal drugs, improved diagnostics, molecular testing, genomics and clinical trials are creating new opportunities to improve aspergillosis care.
But innovation only helps patients if there are trained professionals available to recognise fungal disease, request appropriate tests, interpret results, prescribe and monitor treatment, and work across multidisciplinary teams.
For patients and professionals alike, the message is clear: strengthening the UK’s infection-specialist workforce is not simply a staffing issue. It is essential for earlier diagnosis, safer treatment, better access to expertise and more equitable care for people living with complex fungal diseases.
What does this mean for people living with aspergillosis?
- Specialist expertise can help shorten the journey to diagnosis.
- Better workforce capacity can improve access to advice and referral.
- Strong laboratory services are essential for accurate fungal diagnosis.
- Medical mycology expertise helps guide safe and effective treatment.
- More consistent access to specialist care could reduce regional inequality.
Further reading
- Healthcare Infection Society: Infection Specialist Workforce Report
- Royal College of Pathologists: New report calls for urgent action to strengthen the UK’s infection specialist workforce
Frequently Asked Questions
Why are infection specialists important for aspergillosis?
Aspergillosis can be difficult to diagnose and manage. Infection specialists, respiratory clinicians, microbiologists and medical mycologists help identify fungal disease, interpret specialised tests and guide treatment decisions.
What is medical mycology?
Medical mycology is the branch of medicine and laboratory science concerned with fungal diseases affecting humans. Specialists in medical mycology help diagnose and manage infections caused by fungi such as Aspergillus.
Why can aspergillosis take a long time to diagnose?
The symptoms of aspergillosis often overlap with those of more common respiratory conditions such as asthma, chronic obstructive pulmonary disease (COPD), bronchiectasis and recurrent chest infections. Specialist investigations and expert interpretation are frequently required.
How could workforce shortages affect patients?
Workforce shortages may contribute to delays in diagnosis, referral and access to specialist advice. They can also place additional pressure on laboratories, multidisciplinary teams and specialist centres.
What role do specialist laboratories play?
Specialist laboratories perform fungal cultures, Aspergillus antibody testing, antigen testing, molecular diagnostics and antifungal susceptibility testing. These investigations are often essential for accurate diagnosis and treatment planning.
What is the National Aspergillosis Centre?
The National Aspergillosis Centre (NAC) is a UK specialist service providing expert assessment, multidisciplinary review and management advice for patients with complex aspergillosis.
Will new treatments solve these problems?
New antifungal medicines and diagnostic technologies offer significant opportunities to improve care. However, trained healthcare professionals are still needed to recognise disease, request investigations, interpret results and monitor treatment safely.
How can patients help improve awareness of aspergillosis?
Patients can help by sharing reliable information, supporting awareness campaigns, participating in patient groups and, where appropriate, contributing to research and patient involvement activities.
Last reviewed: June 2026
Suggested audience: Patients, carers, respiratory clinicians, infectious diseases clinicians, microbiologists, medical mycologists, specialist nurses, pharmacists, biomedical scientists, clinical scientists, commissioners and service planners.
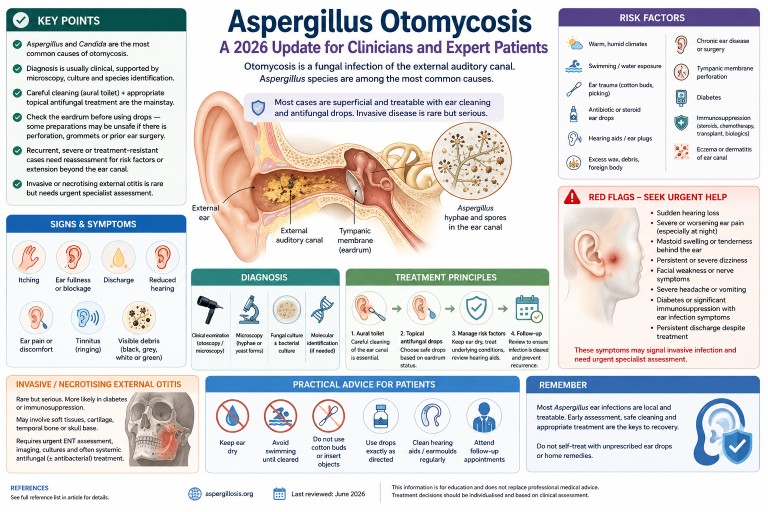
Aspergillus Otomycosis: A 2026 Update for Clinicians and Expert Patients
Article type: Clinical and expert-patient evidence updateIntended audience: Ear, nose and throat clinicians, infectious diseases specialists, medical mycologists, general practitioners, specialist nurses, expert patients and carers.Last reviewed: June 2026
Key points
- Otomycosis is a fungal infection of the external auditory canal. It is often described as fungal otitis externa.
- Aspergillus species and Candida species are the most commonly reported causes.
- Older reports often describe Aspergillus niger as the main cause, but molecular methods show that related black Aspergillus species, including Aspergillus tubingensis, may previously have been misidentified as A. niger.
- Diagnosis is usually clinical, supported where possible by microscopy, fungal culture and species identification.
- Successful treatment usually requires careful cleaning of the ear canal as well as appropriate topical antifungal treatment.
- Before topical treatment is used, clinicians should assess whether the tympanic membrane is intact, because some preparations may be unsafe if there is perforation, grommets, a mastoid cavity or previous ear surgery.
- Most cases are superficial, but recurrent, severe or treatment-resistant disease should prompt reassessment for mixed bacterial infection, diabetes, immunosuppression, hearing aid moulds, foreign body, chronic ear disease or extension beyond the external canal.
- Invasive or necrotising external otitis is rare but serious and requires urgent specialist assessment.
- Sudden hearing loss, facial weakness, severe persistent pain, mastoid swelling or tenderness, neurological symptoms, or infection in a person with diabetes or significant immunosuppression should be treated as red flags.
Contents
- What is otomycosis?
- Aspergillus ear infection is different from lung aspergillosis
- Why Aspergillus matters
- Epidemiology and why cases may be missed
- Causative Aspergillus species
- Risk factors
- Symptoms and clinical features
- Diagnosis
- Differential diagnosis
- Treatment principles
- Recurrent or treatment-resistant otomycosis
- Invasive Aspergillus ear infection and necrotising external otitis
- Practical advice for patients
- Frequently asked questions
- When to seek urgent medical help
- Evidence gaps and uncertainty
- References
What is otomycosis?
Otomycosis is a fungal infection of the external auditory canal, the skin-lined passage leading from the outer ear to the eardrum. It is also called fungal otitis externa. The infection may be acute, subacute or chronic, and it can be mistaken for bacterial otitis externa, eczema, wax, chronic discharge or non-specific inflammation.
In most people, otomycosis is a superficial infection of the outer ear canal. It can be uncomfortable, persistent and prone to recurrence, but it is usually treatable when the ear is examined, cleaned and treated appropriately. Rarely, particularly in people with diabetes, immunosuppression, previous ear surgery or severe persistent symptoms, infection may spread beyond the ear canal and become invasive.
Plain-English summary: most Aspergillus ear infections affect the outer ear canal. They are usually not the same as invasive aspergillosis in the lungs or bloodstream, but they can still need specialist ear care to clear the infection safely.
Aspergillus ear infection is different from lung aspergillosis
Many people searching online for Aspergillus find information about chronic pulmonary aspergillosis, allergic bronchopulmonary aspergillosis or invasive aspergillosis. These are different conditions.
Aspergillus otomycosis usually affects the external ear canal only. It is usually a local fungal infection rather than a whole-body infection. It does not usually mean that a person has invasive aspergillosis, chronic pulmonary aspergillosis or allergic bronchopulmonary aspergillosis.
However, people with existing lung disease, diabetes, immune suppression or complex medical histories should still tell their clinician about these conditions, because they may affect assessment and treatment decisions.
Why Aspergillus matters
Aspergillus is a common environmental mould. Its spores are present in air, dust, soil, compost, decaying vegetation and indoor environments. In the ear canal, fungal growth is favoured when local conditions change. Moisture, trauma to the skin, loss of normal wax protection, altered acidity, previous antibiotic or steroid drops, retained debris and obstruction from hearing aid moulds or ear plugs can all make fungal overgrowth more likely.
In otomycosis, Aspergillus species are among the most frequently reported fungi. They are particularly important because their appearance in the ear can be striking, with black, grey, greenish, yellow-white or fluffy debris. However, appearance alone is not enough for precise species identification.
Epidemiology and why cases may be missed
Reported prevalence varies considerably between studies and geographical regions. Otomycosis is more common in some warm, humid or dusty environments, but it is reported worldwide, including in the United Kingdom. In UK practice, it may be considered particularly in chronic, recurrent or treatment-resistant otitis externa.
Cases may be missed because symptoms overlap with bacterial otitis externa and inflammatory ear conditions. A patient may be treated repeatedly with antibacterial or steroid-containing ear drops before fungal infection is considered. In some cases, antibacterial treatment may suppress bacteria while allowing fungi to overgrow.
A 2025 systematic review highlighted increasing use of molecular methods for species identification, although many published studies still rely primarily on microscopy and culture.
Causative Aspergillus species
Older articles often refer to Aspergillus niger as the dominant Aspergillus species in otomycosis. This remains a useful clinical shorthand, but it is no longer the whole story. Modern molecular identification has shown that black Aspergillus isolates are a complex group and may include species such as Aspergillus tubingensis and other members of the Aspergillus niger complex.
Reported Aspergillus species in otomycosis and fungal otitis externa include:
- Aspergillus niger complex, including related black Aspergillus species
- Aspergillus tubingensis
- Aspergillus flavus
- Aspergillus fumigatus
- Aspergillus terreus complex, reported occasionally in superficial infection series but apparently less common than the Aspergillus niger complex or Aspergillus flavus
Clinical relevance: species-level identification is not always needed for straightforward cases that respond to topical treatment. It becomes more important in recurrent, invasive, immunocompromised or treatment-resistant infection, or where systemic antifungal treatment is being considered.
Risk factors
Otomycosis usually develops when the normal protective environment of the ear canal is disrupted. Important risk factors include:
- warm, humid or dusty environments
- frequent swimming or repeated water exposure
- use of cotton buds, ear picking or other trauma to the ear canal
- previous or repeated antibacterial ear drops
- topical steroid use in the ear
- hearing aids, ear plugs or occlusive moulds
- excess wax, retained debris or foreign material
- chronic otitis externa or chronic otitis media
- previous ear surgery or mastoid cavity
- tympanic membrane perforation
- diabetes, especially if poorly controlled
- immunosuppression, including chemotherapy, transplant medicines, prolonged high-dose corticosteroids and some biological therapies
- skin conditions affecting the ear canal, such as eczema or seborrhoeic dermatitis
Plain-English summary: fungi grow more easily when the ear canal is damp, damaged, blocked, repeatedly treated with antibiotics, or when a person’s immune defences are reduced.
Symptoms and clinical features
Symptoms vary. Some patients have mild itching and fullness, while others have marked discomfort, discharge or hearing loss. Common symptoms include:
- itching in the ear
- ear fullness or blockage
- discharge from the ear
- reduced hearing, often due to debris blocking the canal
- ear discomfort or pain
- tinnitus or ringing in the ear
- scaling, inflammation or visible debris in the ear canal
Severe pain, persistent night pain, swelling around the ear, tenderness or swelling over the mastoid bone behind the ear, fever, persistent or severe dizziness, facial weakness, severe headache, cranial nerve symptoms or symptoms in a person with diabetes or immunosuppression should raise concern for more serious disease.
Sudden hearing loss should be treated as a medical emergency and assessed urgently, regardless of whether otomycosis is suspected.
Diagnosis
Clinical examination
Diagnosis is often suspected by otoscopic or microscopic examination of the ear canal. Typical findings may include fungal debris, spores, hyphae, wet or dry masses, inflammation, scaling, discharge and obstruction. Black, grey, white, yellow-green or fluffy material may be seen, but visual appearance does not reliably identify the species.
Assessment should include:
- extent of external canal inflammation
- presence of fungal debris or discharge
- degree of canal obstruction
- condition of the tympanic membrane
- evidence of perforation, grommets, mastoid cavity or prior surgery
- features suggesting bacterial co-infection
- signs of spread beyond the external canal
Microscopy and fungal culture
Microscopy can demonstrate fungal hyphae or yeast forms. Culture can identify whether Aspergillus, Candida or another fungus is present. Bacterial culture may also be useful if mixed infection is suspected.
Culture is especially helpful when disease is recurrent, severe, atypical, invasive, not responding to standard treatment, or occurring in a person with diabetes, immunosuppression or previous ear surgery.
Molecular identification
Molecular methods can identify Aspergillus species more accurately than morphology alone. This matters because older culture-based reports may have grouped several black Aspergillus species under Aspergillus niger. Molecular identification may also help in epidemiological studies and difficult clinical cases.
For routine mild otomycosis, molecular identification is not always necessary. For persistent, recurrent or invasive disease, species-level identification and antifungal susceptibility testing may help guide treatment.
Antifungal susceptibility testing
Antifungal susceptibility testing is not required for every simple case. It should be considered when there is treatment failure, recurrent disease, unusual species, invasive infection or planned systemic antifungal therapy. Susceptibility patterns may vary between Aspergillus species, although resistance testing is not routinely required for uncomplicated superficial disease.
When to consider imaging
Imaging is not needed for uncomplicated superficial otomycosis. It may be required if there is concern about necrotising external otitis, skull base osteomyelitis, mastoid involvement, middle ear extension, cranial nerve involvement or deep tissue spread. Imaging decisions should be made by ear, nose and throat, infectious diseases, radiology and microbiology or mycology specialists as appropriate.
Differential diagnosis
Conditions that can resemble Aspergillus otomycosis include:
- bacterial otitis externa
- chronic otitis externa
- eczema or dermatitis of the ear canal
- impacted wax
- foreign body
- chronic suppurative otitis media
- cholesteatoma
- otitis media with perforation
- necrotising external otitis
- malignancy of the external canal or temporal bone, rarely
Failure to respond to usual antibacterial treatment should prompt reconsideration of the diagnosis rather than repeated courses of the same treatment.
Treatment principles
Treatment depends on severity, tympanic membrane status, immune status, recurrence, species where known, and whether infection is limited to the outer ear canal. Local ear, nose and throat practice and local antimicrobial guidance should be followed.
1. Aural toilet and debridement
Careful cleaning of the ear canal is central to management. Fungal debris can block the canal, protect organisms from topical treatment and contribute to hearing loss. Aural toilet, often using microsuction or careful debridement, is usually best performed by a trained clinician using appropriate equipment, especially if the canal is swollen, painful, obstructed, or if the tympanic membrane cannot be seen.
Patients should not attempt deep cleaning with cotton buds, hair grips, ear candles or improvised tools. These can damage the ear canal, push debris deeper, worsen inflammation or perforate the eardrum.
Ear irrigation is not usually the preferred approach for suspected otomycosis, because retained moisture may encourage fungal growth and because irrigation may be unsafe if there is tympanic membrane perforation, grommets or previous ear surgery.
2. Topical antifungal treatment
Most uncomplicated otomycosis is treated with topical antifungal therapy after cleaning. Reported agents include clotrimazole, miconazole, nystatin, ciclopirox and other locally used preparations. Different countries and ear, nose and throat services use different formulations, and the evidence does not clearly establish one universally superior topical agent for all cases.
Choice of topical treatment should consider:
- likely organism: mould versus yeast
- whether the tympanic membrane is intact
- previous ear surgery, mastoid cavity or grommets
- local formulary and ear, nose and throat practice
- potential ototoxicity
- patient tolerance and adherence
- whether the canal needs repeat cleaning
3. Tympanic membrane safety
Assessment of the eardrum is important. Some topical agents, antiseptics, acidic preparations or combination drops may be unsafe if the tympanic membrane is perforated or if there are grommets, a mastoid cavity or previous ear surgery. If the eardrum cannot be visualised, treatment should be chosen cautiously and specialist ear, nose and throat advice may be needed.
Important safety point
Patients should not put unprescribed antifungal, antiseptic, acidic, oil-based or herbal preparations into the ear. This is especially important if there is discharge, severe pain, previous ear surgery, grommets, suspected perforated eardrum, sudden hearing loss, dizziness or facial weakness.
4. Mixed bacterial and fungal infection
Mixed infection can occur. If bacterial infection is suspected, bacterial culture and targeted antibacterial treatment may be needed. However, repeated broad-spectrum antibacterial drops without reassessment may encourage fungal overgrowth and delay recognition of otomycosis.
5. Hearing aids, earmoulds and ear plugs
Hearing aids, earmoulds and ear plugs can trap moisture and debris in the ear canal. They may also act as a continuing source of irritation or contamination if not cleaned properly. In recurrent otomycosis, hearing aids and moulds should be reviewed, cleaned according to manufacturer guidance and, where appropriate, assessed by audiology or ear, nose and throat services.
6. Diabetes and immune suppression
People with diabetes or significant immune suppression need particular care, because severe or invasive external ear infection is more likely in these groups. Optimising glycaemic control may help reduce the risk of severe or recurrent infection. Clinicians should consider whether persistent or severe otitis externa in a person with diabetes could represent necrotising external otitis.
7. Systemic antifungal treatment
Systemic antifungal treatment is not usually required for uncomplicated superficial otomycosis. It may be considered in selected situations, including:
- invasive or necrotising external otitis
- extension into the middle ear, mastoid, skull base or surrounding tissues
- severe infection in an immunocompromised patient
- persistent disease where topical therapy is not possible, unsafe or ineffective
- cases requiring multidisciplinary ear, nose and throat, infectious diseases and mycology input
Systemic antifungal choice should be guided by species identification, susceptibility testing, site and extent of infection, drug interactions, renal and liver function, and local specialist advice. Azole antifungals such as itraconazole, voriconazole, posaconazole and isavuconazole have important drug interactions and monitoring requirements.
Recurrent or treatment-resistant otomycosis
Recurrent otomycosis is common in some series. Recurrence does not always mean that the original treatment was wrong; it may reflect ongoing risk factors or incomplete clearance of debris.
When otomycosis recurs or fails to respond, clinicians should reassess:
- Was the ear canal adequately cleaned?
- Can the tympanic membrane be seen?
- Is there perforation, chronic otitis media or mastoid cavity disease?
- Is there a hearing aid mould, ear plug or foreign body contributing?
- Is the patient using cotton buds or self-cleaning the ear?
- Is there persistent water exposure?
- Is there eczema, dermatitis or another inflammatory ear condition?
- Is there mixed bacterial and fungal infection?
- Has microscopy or culture confirmed the organism?
- Is species-level identification or susceptibility testing needed?
- Is the patient diabetic or immunocompromised?
- Is there severe pain, mastoid tenderness or evidence of deeper spread?
Invasive Aspergillus ear infection and necrotising external otitis
Most Aspergillus otomycosis is superficial. However, fungal infection of the external ear can rarely become invasive, particularly in people with diabetes, immunosuppression, severe chronic ear disease or previous ear surgery.
Necrotising external otitis, historically called malignant external otitis, is a severe infection that may involve soft tissues, cartilage, temporal bone or skull base. It is most often bacterial, especially due to Pseudomonas aeruginosa, but fungal cases including Aspergillus and Candida are reported. Fungal necrotising external otitis can be difficult to diagnose and may require prolonged treatment.
Features that should raise concern include:
- severe, persistent or worsening ear pain, especially at night
- pain out of proportion to examination findings
- persistent discharge despite appropriate treatment
- granulation tissue in the ear canal
- facial weakness or other cranial nerve symptoms
- persistent, severe or worsening dizziness, particularly with severe pain, hearing loss or neurological symptoms
- severe headache or neurological symptoms
- swelling, redness or cellulitis around the ear
- tenderness, swelling or redness over the mastoid bone behind the ear
- diabetes, especially if poorly controlled
- immunosuppression
- evidence of mastoid, middle ear or skull base involvement
Suspected invasive or necrotising disease needs urgent ear, nose and throat assessment, microbiological sampling, imaging and specialist antimicrobial or antifungal planning. This is not a condition for self-treatment.
Practical advice for patients and expert patients
Patients can support recovery by protecting the ear canal while treatment is underway. Advice should be individualised by the treating clinician, but common measures include:
- keep the affected ear dry unless advised otherwise
- avoid swimming until cleared by a clinician
- do not use cotton buds or insert objects into the ear
- use prescribed drops exactly as directed
- attend follow-up if symptoms persist, because repeat cleaning may be needed
- tell the clinician about diabetes, immune problems, steroid use, biological therapies, chemotherapy, transplant medicines or previous ear surgery
- ask whether hearing aids, earmoulds or ear plugs need cleaning or review
- report severe pain, dizziness, facial weakness, worsening hearing loss or persistent discharge urgently
Important: online images of invasive aspergillosis can be frightening and often do not represent ordinary otomycosis. Most Aspergillus ear infections are local infections of the outer ear canal. The key is proper assessment, safe cleaning and appropriate treatment.
Frequently asked questions
Is Aspergillus otomycosis rare?
It depends on the setting. Otomycosis is common in some warm and humid regions but is less commonly recognised in many UK clinics. Aspergillus otomycosis may be unfamiliar to clinicians who do not often see fungal ear disease.
Is it the same as invasive aspergillosis?
Usually, no. Most Aspergillus otomycosis is a superficial infection of the outer ear canal. Invasive disease is rare but important, especially in people with diabetes, immunosuppression, severe pain or persistent infection.
Can an ear infection cause symptoms elsewhere in the body?
Otomycosis itself would not usually cause breathlessness, chest symptoms or systemic illness. If a person with suspected otomycosis is also breathless, has chest pain, fever, low oxygen levels or feels very unwell, those symptoms should be assessed separately and promptly.
Can it affect hearing?
Yes. Hearing may be reduced if the ear canal is blocked by fungal debris, discharge or swelling. Hearing often improves when the canal is cleaned and inflammation settles. Sudden hearing loss should be treated as a medical emergency and assessed urgently.
Should every case be cultured?
Not necessarily. Straightforward cases may be treated clinically. Culture and microscopy are more useful when symptoms are recurrent, severe, atypical, treatment-resistant, associated with perforation or surgery, or occur in an immunocompromised patient.
Are antifungal ear drops enough?
Often, topical treatment is effective, but drops may not work well if the ear canal is blocked with debris. Cleaning the canal is often as important as the antifungal medicine itself.
Can patients buy something and treat it themselves?
This is not recommended. Ear symptoms can have several causes, and some substances may be unsafe if the eardrum is perforated. Patients should seek clinical assessment before putting unprescribed antifungal, antiseptic, acidic, herbal or oil-based preparations into the ear.
Why does otomycosis come back?
Recurrence can happen if the canal remains damp, debris persists, the ear is repeatedly traumatised, a hearing aid mould traps moisture, eczema is present, antibiotics are repeatedly used, or an underlying condition such as diabetes or immune suppression is not recognised.
When to seek urgent medical help
Patients should seek urgent medical advice if they have:
- severe or worsening ear pain
- pain that wakes them at night
- swelling, redness or tenderness around the ear
- tenderness, swelling or redness over the mastoid bone behind the ear
- persistent discharge despite treatment
- sudden hearing loss or rapidly worsening hearing
- persistent, severe or worsening dizziness
- severe headache or vomiting
- facial weakness or changes in facial movement
- confusion, fever or feeling very unwell
- diabetes, immune suppression or recent chemotherapy or transplant treatment with ear infection symptoms
- previous ear surgery, grommets or known eardrum perforation with new discharge or pain
These symptoms do not prove invasive infection, but they should be assessed promptly.
Evidence gaps and uncertainty
The evidence base for otomycosis is improving but remains limited. Many studies are single-centre observational series from regions where otomycosis is more common. Treatment studies vary in diagnostic criteria, topical agents, follow-up duration and whether cleaning was standardised. There is no single universally accepted treatment regimen for all cases.
Important gaps include:
- limited high-quality randomised trials comparing topical antifungal treatments
- variable reporting of tympanic membrane status and previous ear surgery
- inconsistent use of fungal culture, molecular identification and susceptibility testing
- limited data on recurrence prevention
- limited evidence specific to UK practice
- uncertainty about the best systemic antifungal approach in rare invasive cases
For these reasons, this article should support but not replace specialist clinical judgement.
References
- Nazari T, Peymaeei F, Ghazi Mirsaid R, et al. Otomycosis: a systematic review and meta-analysis of prevalence and causative agents in the era of molecular diagnostics. BMC Infectious Diseases. 2025;25(1). doi: 10.1186/s12879-025-10954-y. PubMed
- Bojanović M, Stalević M, Arsić-Arsenijević V, et al. Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review. Journal of Fungi. 2023;9(6):662. doi: 10.3390/jof9060662. PubMed
- Wiegand S, Berner R, Schneider A, Lundershausen E, Dietz A. Otitis Externa: Investigation and Evidence-Based Treatment. Deutsches Ärzteblatt International. 2019. doi: 10.3238/arztebl.2019.0224. PubMed
- Koltsidopoulos P, Skoulakis C. Otomycosis With Tympanic Membrane Perforation: A Review of the Literature. Ear, Nose & Throat Journal. 2019;99(8):518–521. doi: 10.1177/0145561319851499. PubMed
- Mtibaa L, Halwani C, El Hamdi M, et al. A retrospective study of 43 cases of fungal malignant external otitis. Pan African Medical Journal. 2022;41. doi: 10.11604/pamj.2022.41.287.29585. PubMed
- Szigeti G, Sedaghati E, Mahmoudabadi AZ, et al. Species assignment and antifungal susceptibilities of black aspergilli recovered from otomycosis cases in Iran. Mycoses. 2011;55(4):333–338. doi: 10.1111/j.1439-0507.2011.02103.x. PubMed
- Jimenez-Garcia L, Celis-Aguilar E, Díaz-Pavón G, et al. Efficacy of topical clotrimazole vs. topical tolnaftate in the treatment of otomycosis: a randomized controlled clinical trial. Brazilian Journal of Otorhinolaryngology. 2020;86(3):300–307. doi: 10.1016/j.bjorl.2018.12.007. PubMed
- Mofatteh MR, Naseripour Yazdi Z, Yousefi M, et al. Comparison of the recovery rate of otomycosis using betadine and clotrimazole topical treatment. Brazilian Journal of Otorhinolaryngology. 2018;84(4):404–409. doi: 10.1016/j.bjorl.2017.04.004. PubMed
- Mao C, Li A, Hu J, et al. Efficient and accurate diagnosis of otomycosis using an ensemble deep-learning model. Frontiers in Molecular Biosciences. 2022;9:951432. doi: 10.3389/fmolb.2022.951432. PubMed
- Feng Y, Zhang Z, Fang W, et al. Profiling Drug Susceptibility and Species Identification of Aspergillus Isolates From Patients With Superficial Infection. Mycoses. 2025;68(4). doi: 10.1111/myc.70059. PubMed
- NICE Clinical Knowledge Summaries. Otitis externa. NICE CKS
Author and review information
Article type: Clinical and expert-patient evidence update
Intended audience: Ear, nose and throat clinicians, infectious diseases specialists, medical mycologists, general practitioners, specialist nurses, patients and carers seeking detailed information.
Last reviewed: June 2026
Review note: This article is for information and education. It should not replace assessment by a qualified clinician. Treatment choices depend on examination findings, tympanic membrane status, culture results where available, medical history, immune status and local prescribing guidance.
```
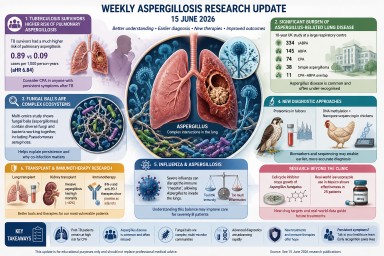
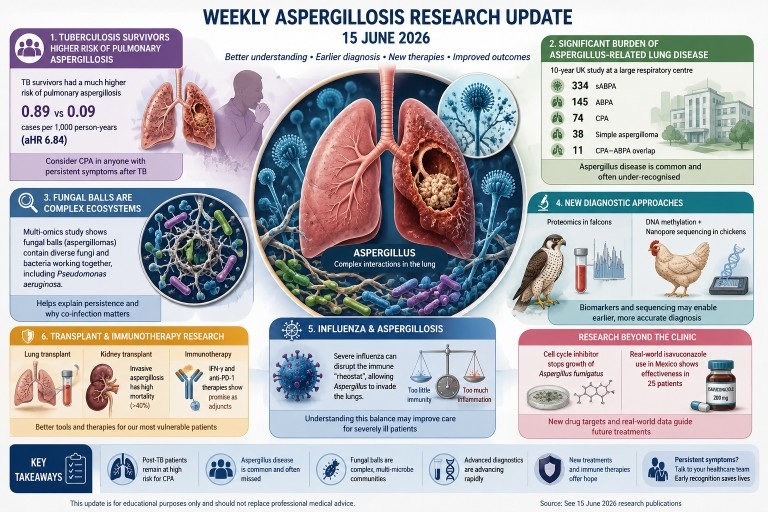
Weekly Aspergillosis Research Update – 15 June 2026
Key Points
- A large population study confirms that people who have survived tuberculosis (TB) have a substantially increased risk of developing chronic pulmonary aspergillosis (CPA).
- New UK data highlight the significant burden of Aspergillus-related chronic lung diseases in routine respiratory care.
- Research suggests that fungal balls (aspergillomas) are complex microbial ecosystems rather than simple collections of fungal growth.
- New diagnostic approaches using proteomics, DNA methylation and sequencing continue to show promise.
- Several studies explore improved diagnosis and treatment of aspergillosis in transplant recipients and other highly vulnerable patients.
Contents
- Tuberculosis Survivors and Aspergillosis Risk
- New UK Data on Aspergillus-Related Lung Disease
- Understanding Fungal Balls
- New Diagnostic Technologies
- Influenza-Associated Pulmonary Aspergillosis
- Transplantation and Immunotherapy Research
- What Does This Mean for Patients?
- References
Tuberculosis Survivors Face a Much Higher Risk of Pulmonary Aspergillosis
One of the most important studies published this week examined the long-term risk of pulmonary aspergillosis among people who have previously had tuberculosis (TB).
Researchers analysed nationwide health data and found that pulmonary aspergillosis occurred almost ten times more frequently in TB survivors than in matched controls. The incidence was 0.89 cases per 1,000 person-years among TB survivors compared with 0.09 cases per 1,000 person-years in the control group.
After adjusting for other risk factors, individuals with a history of TB remained nearly seven times more likely to develop pulmonary aspergillosis.
This finding reinforces a growing body of evidence showing that chronic pulmonary aspergillosis (CPA) is an important long-term complication of tuberculosis. Residual lung cavities and structural lung damage may provide an environment in which Aspergillus can establish chronic infection.
- Zo S, Lee KN, Han K, et al. Risk of Pulmonary Aspergillosis in Tuberculosis Survivors: A Nationwide Population-based Study.
International Journal of Antimicrobial Agents. 2026.
Patients who have previously had tuberculosis and continue to experience symptoms such as chronic cough, breathlessness, fatigue, weight loss or coughing up blood should discuss the possibility of CPA with their healthcare team.
New UK Data Highlight the Burden of Aspergillus-Related Lung Disease
A 10-year retrospective study from Imperial College Healthcare NHS Trust provides valuable insight into the scale of Aspergillus-related lung disease seen within a large UK respiratory service.
The researchers identified:
- 334 patients with serological allergic bronchopulmonary aspergillosis (sABPA)
- 145 patients with allergic bronchopulmonary aspergillosis (ABPA)
- 74 patients with chronic pulmonary aspergillosis (CPA)
- 38 patients with simple aspergilloma
- 11 patients with CPA-ABPA overlap disease
These figures demonstrate that Aspergillus-related conditions are encountered across a broad range of respiratory clinics and are not confined to specialist fungal centres.
- Venkatesan T, Nagi N, Nwankwo L, et al. Describing the Burden and Characteristics of Aspergillus-related Chronic Lung Disease at Imperial College Healthcare Trust: a 10-year Retrospective Study.
BMJ Open Respiratory Research. 2026.
The study highlights the importance of awareness among respiratory specialists, general physicians and primary care clinicians. Early recognition remains one of the biggest challenges in Aspergillus-related lung disease.
Fungal Balls Are More Complex Than Previously Thought
A fascinating multi-omics study examined fungal balls (aspergillomas) removed from patients with chronic pulmonary aspergillosis.
Traditionally, aspergillomas have been viewed as relatively simple accumulations of fungal material within pre-existing lung cavities. However, this research paints a much more complex picture.
The investigators found evidence that aspergillomas function as resilient microbial ecosystems involving interactions between Aspergillus species and bacteria, including organisms such as Pseudomonas aeruginosa.
The fungal communities also showed metabolic adaptations that may help them survive within the challenging environment of the lung cavity.
These findings may help explain why some aspergillomas remain difficult to eradicate and why bacterial co-infections can sometimes influence symptoms and treatment outcomes.
New Diagnostic Technologies Continue to Advance
Two veterinary studies published this week demonstrate the rapid development of advanced fungal diagnostic technologies.
Proteomics in Falcons
Researchers studying aspergillosis in falcons used plasma proteomics to identify potential biomarkers that may allow earlier diagnosis of infection.
Current diagnostic approaches often detect disease only after significant progression. The identification of blood-based biomarkers could eventually improve earlier detection and monitoring.
- Vieu S, Lozano C, Azmanis P, et al. Falcon Plasma Proteomics to Improve Avian Aspergillosis Diagnosis.
Journal of Proteomics. 2026.
DNA Methylation and Nanopore Sequencing in Chickens
A second study used host cell-free DNA methylation combined with nanopore sequencing to diagnose Aspergillus fumigatus infection in chickens with high accuracy.
Although these studies involve birds, they reflect wider trends in fungal diagnostics, where researchers are increasingly exploring:
- Proteomics
- Cell-free DNA analysis
- Next-generation sequencing
- Machine learning approaches
- Biomarker-based diagnostics
Future human diagnostics may rely less on culture-based testing and more on sophisticated molecular techniques that can identify disease earlier and more accurately.
Influenza and Aspergillosis: Understanding the Immune Response
A review published in Trends in Microbiology explores the mechanisms underlying influenza-associated pulmonary aspergillosis (IAPA).
Over the past decade, clinicians have recognised that severe influenza can predispose some patients to invasive Aspergillus infection.
The review discusses how viral infection can disrupt the delicate balance of immune responses in the lungs, creating conditions that allow Aspergillus to invade tissue.
The authors describe this balance as an inflammatory "rheostat" that regulates protection against infection while avoiding excessive tissue damage.
- Charrier Le Blan M, Biquand E, Briard B. Critical Role of the Inflammatory Rheostat in Influenza-associated Pulmonary Aspergillosis.
Trends in Microbiology. 2026.
While primarily relevant to critically ill hospitalised patients, the work improves our understanding of how viral infections and fungal infections interact.
Transplantation and Immunotherapy Research
Several studies this week focused on patients with severe immune suppression and organ transplantation.
Improved Diagnosis After Lung Transplantation
The GALACTBAS study suggests that galactomannan testing of tracheobronchial aspirates may improve detection of Aspergillus infection in lung transplant recipients.
The findings support the idea that some transplant-associated Aspergillus infections begin within the bronchial tree and may not always be detected early using traditional bronchoalveolar lavage (BAL) samples.
- Monforte A, Martín-Gómez MT, Berastegui C, et al. Diagnostic Value of Galactomannan in Tracheobronchial Aspirate for Aspergillus Infection in Lung Transplant Recipients.
Journal of Clinical Microbiology. 2026.
Kidney Transplant Patients
A prospective multicentre study found that invasive aspergillosis remained one of the most serious fungal complications after kidney transplantation, with mortality exceeding 40%.
Emerging Immunotherapies
Another review evaluated growing evidence supporting the use of immune-enhancing treatments such as:
- Interferon-gamma (IFN-γ)
- Anti-programmed death-1 (anti-PD-1) therapies
These approaches aim to strengthen antifungal immunity alongside standard antifungal treatment in selected patients with severe invasive mould infections.
Although still considered specialist therapies, interest in immunomodulation continues to grow.
What Does This Mean for Patients?
Several themes emerge from this week's publications:
- Previous tuberculosis remains one of the most important risk factors for chronic pulmonary aspergillosis.
- Aspergillus-related lung diseases continue to be under-recognised outside specialist centres.
- Fungal balls are biologically complex and involve interactions between fungi, bacteria and the lung environment.
- Diagnostic technology is advancing rapidly, particularly in biomarker and sequencing-based approaches.
- Research into immune-based treatments continues to expand alongside antifungal drug development.
Although many of these studies are early-stage or aimed primarily at researchers and specialists, together they show a field that is continuing to improve our understanding of how Aspergillus causes disease and how it might be diagnosed and treated more effectively in the future.
When to Seek Medical Advice
Patients with known lung disease should seek medical advice if they experience:
- Persistent or worsening breathlessness
- New or worsening cough
- Unexplained weight loss
- Fatigue that is worsening over time
- Coughing up blood (haemoptysis)
- New chest pain
- Persistent fever or night sweats
Individuals who have previously had tuberculosis should be particularly aware that chronic pulmonary aspergillosis can develop months or years after apparent recovery from TB.
References
- Zo S, Lee KN, Han K, et al. Risk of Pulmonary Aspergillosis in Tuberculosis Survivors: A Nationwide Population-based Study.
International Journal of Antimicrobial Agents. 2026. - Venkatesan T, Nagi N, Nwankwo L, et al. Describing the Burden and Characteristics of Aspergillus-related Chronic Lung Disease at Imperial College Healthcare Trust: a 10-year Retrospective Study.
BMJ Open Respiratory Research. 2026. - Liu C, Ribeiro MM, Yang J, et al. Multi-omics Profiling of Fungal Balls in Chronic Pulmonary Aspergillosis Patients Reveals Microbiome Dynamics and Metabolic Adaptations.
mBio. 2026. - Vieu S, Lozano C, Azmanis P, et al. Falcon Plasma Proteomics to Improve Avian Aspergillosis Diagnosis.
Journal of Proteomics. 2026. - Drag MH, Hvilsom C, Poulsen LL, et al. MethylSense: High Accuracy Machine Learning-Based Diagnostics for Aspergillus fumigatus Infection in Chickens Using Host Cell-free DNA Methylation and Nanopore Sequencing.
Journal of Clinical Microbiology. 2026. - Charrier Le Blan M, Biquand E, Briard B. Critical Role of the Inflammatory Rheostat in Influenza-associated Pulmonary Aspergillosis.
Trends in Microbiology. 2026. - Monforte A, Martín-Gómez MT, Berastegui C, et al. Diagnostic Value of Galactomannan in Tracheobronchial Aspirate for Aspergillus Infection in Lung Transplant Recipients.
Journal of Clinical Microbiology. 2026. - Serris A, Guihot A, Joffre J, et al. Emerging Evidence for Anti-PD-1 and IFN-γ as Adjunctive Immunotherapy in Invasive Mold Infections.
mBio. 2026.
Author: Graham Atherton, National Aspergillosis Centre (NAC)
Clinical Review: National Aspergillosis Centre Clinical Team
Last Reviewed: 15 June 2026
For Patient Education Only: This article is intended for educational purposes and should not replace professional medical advice.
The Hidden Job Nobody Talks About: Living with Chronic Illness
For many people, the hardest part of chronic illness is not always the symptoms. It is the constant work of managing them.
Key Points
- Chronic illness often creates a significant hidden workload.
- Patients manage medications, appointments, prescriptions, side effects, monitoring and healthcare administration.
- Fatigue and brain fog can make this workload even harder.
- Organisation helps, but organisation itself requires effort.
- Technology, pharmacists, medication reviews, family support and patient communities can help reduce the burden.
- Nobody should feel they have failed because they occasionally forget something.
Contents
- The Work Nobody Sees
- The Constant Background Process
- The Hidden Impact of Fatigue
- Grieving the Loss of Simplicity
- The Expert Nobody Wanted to Become
- Building an External Brain
- When Organisation Itself Needs Help
- Practical Ways to Reduce the Mental Load
- The Annual Medication MOT
- You Do Not Have to Carry It All Alone
- Final Thoughts
The Work Nobody Sees
When people think about chronic illness, they usually think about symptoms.
Breathlessness.
Pain.
Fatigue.
Cough.
Hospital appointments.
Medication.
These are certainly part of the picture.
But many patients would argue that another challenge receives far less attention.
The work.
Not paid work.
The hidden work of being a patient.
For many people, living with a chronic illness means becoming the organiser, administrator, coordinator and decision-maker for an ongoing healthcare programme.
There are prescriptions to order.
Appointments to attend.
Letters to understand.
Blood tests to arrange.
Side effects to monitor.
Questions to remember.
Symptoms to interpret.
Forms to complete.
Information to absorb.
And unlike most jobs, there are no weekends off.
Many patients are not only managing an illness. They are managing an entire healthcare programme.
The Constant Background Process
One patient recently described chronic illness as being like a computer running a programme permanently in the background.
Even on good days, the process never completely switches off.
Questions quietly run through the mind:
- Do I have enough medication?
- When is my next appointment?
- Should I order my prescription?
- Is this symptom normal?
- Is this a side effect?
- Have I forgotten something important?
Most healthy people can devote their attention entirely to daily life.
Many patients are simultaneously running this constant background process.
That process consumes energy.
It consumes concentration.
And over time it can become exhausting.
The work of being ill can sometimes feel almost as exhausting as the illness itself.
The Hidden Impact of Fatigue
Fatigue affects much more than physical energy.
It can affect:
- Memory.
- Concentration.
- Planning.
- Organisation.
- Decision-making.
This creates a difficult cycle.
The more tired someone becomes, the harder it is to stay organised.
The harder it is to stay organised, the easier it becomes to miss a prescription, forget an appointment or overlook an important detail.
That can create stress.
Stress itself is tiring.
Many patients eventually discover that they are not simply carrying the burden of their illness.
They are carrying the burden of managing the illness.
This is not weakness.
It is a normal human response to a sustained workload.
Grieving the Loss of Simplicity
Many people are not only grieving the loss of health.
They are grieving the loss of simplicity.
Remember when you could:
- Go away for the weekend without checking medication supplies?
- Accept invitations without calculating energy levels?
- Spend a day outdoors without thinking about medication side effects?
- Plan months ahead without wondering how you might feel?
Spontaneity often gives way to planning.
Simple decisions become calculations.
Many people find themselves missing the ease and simplicity they once took for granted.
That feeling is entirely understandable.
The Expert Nobody Wanted to Become
One of the remarkable things about people living with chronic illness is how much they learn.
Over time, patients often become experts in:
- Medications.
- Blood tests.
- Side effects.
- Hospital systems.
- Insurance.
- Benefits.
- Referral pathways.
Most never intended to acquire this knowledge.
They learned because circumstances required it.
As one patient put it:
"I never applied for the job, but somehow I became the project manager for my illness."
Many readers will recognise that immediately.
A person with aspergillosis may spend five minutes taking medication.
They may spend an hour thinking about medication.
The burden is often not the tablet itself.
The burden is remembering the tablet, remembering to reorder the tablet, remembering what it interacts with, remembering the blood test, remembering the side effects and remembering what to do if something changes.
Building an External Brain
One lesson many patients learn is that memory alone is not enough.
This is especially true when fatigue, pain, poor sleep or brain fog are present.
Successful long-term management often depends on creating systems that do some of the remembering for us.
Examples include:
- Paper diaries.
- Calendars.
- Whiteboards.
- Medication reminder apps.
- Smartphone reminders.
- Alexa or Siri reminders.
- Weekly pill organisers.
- Shared family calendars.
One patient described this as creating an "external brain".
The exact system matters less than the principle behind it.
The aim is not to remember everything. The aim is to build systems that do some of the remembering for you.
Technology Can Help
Smart speakers such as Amazon Alexa and voice assistants such as Apple Siri can act as simple reminder systems.
They can be used for:
- Medication reminders.
- Prescription reminders.
- Appointment reminders.
- Weekly health checks.
- Shopping lists.
- Clinic preparation.
For example:
"Alexa, remind me every Sunday evening to check my medication supplies."
Or:
"Hey Siri, remind me every first Monday of the month to order my repeat prescriptions."
For many patients these systems reduce stress and make it less likely that important tasks will be forgotten.
When Organisation Itself Needs Help
People are often told to "stay organised".
It is good advice.
But it overlooks something important.
Organisation itself requires effort.
Creating reminders.
Maintaining calendars.
Sorting medication.
Reading letters.
Booking appointments.
Ordering prescriptions.
All of these tasks require energy.
For someone already dealing with fatigue, breathlessness, pain or brain fog, even staying organised can sometimes feel overwhelming.
This is why support matters.
Support is not always about physical assistance.
Sometimes it is about sharing the responsibility of remembering.
A partner who reminds you about an appointment.
A family member who collects a prescription.
A friend who helps complete a form.
A pharmacist who helps simplify medication schedules.
These small acts can remove a surprising amount of pressure.
Organisation helps. But sometimes organisation needs help too.
Practical Ways to Reduce the Mental Load
Many patients find it helpful to:
- Schedule a weekly "health admin" session.
- Use a diary, whiteboard or calendar.
- Set medication reminders.
- Use a weekly pill organiser.
- Ask about pharmacy reminder services.
- Consider medication packaging systems.
- Share calendars with family members.
- Keep a running list of questions for clinic appointments.
The goal is not perfection.
The goal is to make life easier.
The Annual Medication MOT
Cars receive regular servicing.
Computers receive updates.
Financial plans are reviewed.
Yet many people take the same collection of medications for years without anyone stepping back and looking at the whole picture.
A structured medication review or polypharmacy review can help answer questions such as:
- Do I still need all these medicines?
- Could any side effects be contributing to symptoms?
- Are there interactions?
- Can the schedule be simplified?
- Is every medication still serving a clear purpose?
Sometimes the most useful prescription is not a new medication.
It is a review of the medications already being taken.
Sometimes the most useful prescription is not a new medication, but a review of the medications already being taken.
You Do Not Have to Carry It All Alone
Many of us value independence.
That is understandable.
However, there is a difference between independence and carrying every burden alone.
Help may come from:
- Pharmacists.
- Occupational therapists.
- Family.
- Friends.
- Carers.
- Charities such as Age UK.
- Patient support groups.
Often the most valuable support is not somebody doing something for us.
It is somebody helping us remember.
A second pair of eyes.
A second memory.
A second person asking:
"Have you got everything you need for next week?"
Final Thoughts
Living with a chronic illness is often described in terms of symptoms, test results and treatments.
But behind every clinic letter is a person carrying a mental checklist that never completely disappears.
The medications.
The appointments.
The prescriptions.
The side effects.
The blood tests.
The questions.
The worries.
The constant balancing act.
If you sometimes feel tired not only from your illness, but from the work of managing it, that feeling is understandable.
It may simply be a reflection of how much you are carrying.
No patient should feel they have failed because they forgot something, ran out of medication, missed a reminder or needed support.
Managing chronic illness is complex.
Nobody does it perfectly.
The aim is not perfection.
The aim is to build enough support, systems and kindness around ourselves that daily life becomes a little easier to manage.
The goal is not to prove that you can manage everything alone.
The goal is to build enough support around yourself that life becomes easier, safer and more enjoyable.
Author: National Aspergillosis Centre Patient Support Team
Last reviewed: June 2026
Medical disclaimer: This article provides general information and support. It should not replace advice from your own doctor, pharmacist, nurse or specialist team.
Useful sources and further reading
-
Suggested Internal Links
National Aspergillosis Centre Patient Support
https://aspergillosis.org/patients/Living with Aspergillosis
https://aspergillosis.org/living-with-aspergillosis/Chronic Pulmonary Aspergillosis (CPA)
https://aspergillosis.org/chronic-pulmonary-aspergillosis/Allergic Bronchopulmonary Aspergillosis (ABPA)
https://aspergillosis.org/allergic-bronchopulmonary-aspergillosis-abpa/Aspergillus Bronchitis
https://aspergillosis.org/aspergillus-bronchitis/Understanding Fatigue in Chronic Illness
Medication Information Hub
https://aspergillosis.org/antifungal-drugs/Voriconazole Information
https://aspergillosis.org/voriconazole/Itraconazole Information
https://aspergillosis.org/itraconazole/Posaconazole Information
https://aspergillosis.org/posaconazole/Isavuconazole Information
https://aspergillosis.org/isavuconazole/Adrenal Insufficiency and Steroid Information
National Aspergillosis Centre Online Support Meetings
https://aspergillosis.org/patient-meetings/The Aspergillosis Trust
https://aspergillosistrust.org/
Suggested External Links
Age UK
https://www.ageuk.org.uk/Carers UK
https://www.carersuk.org/NHS Structured Medication Reviews
https://www.england.nhs.uk/primary-care/pharmacy/smr/NHS Repeat Prescriptions
https://www.nhs.uk/nhs-services/prescriptions/

More Than a Referral Centre: How the National Aspergillosis Centre Supports Patients and Healthcare Professionals Across the UK

Combining specialist clinical care, diagnostics, multidisciplinary expertise, patient support, education and research to improve outcomes for people living with Chronic Pulmonary Aspergillosis.
The National Aspergillosis Centre (NAC) was established by NHS England to provide highly specialised care for people living with Chronic Pulmonary Aspergillosis (CPA), a serious fungal lung disease that can develop in patients with pre-existing respiratory conditions.
Over the last sixteen years the service has evolved into much more than a referral clinic. Today, NAC combines specialist clinical care, advanced diagnostics, multidisciplinary expertise, patient support, education and research, working alongside local healthcare teams throughout the UK.
Many clinicians are familiar with NAC as a specialist referral service. However, fewer may be aware of the breadth of support available through the centre, including specialist multidisciplinary team discussions, diagnostic expertise, physiotherapy, nursing support, pharmacy services, patient education programmes and nationally recognised fungal diagnostics.
This article provides an overview of how NAC supports both patients and healthcare professionals in the diagnosis and management of Chronic Pulmonary Aspergillosis.
"The National Aspergillosis Centre exists not only to care for patients with Chronic Pulmonary Aspergillosis, but also to support healthcare professionals throughout the UK in diagnosing and managing this complex condition."
Contents
- Why specialist support matters
- What does NAC do?
- Working with local teams
- Benefits for patients
- Benefits for healthcare professionals
- Patient support and education
- Research, education and innovation
- Why awareness still matters
- Further resources
- Working together
Why specialist support matters
Chronic Pulmonary Aspergillosis (CPA) is a serious fungal lung disease that can develop in people with pre-existing respiratory conditions including bronchiectasis, Chronic Obstructive Pulmonary Disease (COPD), previous tuberculosis, sarcoidosis and other structural lung diseases.
Patients may present with chronic cough, breathlessness, fatigue, weight loss, recurrent chest infections or haemoptysis. These symptoms frequently overlap with more common respiratory conditions, making diagnosis challenging.
CPA remains a relatively uncommon disease and many clinicians may encounter only a small number of cases during their careers. As a result, specialist support can be valuable when diagnosis is uncertain, investigations are difficult to interpret or treatment becomes complex.
The National Aspergillosis Centre was established to provide that support.
What does the National Aspergillosis Centre do?
NAC is commissioned by NHS England to provide highly specialised care for patients with Chronic Pulmonary Aspergillosis.
The service supports patients through:
- Specialist assessment and diagnosis
- Multidisciplinary review of complex cases
- Long-term disease monitoring
- Antifungal treatment planning and optimisation
- Therapeutic drug monitoring
- Assessment and management of antifungal resistance
- Management of drug interactions and adverse effects
- Specialist physiotherapy support
- Specialist nursing support
- Access to clinical research and trials
Every new CPA diagnosis is reviewed within a specialist multidisciplinary team, helping to ensure a consistent and evidence-based approach to diagnosis and management.
NAC in 2023–24
- 209 referrals assessed for aspergillosis
- 101 new confirmed CPA diagnoses
- 311 patients under active specialist follow-up
- 71 external cases discussed through the National MDT
- 56 remote advice and guidance consultations
Working with local teams
One of the most common misconceptions about referral is that patients must transfer all of their care to Manchester.
In reality, NAC operates primarily through a shared-care model.
Wherever possible, investigations, imaging, monitoring and routine care are organised locally, with NAC providing specialist input and treatment recommendations. This approach allows patients to benefit from national expertise while remaining close to home.
The service also supports healthcare professionals through remote advice, specialist consultation and participation in the National Multidisciplinary Team (MDT) meeting.
For many clinicians, discussing a case through the MDT can help clarify diagnosis, identify additional investigations and support treatment decisions before or alongside formal referral.
Benefits for patients
Patients referred to NAC gain access to one of the world's largest specialist CPA services.
Benefits include:
- Specialist review by clinicians with extensive experience in fungal lung disease
- Diagnostic clarification and confirmation
- Optimisation of antifungal therapy
- Management of treatment-related complications
- Access to specialist physiotherapy and nursing support
- Educational resources and self-management support
- Opportunities to participate in research
For many patients, specialist review provides reassurance, a clearer understanding of their condition and confidence in their treatment plan.
Benefits for healthcare professionals
The National Aspergillosis Centre exists not only to support patients, but also to support healthcare professionals.
Referral or specialist discussion may be particularly useful when:
- The diagnosis remains uncertain
- Radiological findings are difficult to interpret
- Patients are not responding as expected
- Antifungal toxicity develops
- Resistance is suspected
- A specialist second opinion would be valuable
Clinicians also gain access to expertise in therapeutic drug monitoring, antifungal stewardship, complex fungal diagnostics and long-term disease management.
Each referral creates opportunities for shared learning, helping local teams build experience and confidence in recognising and managing aspergillosis.
Patient support and education
One of the most distinctive features of the National Aspergillosis Centre is the support available beyond routine clinical care.
Many patients referred to NAC have experienced a long and sometimes frustrating journey to diagnosis. Symptoms may have been present for months or years before Chronic Pulmonary Aspergillosis is recognised.
Following diagnosis, patients are often faced with an unfamiliar condition and may encounter alarming information online that relates to very different forms of aspergillosis. It is therefore common for patients and families to feel anxious, isolated and uncertain about what the future may hold.
For this reason, patient support forms an important part of the NAC service.
Through the Community, Awareness, Research, Education and Support (CARES) programme, patients have access to:
- Regular patient support meetings
- Educational webinars and presentations
- Health and wellbeing sessions
- Patient newsletters
- Online information resources
- The Aspergillosis Patients and Carers website
- Peer support opportunities
One of the most common comments from newly diagnosed patients is the relief of discovering that they are not facing the condition alone. Meeting others living with aspergillosis and having access to trusted information can make a significant difference to confidence, understanding and long-term self-management.
"For many patients, finding the CARES programme is the moment they realise they are no longer facing aspergillosis on their own."
By combining specialist clinical care with education, support and community, NAC aims to help patients and families feel informed, supported and empowered throughout their journey.
Research, education and innovation
The National Aspergillosis Centre works closely with the Mycology Reference Centre Manchester (MRCM), one of Europe's leading specialist fungal diagnostic laboratories.
Together, NAC and MRCM contribute to:
- Clinical trials of new antifungal therapies
- Development of new diagnostic techniques
- Antifungal resistance surveillance
- National and international clinical guidelines
- Professional education and training
- Patient-centred research
The partnership has been recognised internationally through European Confederation of Medical Mycology (ECMM) Diamond Centre of Excellence status.
This close integration of clinical care, diagnostics, education and research helps ensure that patients benefit from the latest developments in fungal disease management.
Why awareness still matters
Chronic Pulmonary Aspergillosis remains an under-recognised disease worldwide.
Many patients present with symptoms that overlap with more common respiratory conditions such as COPD, bronchiectasis or previous tuberculosis. As a result, diagnosis can sometimes be delayed or missed.
This is not because clinicians are failing. CPA is an uncommon disease that can closely resemble more familiar respiratory conditions.
The role of NAC is therefore not simply to provide specialist treatment, but also to support earlier recognition of CPA through education, diagnostic support and collaborative working with healthcare professionals throughout the UK.
By raising awareness and improving access to specialist expertise, we hope to help more patients receive timely diagnosis, appropriate treatment and long-term support.
Further resources
- Aspergillosis Patients & Carers Website
- Chronic Pulmonary Aspergillosis Information Hub
- Patient Support Resources
- World Aspergillosis Day Resources
- Mycology Reference Centre Manchester
Working together
The National Aspergillosis Centre was established to ensure that patients with Chronic Pulmonary Aspergillosis have access to specialist expertise wherever they live.
Through shared-care working, multidisciplinary collaboration, specialist diagnostics, patient support, education and research, NAC continues to work alongside healthcare professionals throughout the UK to improve outcomes for people living with fungal lung disease.
Whether through referral, multidisciplinary discussion, specialist advice or educational resources, our aim remains the same: helping clinicians diagnose and manage aspergillosis with confidence while ensuring patients receive the support they need.
NAC is more than a referral centre. It is a national resource for patients, clinicians and healthcare services working together to improve the diagnosis and management of Chronic Pulmonary Aspergillosis.

Living Safely with Pets When You Have Aspergillosis

Pets can be an important part of life for many people with aspergillosis. They provide companionship, routine, comfort, and sometimes gentle exercise. For most people, having pets does not mean they need to give them up. The key is understanding where fungal spores are most likely to build up and taking sensible precautions.
Key points
- Most people with aspergillosis do not need to avoid pets altogether.
- The main concern is usually not the animal itself, but dusty or damp materials such as hay, straw, bedding, feed, droppings, compost, and mouldy organic matter.
- Risk increases when bedding is left unchanged, becomes damp, or is disturbed during cleaning.
- People with allergic forms of aspergillosis, such as Allergic Bronchopulmonary Aspergillosis (ABPA), may react to fungal spores as allergens.
- People with Chronic Pulmonary Aspergillosis (CPA) may need to avoid heavy spore exposure because their lungs are already damaged.
- Good pet care, dry bedding, regular cleaning, and sensible respiratory protection can reduce avoidable exposure.
- The emotional and wellbeing benefits of pets can be considerable and should be included in any balanced decision.
Contents
- Why patients worry about pets
- What is the actual risk?
- Situations that may increase exposure
- Different risks in different forms of aspergillosis
- Practical advice for different pets
- Children’s pets and shared responsibility
- The benefits of pets
- Simple risk-reduction checklist
- Common questions
- When to seek medical advice
- Author and review information
- References
Why patients worry about pets
After being diagnosed with aspergillosis, many people start to look carefully at their home, garden, hobbies, and pets. This is understandable. Aspergillus is a mould that is found widely in the environment, and people may worry that a pet, cage, litter tray, hutch, or bedding could be making their lung condition worse.
The first reassurance is important: aspergillosis is not usually caught from pets in the way that some infections can be passed from animals to humans. The main issue is breathing in fungal spores from the environment. These spores are more likely to come from dusty, damp, or decaying organic material than from the animal itself.
A clean dog or cat in the home is very different from cleaning out a damp rabbit hutch, shaking mouldy hay, or disturbing old bedding in a poorly ventilated shed.
What is the actual risk?
The risk is mainly from inhaling airborne fungal spores. Aspergillus spores are very common in the environment. Most people breathe them in without becoming ill. Problems are more likely in people with asthma, cystic fibrosis, chronic lung disease, damaged lungs, or weakened immune systems.
Pet-related exposure is most likely when fungal spores build up in:
- Hay
- Straw
- Wood shavings or paper bedding
- Stored animal feed
- Damp hutches or cages
- Bird droppings
- Chicken coops
- Compost, soil, and rotting vegetation
- Dusty sheds or poorly ventilated outbuildings
The animal itself is usually not the main source of concern. The bigger issue is the environment around the animal, especially if it is damp, dusty, mouldy, or not cleaned regularly.
Situations that may increase exposure
Risk is not the same in every situation. Some pet-related activities are likely to create more airborne dust and spores than others.
| Situation | Likely level of concern | Why it matters |
|---|---|---|
| Living with a clean dog or cat | Low | The animal itself is not usually a major Aspergillus source. |
| Feeding pets from clean, dry food | Low | Low dust exposure if food is stored properly. |
| Changing a clean litter tray regularly | Low to moderate | Dust and odour may irritate airways; dusty litter may be a problem for some. |
| Handling hay for guinea pigs or rabbits | Moderate | Hay can contain fungal spores, especially if damp or poorly stored. |
| Cleaning cages or hutches with damp bedding | Moderate to higher | Disturbing bedding can release dust and spores into the air. |
| Cleaning bird cages or chicken coops | Higher | Droppings, feathers, bedding, and feed dust may build up in enclosed spaces. |
| Using mouldy hay, straw, or feed | Higher | Visible mould suggests fungal growth and avoidable exposure. |
| Cleaning old bedding after it has been neglected | Higher | Accumulated organic waste, dampness, and dust increase exposure when disturbed. |
Different risks in different forms of aspergillosis
Not all aspergillosis conditions carry the same type of risk. The reason for reducing exposure differs depending on the diagnosis.
Allergic Bronchopulmonary Aspergillosis (ABPA)
In Allergic Bronchopulmonary Aspergillosis, the main issue is allergic inflammation. The immune system reacts strongly to Aspergillus. Extra exposure to fungal spores may contribute to asthma symptoms, coughing, wheezing, mucus production, or mucus plugging in some people.
For people with ABPA, pet-related precautions are mainly about reducing exposure to fungal allergens from hay, bedding, damp cages, and dusty animal environments.
Severe Asthma with Fungal Sensitisation (SAFS)
Severe Asthma with Fungal Sensitisation is also an allergic-type condition. The concern is not usually that the pet will cause an infection, but that mould spores and other allergens may worsen asthma symptoms.
Chronic Pulmonary Aspergillosis (CPA)
Chronic Pulmonary Aspergillosis usually occurs in lungs that already have damage, cavities, scarring, bronchiectasis, or previous lung disease. In CPA, the concern is less about allergy and more about protecting vulnerable lungs from unnecessary heavy exposure to fungal spores.
There is limited evidence that ordinary pet ownership worsens CPA. However, avoiding heavy exposure to mouldy hay, bedding, compost, bird droppings, and dusty animal housing is sensible.
Aspergillus bronchitis
In Aspergillus bronchitis, Aspergillus may be present in the airways and contribute to cough, sputum, and airway inflammation. Heavy exposure to fungal spores may aggravate symptoms in some people, although this relationship is less well understood than in ABPA.
People with significant immunosuppression
People with severely weakened immune systems may need stricter precautions. This can include people who have had organ or stem cell transplants, people receiving intensive chemotherapy, and people on high-dose immunosuppressive treatment.
For these patients, the concern may include invasive fungal infection. They should follow advice from their specialist team about pets, gardening, compost, bird cages, chicken coops, and mouldy environments.
| Condition | Main concern | Practical message |
|---|---|---|
| Allergic Bronchopulmonary Aspergillosis (ABPA) | Allergic reaction to Aspergillus spores | Reduce exposure to dusty, mouldy, or damp materials. |
| Severe Asthma with Fungal Sensitisation (SAFS) | Asthma worsening from fungal allergens | Avoid mouldy bedding, dusty hay, and damp animal housing. |
| Chronic Pulmonary Aspergillosis (CPA) | Protecting already damaged lungs | Avoid heavy or repeated spore exposure where possible. |
| Aspergillus bronchitis | Airway irritation and possible symptom aggravation | Keep exposure to dust and mould as low as practical. |
| Severe immunosuppression | Risk of serious fungal infection | Follow specialist medical advice; extra precautions may be needed. |
Practical advice for different pets
Dogs
Dogs are usually low risk from an Aspergillus exposure point of view. The main precautions are general hygiene and avoiding large amounts of mud, damp bedding, or mouldy outdoor kennels.
- Wash hands after handling pets, especially before eating.
- Keep dog bedding clean and dry.
- Avoid letting damp or mouldy bedding accumulate.
- If cleaning a dusty kennel or outdoor area, consider wearing an FFP2 or FFP3 mask.
Cats
Cats are also usually low risk. Litter trays can produce dust and odour, which may irritate the airways in some people.
- Use low-dust litter where possible.
- Change litter regularly.
- Avoid letting trays become damp or heavily soiled.
- Ask someone else to clean the tray if you are very sensitive to dust or smells.
- Wash hands after cleaning litter trays.
Guinea pigs, rabbits, hamsters, and other small mammals
For small mammals, the animal is usually not the main issue. The bigger concern is hay, bedding, and cage cleaning.
- Use clean, dry bedding.
- Replace bedding frequently.
- Remove damp bedding promptly.
- Store hay in a dry place.
- Do not use visibly mouldy hay, straw, or feed.
- Avoid shaking hay or bedding indoors.
- Clean cages in a well-ventilated area.
- If possible, ask another family member to do major cage cleaning.
- Consider wearing an FFP2 or FFP3 mask when cleaning dusty bedding.
Birds and chickens
Bird cages and chicken coops can create more dust exposure than many other pets. Droppings, bedding, feathers, seed husks, and feed dust can accumulate, especially in enclosed or poorly ventilated spaces.
- Clean cages and coops regularly.
- Avoid allowing droppings and bedding to build up.
- Improve ventilation where possible.
- Store feed dry.
- Avoid sweeping dry dust if damp cleaning is possible.
- Wear respiratory protection if cleaning a dusty coop or cage.
- People with severe lung disease or significant immunosuppression should discuss this with their clinical team.
Fish tanks and aquariums
Fish tanks are usually low risk for Aspergillus exposure. The main issue is preventing mould around lids, filters, walls, or damp cupboards.
- Clean tanks and filters regularly.
- Check for mould around the tank, lid, or nearby wall.
- Avoid damp build-up in enclosed cupboards.
Reptiles
Reptile enclosures are usually low risk if well maintained. Damp substrates, mouldy wood, or poorly cleaned vivariums may increase exposure to mould and other microbes.
- Replace damp or mouldy substrate promptly.
- Keep enclosures clean and well ventilated.
- Wash hands after handling reptiles or cleaning enclosures.
Children’s pets and shared responsibility
Many family pets are cared for by children or teenagers. This can be a positive way to teach responsibility and empathy. However, routine jobs can be forgotten during busy periods, holidays, exams, illness, or changes in family routine.
For someone in the household with aspergillosis, asthma, bronchiectasis, or another chronic lung condition, it is helpful for an adult or another family member to check regularly that pet care is being maintained.
Family pet-care check
- Is the bedding clean and dry?
- Has damp bedding been removed?
- Is the hay free from visible mould?
- Is feed stored somewhere dry?
- Is the cage, hutch, or coop well ventilated?
- Is there a regular cleaning routine?
- Does the person cleaning the cage need help or a mask?
The aim is not to discourage children from caring for pets. It is to avoid a situation where bedding, hay, or droppings are left long enough to become damp, dusty, mouldy, or heavily contaminated. Neglect increases avoidable exposure.
The benefits of pets
Any decision about pets should include benefits as well as risks. For many people with long-term lung disease, pets are not just animals in the house. They are companions, sources of comfort, and part of daily life.
Companionship
Chronic illness can be isolating. Pets can provide company, reassurance, and a sense of normality, especially for people who live alone or spend long periods at home.
Mental health and wellbeing
Pets may help reduce loneliness, stress, and anxiety. Many people find that caring for an animal gives emotional support during difficult periods of illness.
Routine and purpose
Feeding, grooming, walking, and caring for pets can provide structure to the day. This can be particularly valuable when illness, retirement, or reduced mobility has changed a person’s usual routine.
Gentle activity
Dogs may encourage regular walking and time outdoors. Even small amounts of gentle activity can support physical and mental wellbeing when paced appropriately.
Family connection
Pets can bring families together. Children caring for pets may learn responsibility, while shared pet care can create positive family routines.
Simple risk-reduction checklist
- Keep cages, hutches, beds, and coops clean.
- Replace bedding regularly.
- Remove damp bedding promptly.
- Store hay, straw, and feed in a dry place.
- Do not use visibly mouldy hay, bedding, or feed.
- Avoid shaking dusty bedding indoors.
- Clean animal housing in a well-ventilated area.
- Ask another household member to do dusty cleaning tasks if possible.
- Consider an FFP2 or FFP3 mask for dusty cage, hutch, or coop cleaning.
- Wash hands after handling animals or cleaning cages.
- Keep pet equipment away from food preparation areas.
- Discuss individual risks with your clinical team if you are severely immunosuppressed.
Common questions
Do I need to get rid of my pet if I have aspergillosis?
Usually, no. Most people with aspergillosis do not need to give up their pets. The focus is usually on reducing exposure to mouldy, dusty, or damp materials around pets.
Can my dog or cat give me aspergillosis?
This is not the usual way aspergillosis develops. Aspergillus exposure usually comes from breathing in mould spores from the environment, such as soil, compost, damp buildings, hay, bedding, or decaying organic material.
Are guinea pigs safe?
Guinea pigs themselves are usually not the main concern. The more likely source of fungal spores is hay or bedding, especially if it is damp, mouldy, dusty, or left unchanged for too long. Keep bedding clean and dry, replace it frequently, and store hay properly.
Are birds or chickens more risky?
Bird cages and chicken coops can create more dust and organic waste exposure than many other pet environments. Regular cleaning, good ventilation, dry feed storage, and respiratory protection during dusty cleaning can reduce exposure.
Should I wear a mask when cleaning pet cages?
If the task is dusty, involves hay or bedding, or takes place in a poorly ventilated area, wearing an FFP2 or FFP3 mask may be sensible, particularly for people with asthma, Allergic Bronchopulmonary Aspergillosis, Chronic Pulmonary Aspergillosis, bronchiectasis, or reduced lung reserve.
What is the biggest pet-related risk?
The biggest avoidable risks are usually mouldy hay, damp bedding, accumulated droppings, poorly stored feed, and dusty cleaning of animal housing.
Are pets good for people with aspergillosis?
For many people, yes. Pets can provide companionship, routine, comfort, and encouragement to stay active. These benefits can be very important for people living with long-term lung disease.
When to seek medical advice
Contact your GP, respiratory team, or specialist team if:
- Your breathing becomes suddenly worse.
- You develop new or worsening wheeze, chest tightness, or breathlessness.
- You cough up blood.
- You develop fever, chest pain, or feel acutely unwell.
- Your asthma becomes difficult to control.
- You notice a clear pattern of worsening symptoms after cleaning cages, hutches, coops, or handling hay.
- You are severely immunosuppressed and are concerned about mould exposure.
If you are very breathless, coughing up significant amounts of blood, have chest pain, or feel seriously unwell, seek urgent medical help.
Author and review information
Audience: Patients, carers, families, and non-specialists.
Purpose: General educational information about pet ownership and environmental exposure in people with aspergillosis or related lung conditions.
Important note: This article does not replace medical advice. Individual risk varies depending on diagnosis, lung function, immune status, medications, and home environment. If you are unsure, discuss your situation with your clinical team.
Last reviewed: June 2026
References and further reading
- Centers for Disease Control and Prevention. Reducing Risk for Aspergillosis.
- NHS. Aspergillosis.
- NHS 111 Wales. Aspergillosis.
- National Aspergillosis Centre, Manchester University NHS Foundation Trust. About Aspergillosis.
- Centers for Disease Control and Prevention. Small Mammals: Healthy Pets, Healthy People.
- Asthma + Lung UK. Air pollution and allergies at home.
- Asthma and Allergy Foundation of America. Mold Allergy.
- Allergy UK. Asthma and Respiratory Allergy.
- Aspergillosis Patient Support

Healthy Eating Should Not Feel Like Punishment

Many people living with aspergillosis ask what they should eat. Unfortunately, the answer can seem confusing. One expert says eat less fat. Another says eat less sugar. Then come messages about protein, probiotics, supplements, fasting, gut health and the latest “superfood”.
This article takes a different approach. Rather than focusing on strict dietary rules, it explores what we know, what we still do not know, and how to build a way of eating that is realistic, enjoyable and sustainable while living with a long-term condition.
Healthy eating should not feel like punishment. It should feel like finding more foods you enjoy and fewer foods you later regret.
Important: follow personalised medical advice
If your doctor, specialist nurse or dietitian has recommended a specific diet for you, continue to follow that advice unless they recommend otherwise.
This article provides general information and does not replace personalised medical or dietary advice.
Some people with aspergillosis may need specialised dietary support because of weight loss, malnutrition, diabetes, kidney disease, liver disease, food allergies, coeliac disease, digestive disorders or medication-related side effects.
For some people, maintaining weight, strength and muscle mass may be more important than weight loss. Your healthcare team may recommend a different approach based on your individual circumstances.
Key points
- Healthy eating does not need to be perfect.
- Most dietary advice is less complicated than headlines suggest.
- Food should be enjoyable as well as nutritious.
- Plant foods remain one of the strongest foundations of a healthy diet.
- Many expensive health products offer little advantage over ordinary foods.
- Some people with aspergillosis experience gut symptoms related to illness, medication or other health conditions.
- Diet can support wellbeing but does not replace medical treatment.
Contents
- Why are we so confused about food?
- Healthy eating is not about perfection
- What does the evidence actually show?
- Food is more than nutrients
- The microbiome and fermented foods
- Healthy eating in a modern world
- Healthy eating in the real world
- Diet, gut symptoms and aspergillosis
- Practical ideas
- Common questions
- Resources and further reading
Why are we so confused about food?
Many patients tell us they no longer know what to believe about food. This is hardly surprising.
Over the years we have been told to avoid fat, then sugar, then carbohydrates. We have been encouraged to buy supplements, protein products, probiotics, wellness products and specialist diets. Meanwhile, researchers continue to discover new complexities in nutrition and human biology.
The problem is not that scientists know nothing. The problem is that health messages are often simplified into headlines while commercial interests compete for attention.
When someone is living with a chronic illness, those mixed messages can become exhausting.
The reassuring news is that the broad foundations of healthy eating have changed much less than many people realise.
Healthy eating is not about perfection
One of the biggest misconceptions about healthy eating is that every meal must be perfect.
Real life does not work that way. People have birthdays, holidays, stressful weeks, family gatherings, fatigue, illness and financial pressures.
A healthy diet is not built from one meal. It is built from hundreds and thousands of meals over months and years.
One takeaway meal does not undo a healthy lifestyle. One difficult week does not erase years of sensible habits.
The aim is consistency, not perfection.
Many people find that once they stop chasing perfection, healthy eating becomes much easier to maintain.
What does the evidence actually show?
Despite changing headlines, most major health organisations continue to recommend broadly similar eating patterns.
The strongest evidence supports diets that contain plenty of:
- vegetables
- fruit
- beans and lentils
- whole grains
- nuts and seeds
- adequate protein
- moderate amounts of minimally processed foods
This does not mean everyone must become vegetarian or vegan. It means that plant foods should form a larger part of everyday eating.
A useful summary is:
Eat mostly real foods, especially plant foods, and make the pattern sustainable.
Food is more than nutrients
One reason nutrition advice can be confusing is that food is far more complex than scientists once believed.
For many years, nutrition focused on individual nutrients such as fat, sugar, protein or vitamins. Today, we increasingly understand that foods work as complete packages.
An apple is not simply sugar. It also contains fibre, water, vitamins, minerals and plant compounds, all packaged in a structure that affects how it is digested.
Food also provides pleasure, culture, social connection and enjoyment. That is one reason why healthy eating should not feel like punishment.
The microbiome and fermented foods
One of the most exciting areas of modern research is the gut microbiome — the community of bacteria, fungi and other microorganisms that live in our digestive system.
Researchers now know that the microbiome influences digestion, immunity, inflammation and metabolism. There is also growing evidence that it may affect mood and sleep, although this research is still developing.
This has led to increasing interest in foods such as:
- kefir
- live yoghurt
- sauerkraut
- kimchi
- miso
- tempeh
The evidence is promising but still emerging. Fermented foods are not a miracle cure.
A useful way to think about them is that they may be another brick in building your wellbeing home, alongside exercise, sleep, social connection and good medical care.
If you enjoy fermented foods and tolerate them well, they may be a useful part of a varied diet. If they worsen symptoms such as bloating, reflux or diarrhoea, they may not suit you.
Healthy eating in a modern world
If healthy eating were simply a matter of knowing what was good for us, most of us would find it much easier.
The reality is that modern food environments are full of mixed messages. Many people genuinely want to improve their health but end up spending money, energy and effort on approaches that may not make much difference.
When good advice becomes marketing
Many health messages begin with good intentions.
Take protein as an example. As we get older, maintaining muscle mass becomes increasingly important. This is one reason why many people over the age of 60 are encouraged to pay more attention to protein intake.
That is sensible advice.
The difficulty comes when a useful health message becomes a marketing opportunity. Suddenly supermarket shelves fill with protein bars, protein cereals, protein biscuits, protein drinks, protein puddings and protein snacks.
Some may be useful in specific situations. Many are expensive. Some contain surprisingly large amounts of sugar, sweeteners, saturated fat or highly processed ingredients.
The important question is often not:
How can I buy more protein products?
but:
How can I include protein-containing foods more regularly?
For many people, foods such as eggs, yoghurt, milk, beans, lentils, fish, nuts, seeds, tofu and lean meat can answer that question perfectly well.
The same pattern appears repeatedly throughout nutrition. Foods become fashionable. Products are marketed aggressively. The simple message is often lost.
The foods we forget about
One consequence of modern food marketing is that ordinary foods can start to look uninteresting.
We hear about superfoods, supplements and specialist health products. Meanwhile, some of the most nutritious foods available are sitting quietly on supermarket shelves:
- oats
- beans
- lentils
- peas
- carrots
- cabbage
- apples
- potatoes
- eggs
- wholemeal bread
These foods rarely appear in glossy advertisements. Nobody is becoming rich by persuading people to eat more cabbage.
Yet foods like these have nourished populations for generations.
Health is rarely created by a single miracle food. It is usually created by patterns that are repeated day after day and year after year.
The sugar-to-salt problem
Many people trying to eat more healthily reduce sugar and then find themselves adding more salt.
This is understandable. Food still needs to be enjoyable, and salt is one of the easiest ways to make food taste more rewarding.
However, healthy eating should not simply mean replacing one flavour driver with another.
A useful alternative is to build flavour using herbs, spices, garlic, onions, tomatoes, mushrooms, vinegar, lemon juice, chilli, ginger, mustard, pepper and other naturally flavourful ingredients.
The goal is not bland food. The goal is delicious food that does not depend entirely on sugar, salt or highly processed flavourings.
The health halo problem
Food packaging often highlights one positive feature: high protein, low fat, natural, gut friendly, organic, gluten free or source of vitamins.
The claim may be true, but it only tells part of the story.
A high-protein biscuit is still a biscuit. A low-fat dessert may still contain a large amount of sugar. A vitamin-fortified snack may still be highly processed.
It is often more useful to look at the overall food rather than a single headline claim.
Healthy eating in the real world
Perhaps the biggest problem with many nutrition articles is that they assume everyone has the same life.
They assume everyone enjoys cooking. They assume everyone has plenty of energy. They assume everyone has disposable income.
For many people living with aspergillosis, none of those assumptions are true.
Fatigue, breathlessness, disability, caring responsibilities and financial pressures can all affect what ends up on the plate.
That is why healthy eating should be realistic. Healthy eating should fit around your life, not the other way around.
You do not have to cook everything from scratch
There is a common belief that healthy eating means preparing every meal from fresh ingredients.
In reality, many convenient foods can be part of a healthy diet.
Frozen vegetables are still vegetables. Frozen fruit is still fruit. Tinned beans are still beans. Microwave rice is still rice. Wholemeal bread is still bread. Plain yoghurt is still yoghurt. Tinned fish is still fish.
These foods can save time, reduce waste and often cost less than fresh alternatives.
Healthy eating does not have to be expensive
Many heavily marketed health foods are expensive. Protein bars, specialist snacks, supplements and wellness products often cost far more than ordinary foods.
Some of the most nutritious foods available are also among the cheapest. Oats, beans, lentils, potatoes, carrots, cabbage, frozen vegetables, eggs and wholemeal bread can provide good nutrition at a modest cost.
Healthy eating is not about buying expensive products. It is about building meals from foods that provide good nutrition at a price you can afford.
If energy is limited, simplify
Many people with aspergillosis experience fatigue. On difficult days, preparing a complicated meal may simply not be realistic.
That is perfectly okay. Simple meals are still meals.
- beans on wholemeal toast
- soup and bread
- yoghurt and fruit
- a baked potato with beans
- an omelette with vegetables
- tinned fish with salad
- microwave rice with beans and vegetables
- porridge with fruit
Healthy eating does not need to be complicated to be effective.
A simple meal that you can manage is usually better than an ideal meal that never gets made.
The goal is not dietary perfection. The goal is to build a way of eating that works in the life you actually have.
If you are losing weight, the advice may be different
Not everyone needs to lose weight.
Some people with chronic pulmonary aspergillosis (CPA), severe lung disease or other long-term illnesses struggle to maintain their weight and muscle mass.
For these individuals, increasing calories and protein may be more important than restricting foods.
If you are losing weight unintentionally, have a poor appetite, or are becoming weaker, discuss this with your healthcare team. A dietitian may be able to help.
Diet, gut symptoms and aspergillosis
Many people living with aspergillosis report digestive symptoms at some stage.
These may include:
- bloating
- reflux or indigestion
- nausea
- abdominal discomfort
- altered bowel habits
- diarrhoea or constipation
- reduced appetite
There can be many possible causes. In some people, symptoms may be related to medicines used to manage aspergillosis or associated conditions. Antifungal drugs, antibiotics, steroids and other medicines can sometimes affect the digestive system. Reduced activity, stress, infection, inflammation and changes in eating patterns may also contribute.
There is currently no proven “aspergillosis diet” that treats aspergillosis itself.
Good nutrition can support general health, energy, muscle strength and recovery, but it should be viewed as complementary to medical treatment, not an alternative.
Do not alter prescribed treatment without medical advice
Do not stop or change antifungal medicines, steroids, biologics, inhalers, antibiotics or other prescribed treatments because of diet advice without discussing this with your healthcare team.
If you think a medicine is causing digestive symptoms, report this to your doctor, specialist nurse or pharmacist. They may be able to adjust timing, check for interactions, investigate symptoms or consider alternatives where appropriate.
Practical ideas
Healthy eating does not have to mean changing everything at once. Small changes are often more sustainable.
- Add one extra portion of vegetables to a meal.
- Choose wholegrain bread, oats, brown rice or wholewheat pasta more often.
- Add beans, lentils or chickpeas to soups, stews, curries or pasta sauces.
- Keep fruit visible and easy to reach.
- Use frozen vegetables when energy is low.
- Try live yoghurt or kefir if you enjoy fermented foods and tolerate them well.
- Replace some packaged snacks with fruit, nuts, yoghurt or wholegrain options.
- Cook extra portions when you have energy and freeze them for lower-energy days.
For people who are underweight or losing weight, these ideas may need adapting to include more calories and protein. A dietitian can help with this.
Common questions
Can diet treat aspergillosis?
No specific diet has been proven to treat aspergillosis. Antifungal medicines, steroids, biologics, inhalers, monitoring and specialist care may all be important depending on the type of aspergillosis. Diet can support general health but should not replace medical treatment.
Should I cut out sugar completely?
Most people do not need to cut out sugar completely. It is more useful to reduce frequent sugary drinks, sweets, cakes and biscuits, while enjoying naturally sweet foods such as fruit.
Should I cut out fat?
No. The body needs some fat. The source matters. Nuts, seeds, olive oil, oily fish and avocados contain healthier fats. It is sensible to limit large amounts of saturated fat from highly processed foods, fatty meats, butter, cream and pastries.
Should I eat more protein as I get older?
Many older adults need to pay attention to protein because it helps support muscle mass and strength, especially alongside physical activity. This does not necessarily mean buying protein bars or protein drinks. Ordinary foods such as beans, lentils, eggs, fish, yoghurt, milk, cheese, tofu, nuts, seeds and lean meat can all contribute protein.
Are fermented foods safe for people with aspergillosis?
Many fermented foods are safe for most people and may support gut health. Choose foods that are properly prepared and stored. Avoid homemade ferments that show visible mould or smell abnormal. If you are severely immunocompromised, ask your clinical team for individual advice before using probiotic supplements or unusual fermented products.
Do I need supplements?
Not necessarily. Supplements are useful when there is a clear reason, such as deficiency or specific medical advice. They are not a substitute for a varied diet. Check with a clinician or pharmacist before starting high-dose supplements or herbal products.
What if healthy eating feels too difficult?
Start small. Add one useful food rather than trying to change everything. For example, add fruit to breakfast, vegetables to dinner, or beans to soup. Small changes repeated often can matter more than short bursts of perfection.
When should I seek medical advice?
Ask your GP, specialist nurse, pharmacist or dietitian for advice if you are losing weight without trying, have persistent diarrhoea, vomiting, reflux or abdominal pain, have blood in your stool, are struggling to maintain weight or muscle strength, or think your medication may be causing gut symptoms.
Final thought
Food should not become another source of guilt for people already managing a long-term condition.
A good diet is not about perfection, punishment or expensive products. It is about building a pattern of eating that helps you feel as well as possible, supports your body over time, and still allows you to enjoy your meals.
Most people do not need a perfect diet. They need a way of eating that is good enough, enjoyable enough and sustainable enough to become part of normal life.
Resources and further reading
- NHS: The Eatwell Guide
- NHS: Eating a balanced diet
- NHS: Vitamin D
- British Dietetic Association: Healthy eating
- British Dietetic Association: Vitamin D
- British Dietetic Association: Protein
- World Health Organization: Healthy diet
- BMJ: Ultra-processed food exposure and adverse health outcomes
- Aspergillosis.org: Patient information and support
Author: Aspergillosis.org patient information team
Reviewed by: To be reviewed by clinical team before publication
Last reviewed: June 2026
Disclaimer: This article is for general information only and does not replace advice from your own healthcare team.
```
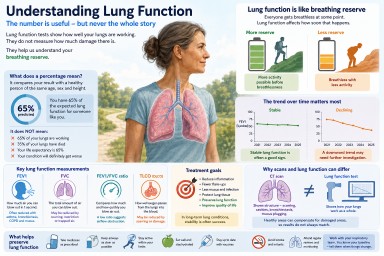
Understanding Lung Function in Aspergillosis and Asthma
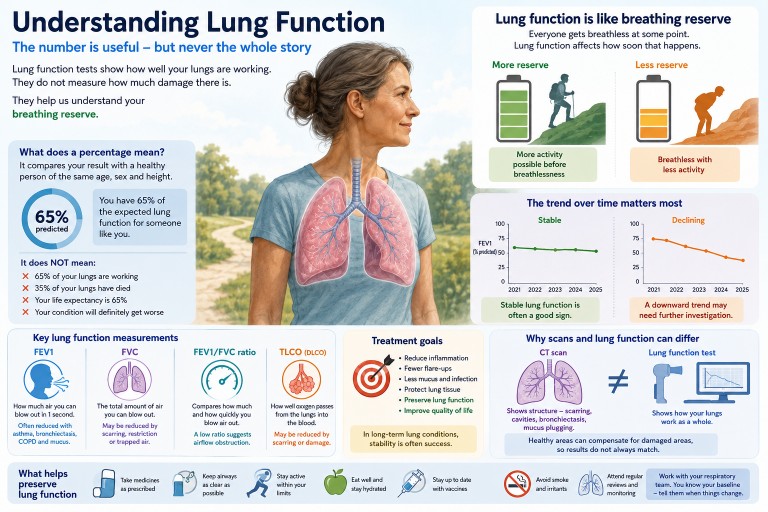
Key points
- Lung function tests show how well your lungs are working, not simply how damaged they look.
- “60% lung function” usually means 60% of the predicted value for someone of your age, sex and height.
- It does not mean 40% of your lungs have stopped working.
- Everyone loses some lung function naturally with age.
- For many people with aspergillosis or asthma, the trend over time matters more than one single result.
- Successful treatment often means stabilising lung function and preventing further decline.
Contents
- What are lung function tests?
- What does a percentage result mean?
- Lung function as breathing reserve
- Do we naturally lose lung function with age?
- Important lung function results
- What patterns are seen in aspergillosis?
- Why scans and lung function do not always match
- Can treatment stop lung function getting worse?
- When to seek medical help
- Common questions
What are lung function tests?
Lung function tests, also called breathing tests or pulmonary function tests, measure how well your lungs are working.
They can help doctors understand:
- how much air you can breathe out,
- how quickly you can empty your lungs,
- whether your airways are narrowed,
- whether your lungs are restricted or stiff,
- how well oxygen passes from the lungs into the blood.
These tests do not diagnose aspergillosis by themselves. Instead, they are one part of the overall picture, alongside symptoms, CT scans, blood tests, sputum tests, oxygen levels and how active you are day to day.
What does a percentage result mean?
Patients are often told things like:
“Your lung function is 65%.”
This can sound frightening, but it is often misunderstood.
A percentage result usually means your result compared with the value expected for a healthy person of the same:
- age,
- sex,
- height,
- and sometimes ethnic background, depending on the reference system used.
So, if your FEV1 is 65% predicted, it means your measured FEV1 is 65% of the value expected for someone like you.
It does not mean:
- 65% of your lungs are working,
- 35% of your lungs have died,
- you have lost 35% of your life expectancy,
- or that your condition will definitely keep getting worse.
Lung function as breathing reserve
A helpful way to think about lung function is as breathing reserve.
Everyone becomes breathless if they work hard enough. Lung function affects how soon that breathlessness appears.
| Activity | Someone with good breathing reserve | Someone with reduced breathing reserve |
|---|---|---|
| Sitting quietly | Comfortable | Usually comfortable |
| Walking around the house | Comfortable | Usually manageable |
| Shopping | Comfortable or mildly breathless | May need to slow down or pause |
| Climbing stairs | Mildly breathless | More likely to become breathless |
| Walking uphill | Breathless with effort | Breathless sooner and may need rests |
This is why two people with the same lung function percentage can feel very different. Breathlessness is also affected by fitness, weight, muscle strength, heart health, asthma control, mucus, anxiety, anaemia and recent infections.
Do we naturally lose lung function with age?
Yes. Lung function normally peaks in early adulthood and then gradually declines over time.
This happens because of natural changes in:
- lung elasticity,
- the chest wall,
- respiratory muscles,
- and small airways.
However, predicted lung function values already take age into account. This means a 70-year-old is not being compared with a healthy 25-year-old. They are being compared with expected values for someone of similar age, sex and height.
This is why the trend over time is often more useful than a single number.
| Year | FEV1 | Possible interpretation |
|---|---|---|
| 2022 | 64% | Relatively stable |
| 2023 | 63% | |
| 2024 | 65% | |
| 2025 | 62% |
A person may worry about being “only 62%”, while their respiratory team may be reassured that the result has remained stable for several years.
Important lung function results
FEV1
FEV1 stands for Forced Expiratory Volume in One Second.
It measures how much air you can blow out forcefully in the first second after taking a deep breath.
This is often the number people mean when they say, “My lung function is 60%.”
FEV1 is often reduced when airways are narrowed, as in asthma, chronic obstructive pulmonary disease (COPD), bronchiectasis or mucus plugging.
FVC
FVC stands for Forced Vital Capacity.
It measures the total amount of air you can blow out after taking the deepest breath possible.
FVC may be reduced if the lungs cannot expand fully, if there is scarring, restriction, muscle weakness, poor test technique, or if air becomes trapped in the lungs.
FEV1/FVC ratio
The FEV1/FVC ratio compares how much air you blow out in the first second with the total amount you can blow out.
A low ratio usually suggests airflow obstruction. This is common in asthma, COPD and some people with bronchiectasis.
TLCO or DLCO
TLCO or DLCO is often called gas transfer.
It measures how well oxygen passes from the air sacs in the lungs into the bloodstream.
Gas transfer may be reduced by scarring, emphysema, blood vessel problems in the lungs, anaemia, or other lung damage. Sometimes spirometry looks fairly good but gas transfer is reduced, which can help explain breathlessness.
What patterns are seen in aspergillosis?
There is no single “typical” lung function result for aspergillosis patients.
Aspergillosis often develops in people who already have asthma, bronchiectasis, previous tuberculosis, chronic obstructive pulmonary disease, sarcoidosis, prior lung surgery or other lung conditions. This means lung function varies widely from person to person.
Allergic bronchopulmonary aspergillosis (ABPA)
Allergic bronchopulmonary aspergillosis is an allergic inflammatory reaction to Aspergillus, usually in people with asthma or cystic fibrosis.
Lung function may show:
- airflow obstruction,
- reduced FEV1,
- fluctuation during flares,
- improvement after treatment,
- or gradual decline if inflammation and mucus plugging repeatedly damage the airways.
Chronic pulmonary aspergillosis (CPA)
Chronic pulmonary aspergillosis usually occurs in lungs that have already been damaged by another condition.
Lung function may show:
- reduced breathing reserve,
- reduced FVC if there is scarring or volume loss,
- reduced gas transfer,
- or surprisingly preserved spirometry despite abnormal CT scans.
In CPA, stability can be a very positive treatment outcome.
Aspergillus bronchitis
Some people have chronic Aspergillus infection or colonisation in the airways with cough and sputum production.
Symptoms may be troublesome even when lung function changes are modest. This is one reason doctors do not rely on lung function tests alone.
Asthma with Aspergillus sensitisation
Some people with asthma are sensitised to Aspergillus without meeting criteria for ABPA.
Their lung function may vary depending on asthma control, airway inflammation, triggers, inhaler use and recent infections.
Why scans and lung function do not always match
Patients are sometimes told:
“Your CT scan shows quite a lot of damage, but your lung function is better than expected.”
This can happen because CT scans and lung function tests measure different things.
A CT scan shows what the lungs look like. It can show bronchiectasis, scarring, cavities, mucus plugging, nodules or areas of collapse.
Lung function tests show how the lungs work overall.
The lungs have a large reserve capacity. If some areas are damaged but other areas remain healthy, the healthy areas can often compensate. This is why a scan can look alarming while lung function remains better than expected.
The opposite can also happen. A scan may look only mildly abnormal, but the person may feel very breathless because of asthma, small airways disease, poor gas transfer, deconditioning, anaemia, heart disease, anxiety or muscle weakness.
Can treatment stop lung function getting worse?
For many aspergillosis and asthma patients, one of the main aims of treatment is to preserve lung function.
Successful treatment does not always mean lung function returns to normal. It may mean:
- fewer flare-ups,
- less inflammation,
- less mucus plugging,
- fewer infections,
- better symptoms,
- stable CT scans,
- and little or no further decline in lung function.
In allergic bronchopulmonary aspergillosis, treatment aims to reduce inflammation and prevent repeated episodes that can damage the airways.
In chronic pulmonary aspergillosis, antifungal treatment often aims to slow or stop progression, reduce symptoms and preserve remaining lung function.
In asthma, good control with inhalers, biologics where appropriate, trigger reduction and treatment of associated conditions can reduce exacerbations and protect lung health.
For many patients, hearing that lung function is “stable” may sound disappointing. In long-term lung disease, stability is often a very good result.
Small changes are not always meaningful
Lung function tests require effort and technique. Results can vary from day to day.
A small change may reflect:
- how well the test was performed,
- tiredness,
- recent infection,
- asthma control,
- mucus,
- time of day,
- or normal measurement variability.
This is why clinicians look for sustained patterns rather than reacting to every small rise or fall.
Questions to ask your respiratory team
- Which result are we talking about: FEV1, FVC, ratio or gas transfer?
- Is my result stable compared with previous tests?
- Is the pattern obstructive, restrictive, mixed or mainly gas transfer-related?
- Does this result explain my symptoms?
- Could asthma, mucus plugging or infection be affecting today’s result?
- What result would make you concerned about deterioration?
- What can I do to help preserve my lung function?
When to seek medical help
Seek medical advice if you notice:
- a clear and persistent worsening of breathlessness,
- breathlessness at rest or with minimal activity,
- new or worsening wheeze,
- coughing up blood,
- fever or signs of infection,
- new chest pain,
- oxygen levels lower than usual if you monitor them,
- or a sudden drop in exercise tolerance.
Seek urgent medical help if breathlessness is severe, sudden, associated with chest pain, blue lips, confusion, fainting, or oxygen levels are dangerously low compared with your usual readings.
Common questions
What does “60% lung function” mean?
It usually means one of your lung function results is 60% of the value predicted for someone of your age, sex and height. It does not mean only 60% of your lungs are working.
Is there a normal amount of lung function for aspergillosis patients?
No. Aspergillosis patients vary widely. Some have normal or near-normal lung function. Others have severe impairment, often because aspergillosis has developed on top of another lung condition.
Does lower lung function mean I will be more breathless?
Often, yes. Lower lung function usually means less breathing reserve, so you may become breathless with less effort. However, symptoms also depend on fitness, weight, muscle strength, asthma control, mucus, oxygen levels and other health conditions.
Can my lung function improve?
Sometimes. Lung function may improve if asthma control improves, inflammation settles, mucus plugging clears, infection is treated, or fitness improves. Permanent scarring and bronchiectasis are less likely to reverse.
Is stable lung function a good result?
Yes. In long-term lung disease, stable lung function over months or years can be a very positive sign that treatment and monitoring are helping to prevent further deterioration.
Why do I feel worse if my lung function has not changed?
Breathlessness and fatigue can worsen for many reasons, including infection, mucus, asthma flare, anaemia, heart problems, medication side effects, poor sleep, anxiety, pain or loss of fitness. Lung function is important, but it is not the only explanation for symptoms.
Summary
Lung function results are useful, but they need careful interpretation.
The number is not a simple measure of how much lung you have left. It is better understood as a measure of breathing reserve compared with what would be expected for someone like you.
For people with aspergillosis and asthma, the most important question is often not “What is my lung function today?” but “Is my lung function stable over time?”
Many patients live active and fulfilling lives with lung function results that sound worrying when expressed as a percentage. The result matters, but so do symptoms, CT scans, oxygen levels, exercise ability, treatment response and the overall trend.
In long-term lung disease, stability is not failure. Stability can be success.
References and further reading
Author and review information
Written for: aspergillosis.org
Intended audience: People living with aspergillosis, asthma, bronchiectasis or other long-term lung conditions, and their families.
Clinical note: This article is for general education and should not replace advice from your own respiratory team.
Last reviewed: June 2026