
Professional Aspergillosis Update: May 2026
Audience: respiratory physicians, infectious diseases physicians, clinical microbiologists, haematologists, pharmacists, specialist nurses, laboratory scientists and researchers with an interest in aspergillosis.
Contents
Key messages
- Isavuconazole therapeutic drug monitoring may have a selective role. Although isavuconazole is usually more predictable than voriconazole, real-world pharmacokinetic variability remains clinically relevant in some patients.
- Posaconazole prophylaxis should not automatically be avoided with midostaurin. The interaction is real, but clinical consequences may often be manageable with careful monitoring.
- Surrogate azole susceptibility testing has limits. Voriconazole gradient diffusion testing may help screen for broader azole resistance, but it should not replace direct susceptibility testing where treatment decisions depend on the result.
- Invasive fungal sinusitis remains a high-mortality emergency in haematological malignancy. Early tissue diagnosis, ENT involvement and multidisciplinary management remain central.
- Non-fumigatus Aspergillus species are becoming more important research targets. New CRISPR-Cas9 tools for Aspergillus calidoustus may support future work on virulence and antifungal resistance.
Top papers this month
1. Isavuconazole pharmacokinetics and pharmacodynamics in real-world practice
Guidi M, Couchepin J, Reinhold I, Kronig I, Neofytos D, Schreiber PW, André P, Buclin T, Lamoth F.
Characterization of isavuconazole pharmacokinetics and pharmacodynamics in a real-life cohort.
JAC Antimicrobial Resistance. 2026;8(3):dlag071.
PMID: 42088097
Why this paper was selected
Isavuconazole is increasingly used for invasive aspergillosis because of its favourable safety profile and generally more predictable pharmacokinetics compared with voriconazole. This study provides important real-world evidence that clinically relevant interpatient variability still occurs and that therapeutic drug monitoring may have a role in selected patients.
Key findings
- Isavuconazole showed relatively predictable pharmacokinetics overall.
- Clinically relevant variability in drug exposure was still observed between patients.
- Therapeutic drug monitoring identified patients with atypically low or high exposure.
- Exposure relative to fungal minimum inhibitory concentration may be more informative than plasma concentration alone.
- No strong concentration-dependent toxicity signal was observed within the exposure range studied.
Clinical significance
This paper challenges the assumption that isavuconazole therapeutic drug monitoring is rarely useful. While the findings do not justify universal routine monitoring, they support selective monitoring in complex patients, particularly where there is treatment failure, suspected malabsorption, significant drug interactions, unusual body composition, long-term therapy, or infection with isolates showing elevated minimum inhibitory concentrations.
Implications for practice
Classification: Important but not yet practice changing.
The study supports a more individualised approach to isavuconazole use. It also reinforces the direction of travel in antifungal stewardship: interpreting drug exposure alongside fungal susceptibility rather than considering plasma concentrations in isolation.
Evidence assessment
Evidence quality: Moderate. The real-world dataset and pharmacokinetic-pharmacodynamic modelling strengthen the evidence base, but the observational design limits causal inference and definitive exposure targets were not established.
Editorial assessment
This is one of the most clinically relevant antifungal pharmacology papers in this update. It does not establish mandatory isavuconazole monitoring, but it provides a strong argument for selective therapeutic drug monitoring in high-risk or complex aspergillosis patients.
2. Managing posaconazole and midostaurin interactions in FLT3-mutated AML
Joisten CS, Mellinghoff SC, Seidel D, Müller C, Müller-Ohrem C, Kreuzer K-A, Frenzel LP, Simon F, Hallek M, Koehler P, Cornely OA, Stemler J.
Clinical impact of potential drug-drug interactions between midostaurin and posaconazole in FLT3-mutated AML.
Antimicrobial Agents and Chemotherapy. 2026;70(6):e01951-25.
PMID: 42118097
Why this paper was selected
Posaconazole prophylaxis is central to prevention of invasive aspergillosis in patients undergoing intensive acute myeloid leukaemia treatment. Midostaurin is metabolised through CYP3A4, and posaconazole is a potent CYP3A4 inhibitor. This study addresses a common real-world dilemma: whether this interaction should alter antifungal prophylaxis practice.
Key findings
- The pharmacokinetic interaction between posaconazole and midostaurin was confirmed.
- Clinical toxicity appeared less severe than theoretical concerns might suggest.
- Many patients were able to receive both agents without major treatment-limiting toxicity.
- Individual variability in exposure and tolerability remained important.
- The findings support continued attention to monitoring rather than automatic avoidance of posaconazole.
Clinical significance
This paper is important because it addresses an immediate bedside decision. Avoiding posaconazole because of interaction concerns may leave high-risk acute myeloid leukaemia patients vulnerable to invasive aspergillosis. The study suggests that the interaction is clinically manageable in many patients when appropriate monitoring and multidisciplinary oversight are in place.
Implications for practice
Classification: Important but not yet practice changing.
The paper supports continued use of posaconazole prophylaxis where clinically indicated, with careful monitoring for toxicity and close collaboration between haematology, infectious diseases, microbiology and pharmacy teams.
Evidence assessment
Evidence quality: Moderate. The study is clinically relevant and real-world, but observational. It does not establish definitive dose-adjustment protocols or replace existing guideline recommendations.
Editorial assessment
The key message is that proven antifungal prophylaxis should not be abandoned solely because of theoretical interaction concerns. The interaction is real, but careful monitoring is generally preferable to withholding protection against invasive aspergillosis in a very high-risk group.
3. Can voriconazole susceptibility predict isavuconazole or posaconazole susceptibility?
Vahedi-Shahandashti R, Nickel A-S, Eisele D, Lass-Flörl C; ISHAM Working Group Member of Intrinsic Antifungal Resistance.
Can voriconazole gradient diffusion testing results be extrapolated to isavuconazole and posaconazole in Aspergillus spp.? Comparative analysis with CLSI broth microdilution and cyp51A gene sequencing.
Antimicrobial Agents and Chemotherapy. 2026;70(6):e01813-25.
PMID: 42138696
Why this paper was selected
Azole resistance in Aspergillus species is a growing problem, but not all laboratories can perform comprehensive susceptibility testing for every triazole. This paper asks whether voriconazole gradient diffusion testing can be used as a practical surrogate marker for broader azole susceptibility.
Key findings
- Voriconazole susceptibility often correlated with broader azole susceptibility patterns.
- Elevated voriconazole minimum inhibitory concentrations frequently corresponded with reduced isavuconazole susceptibility.
- Prediction of posaconazole susceptibility was less reliable.
- Discordant susceptibility profiles occurred, particularly among resistant isolates.
- cyp51A sequencing helped explain many resistance patterns but did not account for all phenotypes.
Clinical significance
The study supports voriconazole gradient diffusion testing as a useful first-line screening approach, especially where full reference testing is not immediately available. However, it also highlights a critical limitation: susceptibility to one triazole cannot be assumed to guarantee susceptibility to another.
Implications for practice
Classification: Important but not yet practice changing.
Voriconazole gradient diffusion testing may help identify isolates that require further investigation, but it should not replace direct isavuconazole or posaconazole susceptibility testing where treatment decisions depend on accurate results.
Evidence assessment
Evidence quality: Moderate to high for a laboratory diagnostic study. The use of CLSI broth microdilution and cyp51A sequencing strengthens the analysis, but clinical outcome data were not assessed.
Editorial assessment
This is a practical paper for clinical mycology laboratories. The main message is that surrogate azole testing can support screening and stewardship, but definitive treatment decisions should still be based on agent-specific susceptibility testing and molecular resistance analysis where available.
4. Invasive fungal sinusitis in haematological malignancy
Athni TS, Strauch CB, Kovac V, Arbona-Haddad E, Villa IP, Gupta S, Aleissa MM, Liakos AD, Tong A, Vedula RS, Maxfield AZ, Bergmark RW, Sherman AC.
Invasive fungal sinusitis in patients with hematological malignancies: a 20-year study from a tertiary academic US hospital system.
Open Forum Infectious Diseases. 2026;13(6):ofag304.
PMID: 42238379
Why this paper was selected
Invasive fungal sinusitis is a severe but less commonly discussed manifestation of invasive mould disease. In haematological malignancy, delayed recognition can lead to orbital, intracranial and fatal complications. This 20-year cohort provides useful long-term clinical insight.
Key findings
- Aspergillus species and Mucorales were the dominant pathogens.
- Mortality remained substantial despite modern antifungal therapy and supportive care.
- Early imaging, endoscopic assessment, tissue biopsy and histopathology remained central to diagnosis.
- Successful management frequently required combined medical and surgical approaches.
- Multidisciplinary care involving haematology, infectious diseases, ENT, microbiology and radiology was essential.
Clinical significance
This study reinforces that invasive aspergillosis is not solely a pulmonary disease. Sinonasal invasive fungal disease remains an emergency in profoundly immunocompromised patients. Distinguishing aspergillosis from mucormycosis is particularly important because antifungal treatment choices differ substantially.
Implications for practice
Classification: Important but not practice changing.
The paper reinforces existing best practice: early suspicion, urgent ENT involvement, tissue diagnosis, prompt antifungal therapy and multidisciplinary management.
Evidence assessment
Evidence quality: Moderate. The long observation period and detailed clinical experience are strengths, but the retrospective single-system design limits causal conclusions.
Editorial assessment
This paper is a useful reminder that early recognition remains one of the strongest determinants of outcome in invasive fungal disease. Persistent or atypical sinus symptoms in high-risk haematology patients should prompt urgent assessment rather than routine treatment as uncomplicated bacterial sinusitis.
Important development
5. Invasive mould infections in transplant recipients
Sudhaharan S, Pamidimukkala U, Bojja S, Raju DSB, Kk R, Gopal PSS.
Invasive mold infections among transplant recipients: a single-center observational study.
Journal de Mycologie Médicale / Journal of Medical Mycology. 2026;36(2):101629.
DOI: 10.1016/j.mycmed.2026.101629
Why this paper was selected
Transplant recipients remain a key high-risk population for invasive aspergillosis and other invasive mould infections. This observational study provides contemporary real-world data on presentation, diagnosis, microbiology, treatment and outcomes in a transplant centre.
Key findings
- Aspergillus species remained the predominant mould pathogen.
- Pulmonary disease was the most common presentation.
- Diagnosis required multimodal assessment combining clinical, radiological and mycological data.
- Invasive mould infections remained associated with substantial morbidity and mortality.
- Earlier diagnosis was associated with more favourable outcomes.
Clinical significance
The study confirms rather than changes current understanding. Its main value is as a contemporary reminder that invasive aspergillosis remains a major threat in transplantation despite advances in prophylaxis, diagnostics and antifungal treatment.
Implications for practice
Classification: Important but not practice changing.
The findings support ongoing vigilance, rapid investigation pathways, early multidisciplinary input and antifungal stewardship in transplant programmes.
Evidence assessment
Evidence quality: Moderate. Real-world applicability is useful, but the single-centre observational design and modest sample size limit generalisability.
Editorial assessment
This paper does not introduce a new management strategy, but it reinforces an enduring message: invasive aspergillosis outcomes in transplant recipients remain strongly dependent on early recognition and timely treatment.
Research horizon
6. CRISPR-Cas9 gene editing in Aspergillus calidoustus
Hollomon JM, Dahlstrom KM.
CRISPR-Cas9-mediated targeted gene deletion in Aspergillus calidoustus, a non-model environmental mold.
Microbiology Spectrum. 2026;14(6):e03899-25.
PMID: 42112836
Why this paper was selected
Most molecular understanding of pathogenic Aspergillus species comes from Aspergillus fumigatus. This study establishes a CRISPR-Cas9 gene-editing system for Aspergillus calidoustus, an emerging opportunistic mould with clinical relevance and reduced susceptibility to some antifungals.
Key findings
- The authors successfully developed a CRISPR-Cas9 platform for targeted gene deletion in A. calidoustus.
- The system provides a method for functional genetic studies in a previously less tractable species.
- The platform may support future research into virulence, environmental adaptation, antifungal resistance and novel drug targets.
Clinical significance
There is no immediate clinical application. However, the study is important as enabling science. As non-fumigatus Aspergillus species are increasingly recognised in clinical practice, tools that allow their biology to be studied directly may become increasingly valuable.
Implications for practice
Classification: Early-stage research requiring further validation.
This paper does not alter clinical management, diagnostics or guidelines. Its value lies in supporting future translational research.
Editorial assessment
This is a foundational research paper. It will not change patient care today, but it may help build the scientific infrastructure needed to understand emerging mould pathogens and their resistance mechanisms over the next decade.
Clinical pearl
7. Primary traumatic cutaneous aspergillosis caused by Aspergillus terreus
Ing SK, Lee YH, Tan YY, Aziz MBA, Chang AKW.
Primary traumatic cutaneous aspergillosis of the hand caused by Aspergillus terreus following a mould-contaminated penetrating injury.
Medical Mycology Case Reports. 2026;52:100798.
PMID: 42237979
Why this case was noted
This case report describes primary traumatic cutaneous aspergillosis of the hand caused by Aspergillus terreus following a mould-contaminated penetrating injury.
Clinical take-home points
- Aspergillosis is not always acquired through inhalation.
- Direct traumatic inoculation can cause localised Aspergillus infection.
- Persistent or atypical wounds following mould-contaminated trauma should prompt consideration of fungal infection.
- Tissue sampling is essential for diagnosis.
- Species-level identification matters because Aspergillus terreus is intrinsically resistant to amphotericin B.
Editorial assessment
This is not a practice-changing paper, but it is a useful educational case. It broadens clinical awareness beyond pulmonary aspergillosis and highlights the importance of early tissue diagnosis when wounds behave unexpectedly after contaminated trauma.
Overall editorial summary
The May 2026 literature contains several papers that are useful for clinicians and laboratory professionals working in aspergillosis and invasive mould disease. The strongest clinical themes are antifungal stewardship, drug exposure, azole resistance, and the continued importance of early diagnosis in high-risk populations.
The isavuconazole pharmacokinetic-pharmacodynamic study and the midostaurin-posaconazole interaction paper are particularly relevant because they address practical treatment decisions. The azole susceptibility study is highly relevant to clinical mycology laboratories and reinforces the need for careful interpretation of surrogate resistance testing. The invasive fungal sinusitis and transplant studies reinforce a familiar but important message: outcomes remain closely linked to early recognition, tissue diagnosis where appropriate, and multidisciplinary management.
Finally, the CRISPR-Cas9 paper and traumatic cutaneous aspergillosis case illustrate the breadth of modern aspergillosis research, from molecular tools for emerging moulds to unusual clinical presentations outside the respiratory tract.
References
- Guidi M, Couchepin J, Reinhold I, Kronig I, Neofytos D, Schreiber PW, André P, Buclin T, Lamoth F. Characterization of isavuconazole pharmacokinetics and pharmacodynamics in a real-life cohort. JAC Antimicrobial Resistance. 2026;8(3):dlag071. PMID: 42088097
- Joisten CS, Mellinghoff SC, Seidel D, Müller C, Müller-Ohrem C, Kreuzer K-A, Frenzel LP, Simon F, Hallek M, Koehler P, Cornely OA, Stemler J. Clinical impact of potential drug-drug interactions between midostaurin and posaconazole in FLT3-mutated AML. Antimicrobial Agents and Chemotherapy. 2026;70(6):e01951-25. PMID: 42118097
- Vahedi-Shahandashti R, Nickel A-S, Eisele D, Lass-Flörl C; ISHAM Working Group Member of Intrinsic Antifungal Resistance. Can voriconazole gradient diffusion testing results be extrapolated to isavuconazole and posaconazole in Aspergillus spp.? Comparative analysis with CLSI broth microdilution and cyp51A gene sequencing. Antimicrobial Agents and Chemotherapy. 2026;70(6):e01813-25. PMID: 42138696
- Athni TS, Strauch CB, Kovac V, Arbona-Haddad E, Villa IP, Gupta S, Aleissa MM, Liakos AD, Tong A, Vedula RS, Maxfield AZ, Bergmark RW, Sherman AC. Invasive fungal sinusitis in patients with hematological malignancies: a 20-year study from a tertiary academic US hospital system. Open Forum Infectious Diseases. 2026;13(6):ofag304. PMID: 42238379
- Sudhaharan S, Pamidimukkala U, Bojja S, Raju DSB, Kk R, Gopal PSS. Invasive mold infections among transplant recipients: a single-center observational study. Journal de Mycologie Médicale / Journal of Medical Mycology. 2026;36(2):101629. DOI: 10.1016/j.mycmed.2026.101629
- Hollomon JM, Dahlstrom KM. CRISPR-Cas9-mediated targeted gene deletion in Aspergillus calidoustus, a non-model environmental mold. Microbiology Spectrum. 2026;14(6):e03899-25. PMID: 42112836
- Ing SK, Lee YH, Tan YY, Aziz MBA, Chang AKW. Primary traumatic cutaneous aspergillosis of the hand caused by Aspergillus terreus following a mould-contaminated penetrating injury. Medical Mycology Case Reports. 2026;52:100798. PMID: 42237979
Article information
Prepared for: aspergillosis.org professionals section
Intended audience: healthcare professionals and researchers
Article type: monthly professional literature update
Coverage period: May 2026
Last reviewed: June 2026
Clinical Trials Update: Progress in ABPA and Invasive Aspergillosis Research
Date reviewed: 8 June 2026
Clinical research into aspergillosis continues to move forward, although there have been relatively few major new trial launches in recent weeks. The most significant developments involve two areas:
- Growing evidence supporting biologic treatment for Allergic Bronchopulmonary Aspergillosis (ABPA).
- Progress towards completion of a major international trial of a new antifungal drug for invasive aspergillosis.
Contents
- ABPA: More Evidence for Dupilumab
- Olorofim Trial Moves Towards Completion
- Why These Studies Matter
- What We Didn't Find This Month
- Common Questions
- When to Seek Medical Advice
ABPA: More Evidence for Dupilumab
One of the most encouraging developments in recent years has been the emergence of biologic therapies for ABPA. Researchers continue to publish and present results from the Phase II LIBERTY ABPA AIRED study, which investigated the biologic drug dupilumab.
Dupilumab works by blocking two important inflammatory pathways (Interleukin-4 and Interleukin-13) that contribute to allergic inflammation in asthma and ABPA.
Additional scientific presentations and publications appearing during 2025 and 2026 continue to show consistent benefits for many patients:
- Improved lung function.
- Fewer severe respiratory exacerbations.
- Reduced need for oral corticosteroids.
- Better asthma control.
- Improved quality of life.
- Reductions in total Immunoglobulin E (IgE) and Aspergillus-specific IgE levels.
Although biologics are not suitable for everyone with ABPA, these results continue to strengthen the evidence that targeted immune therapies may offer an alternative to long-term steroid treatment for some patients.
For people living with ABPA, this remains one of the most promising areas of current research.
Olorofim Trial Moves Towards Completion
The other major development concerns olorofim, a novel antifungal medication being developed for difficult-to-treat invasive fungal infections.
The large international Phase III OASIS trial has been comparing olorofim with standard treatment in patients with invasive aspergillosis.
Recent updates suggest that recruitment has now effectively closed and that the study is entering its final follow-up and analysis phase.
This is an important milestone because it usually means researchers have enrolled enough participants and are now collecting the final outcome data needed to determine whether the treatment works and how safe it is.
However, the most important information is still awaited:
- The primary trial results have not yet been published.
- No peer-reviewed Phase III paper is currently available.
- The effectiveness of olorofim compared with current standard treatments remains under formal evaluation.
If the final results are positive, olorofim could become an important additional treatment option for patients with invasive aspergillosis, particularly those whose infections are resistant to existing antifungal drugs or who cannot tolerate current therapies.
Why These Studies Matter
Research into aspergillosis has traditionally lagged behind many other respiratory and infectious diseases. It is therefore encouraging to see progress occurring in two key areas:
- Allergic disease (ABPA) – where biologics are offering the possibility of reducing steroid dependence.
- Invasive disease – where new antifungal drugs may help address drug resistance and treatment failure.
These studies also reflect a broader trend towards more personalised treatment approaches, matching therapies to the specific type of aspergillosis and the underlying immune response of the patient.
What We Didn't Find This Month
While there has been progress in ongoing studies, we did not identify any major new:
- ABPA clinical trials.
- Chronic Pulmonary Aspergillosis (CPA) treatment trials.
- Severe Asthma with Fungal Sensitisation (SAFS) interventional studies.
- Aspergillus bronchitis treatment trials.
- Major environmental intervention studies.
- Newly terminated or withdrawn aspergillosis drug-development programmes.
This is not unusual. Large clinical trials often take several years to complete, and periods of data analysis between recruitment and publication can be lengthy.
Common Questions
Is dupilumab available for ABPA?
Dupilumab is already licensed for several allergic and eosinophilic conditions, including some forms of severe asthma. Its use specifically for ABPA varies between countries and healthcare systems. Decisions about treatment remain highly individual and should be discussed with a specialist team.
What is a Phase III trial?
Phase III studies are large clinical trials designed to determine whether a new treatment works and how safe it is compared with existing treatments. Positive Phase III results are often required before regulatory approval.
Could olorofim be used for CPA?
Research has explored olorofim in a variety of fungal diseases, but the current Phase III programme focuses on invasive aspergillosis. Further evidence would be needed before routine use in Chronic Pulmonary Aspergillosis.
When might the OASIS results be available?
There is currently no confirmed publication date. As recruitment appears to have finished, the next major milestone will be release of the primary efficacy and safety results.
When to Seek Medical Advice
Clinical trial news is exciting, but it should not replace advice from your healthcare team.
Seek medical attention if you experience:
- Worsening breathlessness.
- New or worsening haemoptysis (coughing blood).
- Persistent fever.
- Sudden deterioration in asthma control.
- Significant side effects from antifungal or biologic treatments.
If you are interested in taking part in clinical research, speak with your specialist team about studies that may be available in your area.
Key Takeaway: The strongest current momentum in aspergillosis research remains in biologic treatments for ABPA and new antifungal therapies for invasive aspergillosis. While no major new trials have appeared this month, ongoing studies continue to move closer to delivering results that could influence future care.
Last reviewed: 8 June 2026

Aspergillosis Research Update: Week Ending 8 June 2026
Key Points
- This was a relatively quiet week for aspergillosis research, with few major new clinical studies.
- A review explored whether positive parasite blood tests in people with Allergic Bronchopulmonary Aspergillosis (ABPA) may represent true infection or immune cross-reactivity.
- Chronic Pulmonary Aspergillosis (CPA) continues to gain recognition as an important complication following tuberculosis.
- Researchers are investigating home monitoring technologies and microsampling approaches.
- Antifungal resistance remains an important area of global surveillance.
- A major review examined Aspergillus species beyond Aspergillus fumigatus.
Contents
- Can ABPA Be Confused with Parasitic Infections?
- Can Tuberculosis Lead to CPA?
- Could Home Blood Testing Help Aspergillosis Patients?
- What Is Antifungal Resistance?
- Are There Aspergillus Species Other Than Aspergillus fumigatus?
- New Aspergillus Research
- Other Interesting Publications
- What Does This Mean for Patients?
- When Should Patients Seek Medical Advice?
This week was dominated by review articles rather than major new clinical trials. While there were no obvious practice-changing breakthroughs, several useful papers provide updated summaries of important topics including ABPA diagnosis, Chronic Pulmonary Aspergillosis (CPA), antifungal resistance and future monitoring technologies.
These reviews help clinicians and researchers understand where the field currently stands and identify areas where further research is needed.
Can ABPA Be Confused with Parasitic Infections?
Our research highlight this week is a review by Mewara and colleagues examining the relationship between Allergic Bronchopulmonary Aspergillosis (ABPA) and parasitic worm (helminth) infections. Read the paper on PubMed.
ABPA and some parasitic infections can trigger remarkably similar immune responses, including:
- Very high Immunoglobulin E (IgE) levels
- Raised eosinophils
- Allergic inflammation
- Positive antibody tests
This can occasionally create diagnostic uncertainty. The authors discuss whether positive parasite blood tests in some patients with ABPA represent genuine infection, previous exposure or immune cross-reactivity caused by overlapping allergic responses.
Are parasitic infections common in the UK?
For most patients living in the UK, USA, Canada and much of Europe, parasitic worm infections remain relatively uncommon. However, doctors may consider them in people who have:
- Lived abroad
- Travelled extensively
- Worked overseas
- Been exposed to contaminated soil or freshwater in higher-risk regions
One parasite of particular interest is Strongyloides stercoralis, which can persist silently for many years and may become dangerous if someone receives high-dose steroids or other immunosuppressive treatments.
Take-home message: A positive blood test rarely tells the whole story. Symptoms, scans, blood tests and clinical history all contribute to making the correct diagnosis.
Can Tuberculosis Lead to CPA?
A large scoping review examining lung disease after tuberculosis highlighted the growing recognition of Chronic Pulmonary Aspergillosis (CPA) as an important and potentially treatable complication. Read the review on PubMed.
The review identified evidence that antifungal treatment can improve:
- Symptoms
- Radiological findings
- Markers of inflammation
Tuberculosis remains one of the most important risk factors for CPA worldwide.
Many people continue to experience symptoms after completing tuberculosis treatment, including:
- Breathlessness
- Persistent cough
- Fatigue
- Weight loss
- Haemoptysis (coughing up blood)
Increasingly, researchers recognise that some of these patients may have treatable Aspergillus-related disease rather than simply permanent lung damage.
Not all ongoing symptoms after tuberculosis are simply due to old lung damage. Some patients may have treatable Chronic Pulmonary Aspergillosis.
Could Home Blood Testing Help Aspergillosis Patients?
A review of respiratory biomarkers and patient-centred microsampling explored technologies that may eventually make monitoring chronic respiratory diseases easier and more convenient. Read the review on PubMed.
Areas under investigation include:
- Finger-prick blood testing
- Home sample collection
- Microsampling technologies
- Remote monitoring
- Personalised treatment optimisation
These approaches are particularly attractive for patients with long-term conditions who require regular monitoring.
Although still developing, they align closely with the wider move towards patient-centred care and remote monitoring.
What Is Antifungal Resistance?
A review from Japan examined azole-resistant Aspergillus species and their implications for patient care. Read the review on PubMed.
Azole antifungal drugs remain central to treatment for:
- Chronic Pulmonary Aspergillosis (CPA)
- Aspergillus bronchitis
- Invasive aspergillosis
The review highlights the continuing importance of:
- Fungal culture
- Susceptibility testing
- Therapeutic drug monitoring
- Clinical review when treatment is not working as expected
Resistance remains relatively uncommon in many patient groups but continues to be monitored closely worldwide.
Are There Aspergillus Species Other Than Aspergillus fumigatus?
Most patients are familiar with Aspergillus fumigatus, the species most commonly associated with lung disease.
However, a major review published in Clinical Microbiology Reviews examined the black aspergilli, including the Aspergillus niger complex. Read the review on PubMed.
While less common causes of lung disease, these fungi can also be associated with:
- Ear infections
- Nail infections
- Chronic pulmonary disease
- Rare invasive infections
The review serves as a useful reminder that Aspergillus is a large family of related fungi rather than a single organism.
New Aspergillus Research
One of the few original research studies highlighted this week investigated how Aspergillus fumigatus builds and repairs its cell wall. Read the study on PubMed.
The researchers explored how fungal growth is affected by antifungal drugs that target cell wall synthesis.
Although this laboratory work is unlikely to affect patient care immediately, it improves our understanding of how antifungal drugs work and may help identify future treatment targets.
Other Interesting Publications
- Fosmanogepix: A review of an emerging antifungal drug that may play a future role in treating resistant fungal infections. PubMed.
- ABPA and Eosinophilic Granulomatosis with Polyangiitis (EGPA): A rare case report describing overlapping eosinophilic disease and ABPA. PubMed.
- Hyper-IgE Syndrome and Pulmonary Aspergillosis: A case report highlighting fungal infection in a rare inherited immune disorder. PubMed.
What Does This Mean for Patients?
While this was not a week of major breakthroughs, the research reinforces several important messages:
- Diagnosing ABPA can sometimes be complicated because different conditions can produce similar immune responses.
- CPA remains an important and potentially treatable complication after tuberculosis.
- Future monitoring technologies may allow more care to take place at home.
- Antifungal resistance continues to be monitored closely worldwide.
- Research into Aspergillus biology continues to support the development of future treatments.
When Should Patients Seek Medical Advice?
Patients should contact their healthcare team if they experience:
- Increasing breathlessness
- Coughing up blood
- Persistent fever
- Unexplained weight loss
- New chest pain
- A significant increase in sputum production
- New or worsening treatment side effects
Anyone with a history of living or travelling in regions where parasitic infections are common should mention this to their healthcare team before starting high-dose steroid treatment.
Review Information
Last reviewed: 8 June 2026
Prepared for: Aspergillosis.org Weekly Research Update
Audience: Patients, carers and non-specialist readers
This article summarises recently published research. Research findings may take years to influence routine clinical practice and should not replace personalised medical advice from your healthcare team.
```

Help Us Improve Our Damp Homes and Health Questionnaire

We are asking patients, carers and members of the public to help us improve a draft questionnaire for our new UK Citizen Science project on damp homes, mould and health.
Draft 1 of questionnaire download here: Health Effects of Indoor Mould Questionnaire
Key points
- We are developing a questionnaire for a Citizen Science project about damp homes, mould and health.
- Before using it in the study, we want feedback from people who may complete it.
- We are not just asking people to check spelling or grammar.
- We want to know whether the questionnaire asks the right questions, is easy to understand, and collects useful information.
- Your comments can help shape the final version of the study.
Why are we doing this project?
Damp homes and indoor mould are common problems in the UK. Many people worry that dampness, condensation and mould may affect their breathing, allergies, infections, fatigue or general wellbeing.
Our Citizen Science project aims to learn more about the links between homes, indoor mould and health by working directly with patients, carers and householders.
Citizen Science means that members of the public are not just research subjects. They help shape the research, collect information, and improve the questions being asked.
What is the questionnaire for?
The questionnaire is designed to collect information about:
- the type of home someone lives in
- signs of damp, condensation or mould
- heating and ventilation
- previous water damage, leaks or flooding
- respiratory symptoms and other health problems
- whether symptoms seem to change in different environments
- how damp or mould affects everyday life and wellbeing
This information will help researchers understand whether there are patterns between housing conditions and health. It will also help guide the next stages of the project, including possible home sampling and laboratory analysis.
Why do we need feedback?
A questionnaire can look clear to researchers but feel very different to the people completing it.
Patients and householders may notice:
- questions that are confusing
- questions that are too difficult to answer
- important topics that are missing
- sections that feel repetitive
- questions that need a “Don’t know” option
- places where more explanation is needed
This is why your feedback is so important.
What sort of comments are we looking for?
We are especially interested in comments on the following areas.
1. Is the questionnaire easy to understand?
Please tell us if any wording is unclear, too technical, or open to different interpretations.
2. Are any important questions missing?
For example, should we ask more about:
- previous mould exposure in other homes
- roof leaks, plumbing leaks or flooding
- diagnosed respiratory conditions
- asthma, allergic bronchopulmonary aspergillosis, chronic pulmonary aspergillosis or other lung conditions
- steroid treatment or immune-suppressing medicines
- whether symptoms improve away from home
- whether symptoms changed after moving house
3. Is the questionnaire too long?
Long questionnaires can be tiring, especially for people living with chronic illness. We want to collect enough information to make the study useful, but not so much that people give up before finishing.
4. Are any questions difficult to answer accurately?
Some people may not know exact details about their home, heating system, building age or past water damage. We want to identify questions where people may need clearer options, such as “Not sure” or “Don’t know”.
5. Are any questions sensitive?
Questions about housing, health and personal circumstances can sometimes feel sensitive. Please tell us if any question needs a clearer explanation of why it is being asked.
The most important question
One of the most useful questions we can ask is:
If this study could answer one question about damp homes, mould and health, what would you most like to know?
This helps us understand what matters most to patients, carers and householders.
How to send us your comments
Click here for a short Google Form where you can send your feedback.
The feedback form will ask questions such as:
- How easy was the questionnaire to understand?
- Were any questions unclear or confusing?
- Do you think any important questions are missing?
- Were any questions unnecessary or repetitive?
- Was the questionnaire too long, too short, or about right?
- If this study could answer one question about damp homes, mould and health, what would you most like to know?
- Do you have any other comments or suggestions?
You do not need to answer every question. Any feedback is helpful.
This is not a grammar exercise
We are not mainly asking people to proofread the questionnaire.
What we really want to know is:
Does this questionnaire help us collect the information needed to understand whether damp homes and mould may be affecting health, and are we asking the right questions?
Thank you
Thank you for helping us improve this questionnaire. Your comments will help us design a better study and make sure the project reflects the experiences and priorities of the people affected by damp homes and mould.
By sharing your views at this early stage, you are helping shape research that could improve understanding of indoor mould, housing conditions and health.
```

The Power of Keeping a Health Diary When You Have Aspergillosis
Last reviewed: June 2026
Audience: People living with aspergillosis, families and carers
Key points
- A health diary can help you understand symptoms, triggers and changes over time.
- It can be especially useful if you experience fatigue, brain fog or memory problems.
- It can make clinic appointments more focused and productive.
- A diary may show progress that is hard to notice day to day.
- The best diary is simple, quick and realistic to keep using.
Contents
- Why keep a health diary?
- How it can help with aspergillosis
- Brain fog and memory
- Spotting patterns and triggers
- Using your diary at appointments
- The psychological benefit
- Simple diary template
- Common questions
- When to seek medical advice
Why keep a health diary?
Living with aspergillosis often means symptoms change from day to day. Some days may be manageable. Others may involve more coughing, breathlessness, fatigue, sinus symptoms, poor sleep or medication side effects.
Because these changes can happen gradually, it can be difficult to remember exactly when symptoms started, whether they are getting better or worse, or what might have triggered them.
A health diary gives you a simple record of what is happening over time. It can help you, your family and your healthcare team see patterns that may not be obvious from memory alone.
How a diary can help with aspergillosis
People with aspergillosis may find it useful to record:
- Cough
- Breathlessness
- Fatigue
- Sputum or phlegm
- Wheeze
- Sinus symptoms
- Sleep quality
- Exercise or walking distance
- Mood and wellbeing
- Medication changes
- Possible side effects
You may also want to note possible triggers, such as damp or mould exposure, pollen, dusty environments, changes in weather, respiratory infections, stress, travel or changes in medication.
Brain fog and memory
Many people with long-term lung conditions describe episodes of brain fog. This may feel like forgetfulness, poor concentration, difficulty finding words, feeling mentally slower than usual, or feeling as though your head is “empty”.
Brain fog can have many possible causes, including fatigue, poor sleep, infection, inflammation, stress, anxiety, pain, medication side effects, low oxygen levels or other health problems.
A diary acts as an external memory. Instead of trying to remember when something changed, you can look back and see what was happening at the time.
Spotting patterns and triggers
| What you record | What it may help show |
|---|---|
| Symptoms | Whether cough, breathlessness or fatigue are improving or worsening |
| Sleep | Whether poor sleep is linked to worse symptoms |
| Exercise | What level of activity is manageable |
| Weather | Whether heat, humidity, cold air or storms affect symptoms |
| Environment | Possible links with damp, mould, dust or pollen |
| Medication | Possible benefits, side effects or changes during dose reduction |
| Infections | Early warning signs or repeated patterns |
Using your diary at appointments
Healthcare professionals may ask questions such as:
- When did your symptoms start?
- Are they getting better or worse?
- Have you noticed any triggers?
- Have you changed any medication recently?
- How far can you walk now compared with before?
- Have you had any infections or courses of antibiotics?
These questions are not always easy to answer from memory, especially when you are tired or anxious. A diary can help you give clearer, more accurate information.
You may find it useful to bring a short summary to your appointment, such as:
- Three things that have improved
- Three things that have worsened
- Any medication changes
- Your main questions for the appointment
Sometimes the diary tells a different story
When you have had a difficult few days, it can feel as though nothing is improving. A diary may show that the wider picture is more encouraging.
For example, you may feel:
“Nothing has changed.”
But your diary may show:
- You are walking further than three months ago
- You are sleeping better
- You have had fewer chest infections
- You are coughing less at night
- You are doing more social activities
Equally, a diary can show gradual deterioration that might otherwise be missed. Both types of information can be useful.
The psychological benefit
Chronic illness can feel unpredictable. A diary can help restore a sense of control by changing the question from:
“Why do I feel awful?”
to:
“What changed recently?”
This can reduce uncertainty and help you feel more involved in your care.
A diary can also become a record of resilience. It may include difficult days, but it can also capture walks completed, holidays taken, family events attended, personal goals reached and challenges overcome.
Keep it simple
Many people stop keeping a diary because they try to record too much. A simple diary is usually more useful than a complicated one.
A daily entry might take less than two minutes and include:
- Symptoms, scored from 0 to 10
- Energy level, scored from 0 to 10
- Sleep quality
- Exercise or activity
- Medication changes
- Anything unusual
Consistency matters more than detail.
Paper, phone or app?
There is no single correct way to keep a diary. You could use:
- A notebook
- A printed diary sheet
- A phone notes app
- A calendar
- Voice notes
- A spreadsheet
- A symptom tracking app
- A fitness tracker or smartwatch
The best diary is the one you will actually use.
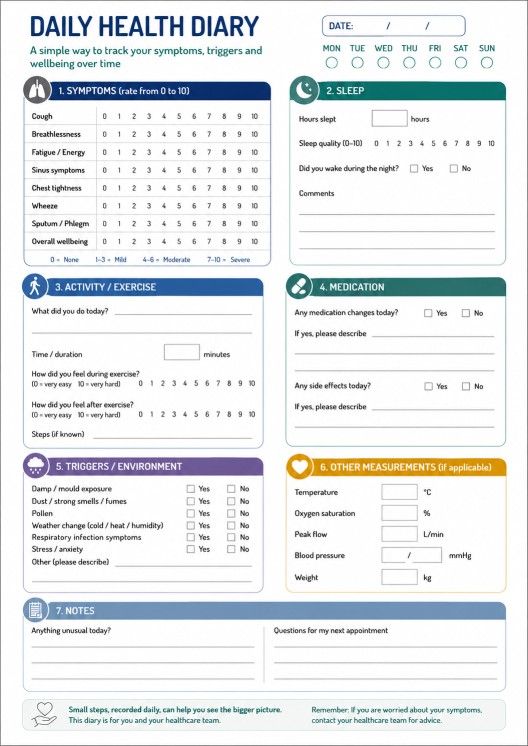
Simple diary template
Daily health diary
Date: __________________________
Symptoms, 0–10
Cough: ______
Breathlessness: ______
Fatigue: ______
Sinus symptoms: ______
Overall wellbeing: ______
Sleep
Hours slept: ______
Sleep quality, 0–10: ______
Activity
Exercise or activity today:
__________________________________________________
Medication
Any medication changes or side effects?
__________________________________________________
Notes
Anything unusual today?
__________________________________________________
__________________________________________________
Daily Diary - PDF downloadable
Common questions
Do I need to write every day?
No. Some people write daily. Others only record changes, flare-ups, medication changes or important events.
What if I forget for a few days?
That is very common. Simply restart when you remember. A diary does not have to be perfect to be useful.
Should I record test results?
You can if you find it helpful. Some people record blood results, oxygen saturations, lung function, weight, clinic letters or medication levels. Do not worry if this feels too much. A simple symptom diary is still useful.
Can a diary replace medical advice?
No. A diary is a tool to support conversations with your healthcare team. It should not be used to diagnose or treat symptoms without medical advice.
When to seek medical advice
Seek medical advice promptly if you experience:
- Sudden or significant worsening of breathlessness
- Coughing up large amounts of blood
- Persistent fever
- Severe chest pain
- New confusion or rapidly worsening brain fog
- Weakness, speech problems, facial drooping or visual changes
- Symptoms that are worsening quickly or feel unusual for you
If you are unsure, contact your healthcare team, NHS 111, your GP, or emergency services depending on severity.
Further information
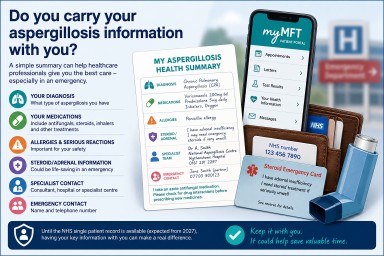
Do You Carry Your Aspergillosis Information With You?

New NHS Plans Could Help in Future – But What About Today?
The UK government is currently debating plans for a new NHS “single patient record” system. The aim is to allow authorised healthcare professionals to access important information from GP surgeries, hospitals, community services and other parts of the NHS more easily.
If implemented successfully, this could reduce the need for patients to repeatedly explain their medical history and could help emergency departments, ambulance crews and other healthcare professionals see important information such as diagnoses, medications, allergies and previous treatment.
For people living with aspergillosis and other long-term respiratory conditions, this could be especially valuable. However, these changes will take time to develop and introduce. For now, patients remain one of the most important links between different parts of the healthcare system.
Why This Matters for Aspergillosis Patients
Many people with aspergillosis receive care from several different services, including:
- General Practitioners (GPs)
- Local respiratory teams
- Specialist nurses
- Hospital clinics
- Emergency departments
- Pharmacists
- Community healthcare teams
- Specialist centres such as the National Aspergillosis Centre
Healthcare records are not always immediately available to every professional involved in your care. This means there may be times when you need to explain:
- What type of aspergillosis you have
- Which medications you take
- Any important allergies or serious drug reactions
- Whether you have adrenal insufficiency or take long-term steroids
- Who your specialist team is
- What previous treatments you have received
Having this information readily available can save time and may help healthcare professionals make decisions more quickly and safely.
What Information Should You Carry?
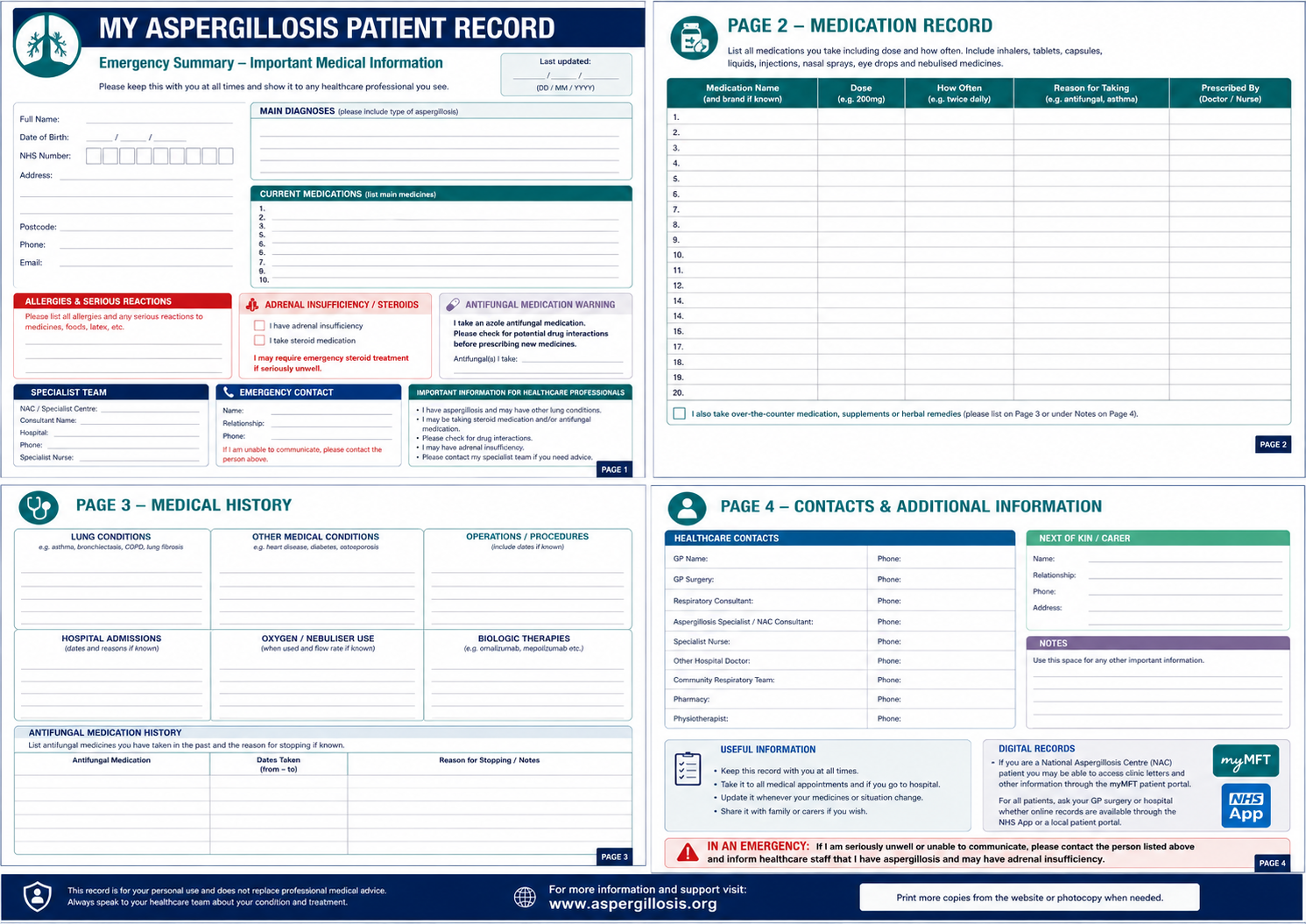 You do not need to carry your entire medical record. A simple one-page health summary is usually enough.
You do not need to carry your entire medical record. A simple one-page health summary is usually enough.
1. Your Diagnosis
List your main diagnoses clearly. Examples include:
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Chronic Pulmonary Aspergillosis (CPA)
- Severe Asthma with Fungal Sensitisation (SAFS)
- Aspergillus Bronchitis
- Bronchiectasis
- Severe Asthma
- Chronic Obstructive Pulmonary Disease (COPD)
2. Your Current Medications
Include all current treatments, particularly:
- Antifungal medications, such as itraconazole, voriconazole, posaconazole or isavuconazole
- Steroid tablets
- Hydrocortisone replacement therapy
- Biologic therapies
- Inhalers
- Oxygen therapy
- Antibiotics you are currently taking
Try to keep this list up to date.
3. Drug Allergies and Serious Reactions
This is one of the most important sections. Include any known allergies or serious reactions, for example:
- Penicillin allergy
- Prednisolone allergy
- Previous severe drug reactions
- Medicines you have been told to avoid
4. Steroid or Adrenal Information
If you have adrenal insufficiency or are taking long-term steroid treatment, make this very clear.
I have adrenal insufficiency and may require emergency steroid treatment if seriously unwell.
Many patients already carry a steroid emergency card. If you have been advised to carry one, continue to carry it at all times.
5. Specialist Contact Information
Include:
- Consultant name
- Hospital or specialist centre
- Clinic or specialist nurse contact details, if available
6. Emergency Contact
Include:
- Name
- Relationship
- Telephone number
An Important Extra Note for Aspergillosis Patients
Many antifungal medications interact with other medicines. If you take itraconazole, voriconazole, posaconazole or isavuconazole, consider including the following statement on your health summary:
I take an azole antifungal medication. Please check for potential drug interactions before prescribing new medicines.
This simple statement may help avoid medication-related problems.
If You Are a National Aspergillosis Centre Patient: Using myMFT
If you are a patient of the National Aspergillosis Centre (NAC), you may already have access to some of your hospital information through the myMFT patient portal.
myMFT is the patient portal used by Manchester University NHS Foundation Trust (MFT), which includes Wythenshawe Hospital and the National Aspergillosis Centre.
Depending on the services you use, myMFT may allow you to:
- View MFT appointment details
- Access clinic letters
- Keep track of important test results, letters and health information
- Attend online video consultations
- Use proxy access to help manage a family member’s healthcare, with consent
Many patients find it useful to keep copies of important clinic letters on their phone or tablet. This can be particularly helpful if you attend another hospital, visit your GP, travel away from home or need emergency treatment.
myMFT does not replace a future NHS-wide patient record, but it can provide access to important information that may help you and your healthcare professionals manage your care more effectively.
Find out more about myMFT on the Manchester University NHS Foundation Trust website.
For Patients Not Under the National Aspergillosis Centre
If you are not an NAC or MFT patient, your local hospital may have its own patient portal or online record system. Ask your hospital clinic, respiratory team or GP surgery whether you can access clinic letters, appointment information or test results online.
You may also be able to use the NHS App to manage parts of your healthcare, depending on your GP surgery and local NHS services.
Find out more about the NHS App.
You may also find it useful to know your NHS number. You do not need to know your NHS number to receive NHS care, but it can be helpful when contacting services or completing forms.
Where Should You Keep Your Information?
Many patients choose to:
- Save a copy on their mobile phone
- Keep a printed copy in their wallet or handbag
- Store it alongside their steroid emergency card
- Keep a copy with travel documents
- Share a copy with family members or carers
- Keep copies of important clinic letters on their phone or tablet
The best system is the one that is easy to access when needed.
Printable options (Word documents):
Looking Ahead
The proposed NHS single patient record could eventually make it easier for healthcare professionals to access important information quickly and safely.
For patients with rare conditions such as aspergillosis, that could improve continuity of care, reduce delays and reduce the need to repeatedly explain complex medical histories.
Until then, carrying a simple summary of your condition remains one of the easiest and most effective ways to help healthcare professionals understand your health needs and provide appropriate care.
Key Points
- Carry a simple one-page health summary.
- Include diagnoses, medications, allergies and specialist contacts.
- Clearly state if you have adrenal insufficiency or take long-term steroids.
- Mention azole antifungal treatment and potential drug interactions.
- National Aspergillosis Centre patients may be able to access clinic information through myMFT.
- Patients outside MFT should ask whether their own hospital has a patient portal.
- Keep important information on your phone and consider carrying a printed copy.
- A future NHS single patient record may improve information sharing, but patients remain an important source of information today.
Common Questions
Do I need to carry all my clinic letters?
No. A concise one-page summary is usually more useful in an emergency. However, keeping copies of important clinic letters on your phone can be helpful.
What if I am treated at more than one hospital?
This is one of the main reasons to carry a health summary. Different healthcare providers may not always have immediate access to the same information.
Is this only useful in emergencies?
No. It can also help during GP appointments, outpatient visits, travel, planned hospital admissions and when seeing healthcare professionals unfamiliar with aspergillosis.
What if I am a National Aspergillosis Centre patient?
Consider registering for myMFT and keeping important clinic letters available on your phone or tablet for easy access.
What if I am not an NAC patient?
Ask your own hospital or respiratory clinic whether they offer a patient portal. You can also check what information is available through the NHS App.
When to Seek Medical Advice
Seek urgent medical advice if you experience:
- Significant worsening of breathlessness
- Chest pain
- Coughing up significant amounts of blood
- Symptoms of adrenal crisis if you have adrenal insufficiency
- Severe allergic reactions to medications
- Rapid deterioration in your respiratory symptoms
If you need emergency help, call 999. For urgent medical advice in the UK, use NHS 111.
Useful Links
- myMFT patient portal – Manchester University NHS Foundation Trust
- NHS App
- Find your NHS number
- Aspergillosis information and support
Frequently Asked Questions
What information should an aspergillosis patient carry in an emergency?
Patients should consider carrying a summary of their diagnosis, medications, allergies, steroid or adrenal information, specialist contacts and emergency contact details.
Should people with aspergillosis carry a medication list?
Yes. Many aspergillosis patients take antifungal medicines, steroids, biologic therapies and inhalers. An up-to-date medication list can help avoid prescribing errors and drug interactions.
What is myMFT?
myMFT is the patient portal used by Manchester University NHS Foundation Trust. It allows eligible patients to access appointments, clinic letters, test results and other healthcare information.
Can aspergillosis patients access their records online?
Some patients can access records through services such as myMFT, local hospital portals or the NHS App, depending on where they receive care.
What is the NHS single patient record?
The proposed NHS single patient record aims to improve information sharing between healthcare providers so patients do not need to repeatedly explain their medical history.
Author: National Aspergillosis Centre Patient Support Team
Reviewed by: National Aspergillosis Centre
Last reviewed: June 2026
Important: This article is intended for information only and should not replace advice from your healthcare team.

Exercise and Aspergillosis: How Physical Activity Can Improve Breathing, Strength and Wellbeing
Key points
- Exercise is one of the most helpful non-drug tools for many people living with aspergillosis.
- Regular physical activity can improve breathlessness, strength, stamina, mood, confidence and quality of life.
- The best approach is usually little and often, rather than occasional intensive exercise.
- Do not compare yourself with others. Everyone has different lungs, treatments, fitness levels and limits.
- Respiratory physiotherapists and pulmonary rehabilitation programmes can help you exercise safely and confidently.
- Walking, cycling, swimming, rowing, gentle yoga, Tai Chi and singing can all be useful, depending on the individual.
- People with aspergillosis should take extra care around mould-heavy environments such as compost, leaf mould, sheds and building dust.
Contents
- Why exercise matters in aspergillosis
- The activity and breathlessness cycle
- Benefits of exercise
- Specific issues for aspergillosis patients
- How to start safely
- Activities that may help
- Pulmonary rehabilitation and physiotherapy
- The golden rule: little and often
- What clinicians want patients to know
- Real-life examples
- When to seek medical advice
- Frequently asked questions
- Related articles and further support
Why exercise matters in aspergillosis
Living with aspergillosis can be physically and emotionally challenging. Breathlessness, coughing, fatigue, disturbed sleep, medication side effects and reduced confidence can all make it tempting to become less active.
Unfortunately, becoming less active can make symptoms feel worse over time. Muscles weaken, fitness falls, balance may worsen and everyday activities such as walking, climbing stairs, shopping or playing with grandchildren can become harder.
This process is often called deconditioning. It does not mean the symptoms are imaginary. It means the body has lost some of its ability to cope with activity.
The encouraging news is that exercise can help reverse part of this process.
Exercise cannot cure aspergillosis, but it can help the body use oxygen more efficiently, strengthen muscles, improve confidence and make daily life easier.
Importantly, people may feel better and do more even when their lung function tests do not change very much.
The activity and breathlessness cycle
Many people with chronic lung disease become trapped in a difficult cycle:
The deconditioning cycle
Breathlessness → Less activity → Loss of fitness → More breathlessness → Even less activity
Exercise helps by creating a healthier cycle:
The rebuilding cycle
Gentle activity → Stronger muscles → More confidence → Easier daily tasks → Better quality of life
This is why small, regular activity can be so powerful. The aim is not to force the lungs to work harder. The aim is to help the whole body work better.
Benefits of exercise
Improved breathlessness
Exercise may make you breathless while you are doing it, but regular activity often reduces breathlessness during everyday tasks. This happens because muscles become stronger and more efficient, so they need less effort to perform the same activity.
More energy
Many patients report feeling less tired once they build a regular routine. Exercise uses energy in the short term, but over time it can improve stamina and reduce the effort needed for daily life.
Stronger muscles
Long-term illness, hospital admissions, inactivity and corticosteroid treatment can all contribute to muscle weakness. Strength exercises can help rebuild leg strength, improve balance and support independence.
Better mood and confidence
Living with aspergillosis can affect mental wellbeing. Exercise can help reduce anxiety, stress and low mood. It can also restore a sense of control and achievement.
Improved bone health
This is especially important for people who have taken long-term corticosteroids. Weight-bearing activity and strength training can help protect bone strength and reduce the risk of osteoporosis.
Better daily function
For many patients, the most important benefit is practical: being able to walk further, climb stairs more easily, go shopping, travel, garden, socialise or enjoy family life with more confidence.
Specific issues for aspergillosis patients
Avoiding high mould exposure
Aspergillus is commonly found in soil, compost, decaying vegetation, damp buildings and dust. Some activities can expose people to large numbers of fungal spores.
Activities that may increase exposure include:
- Handling compost
- Turning soil
- Clearing leaf piles
- Wood chipping
- Spreading bark or mulch
- Cleaning sheds, garages, lofts or basements
- Working around mouldy materials
- Construction or demolition environments
Outdoor exercise such as walking, cycling and running is generally encouraged. However, it is sensible to avoid places where mould, compost, dust or decaying vegetation are being heavily disturbed.
Some people may choose to wear a well-fitting FFP2 or FFP3 mask for unavoidable dusty or mould-heavy tasks, but avoidance is usually better where possible.
Haemoptysis: coughing blood
People with Chronic Pulmonary Aspergillosis (CPA), lung cavities or aspergillomas may sometimes cough blood. This is called haemoptysis.
If you have recent, recurrent or significant haemoptysis, discuss exercise with your respiratory team. Most routine activity remains safe for many people, but vigorous exertion may need to be paused or modified during periods of active bleeding.
Oxygen levels
Some people with aspergillosis also have bronchiectasis, Chronic Obstructive Pulmonary Disease (COPD), fibrosis, previous tuberculosis damage or other lung scarring. In these situations, oxygen levels may fall during exertion even when resting oxygen levels are normal.
If breathlessness feels out of proportion, or if you notice unusually low oxygen saturations during activity, discuss this with your respiratory team. You may benefit from an exercise assessment or pulmonary rehabilitation referral.
Fatigue and boom-and-bust activity
Aspergillosis-related fatigue can be different from normal tiredness. It may be influenced by chronic inflammation, active infection, poor sleep, anxiety, medication side effects and reduced fitness.
Many patients experience a boom-and-bust pattern:
Good day → Do too much → Several days recovering
Regular, steady activity is usually more helpful than occasional bursts of intensive effort.
Steroid-related muscle weakness
People who have taken long-term corticosteroids may develop muscle weakness, particularly around the thighs and hips. This can make standing from a chair, climbing stairs and walking uphill more difficult.
Strength exercises such as sit-to-stands, step-ups and resistance band work can be particularly helpful.
Adrenal insufficiency
Some patients who have used long-term corticosteroids develop adrenal insufficiency. These patients should understand their sick day rules and discuss unusually strenuous exercise, endurance events or major hikes with their healthcare team.
Most routine gentle or moderate exercise is safe, but unusually demanding activity may require additional planning.
Asthma, ABPA and exercise symptoms
Many people with Allergic Bronchopulmonary Aspergillosis (ABPA) also have asthma. Exercise can sometimes trigger wheeze, cough or chest tightness.
This does not usually mean exercise should be avoided. Good asthma control, appropriate inhaler use, gradual warm-up and pacing can make a major difference. Speak to your healthcare team if exercise regularly triggers asthma symptoms.
How to start safely
Start from where you are
Your starting point is your starting point. It does not matter what someone else can do. If you can only walk for two or three minutes, that is still a valid place to begin.
Use the talk test
During moderate exercise, you should usually be able to speak in short sentences. If you cannot speak at all, you may be pushing too hard.
Build gradually
Small increases are usually safer and more sustainable than sudden changes. For example, increasing a walk from five minutes to six or seven minutes may be more helpful than trying to double it immediately.
Plan rest periods
Rest is not failure. Many people with lung disease do better with short bursts of activity separated by planned rests.
Track progress gently
Some patients find it motivating to keep a simple record of walks, steps, strength exercises or how breathless they feel. The aim is encouragement, not pressure.
A simple beginner example
Example starter plan
- Week 1–2: Walk for 5 minutes most days, or less if needed.
- Week 3–4: Add one or two minutes when comfortable.
- Week 5–6: Add gentle strength exercises, such as sit-to-stands.
- Ongoing: Continue gradual increases, with rest days when needed.
This is only an example. Some people will need to start lower, while others may safely start higher.
Activities that may help
The best exercise is usually the one you enjoy and can keep doing regularly.
Walking
Walking is one of the simplest and most effective activities. It requires no special equipment, can be adapted to most fitness levels and is easy to build gradually.
Cycling
Cycling, including use of a stationary exercise bike, can improve stamina while placing less strain on the joints than running.
Swimming
Swimming can be helpful because the water supports body weight. However, some people with asthma find chlorinated pools trigger symptoms.
Rowing
Rowing machines can provide both cardiovascular and strength benefits. Start gently and focus on technique.
Strength training
Strength training does not have to mean heavy weights. Useful exercises may include:
- Sit-to-stands from a chair
- Step-ups
- Wall push-ups
- Resistance bands
- Light hand weights
Gentle yoga and Tai Chi
Many patients enjoy gentle yoga or Tai Chi because they combine movement, balance, breathing awareness, posture and relaxation. Chair-based versions may be useful for people with reduced mobility.
Singing
Singing may not sound like exercise, but many people with lung conditions find it helpful. It can support breathing control, posture, confidence, social connection and respiratory muscle coordination.
Some patients enjoy local choirs or Singing for Lung Health groups.
Pulmonary rehabilitation and physiotherapy
You do not have to do this alone.
A respiratory physiotherapist can help assess your current ability and design a programme that suits your symptoms, fitness level and goals.
A specialist physiotherapist may help with:
- Breathlessness management
- Pacing strategies
- Strength and stamina building
- Airway clearance techniques where appropriate
- Confidence around movement
- Safe return to activity after illness
Pulmonary rehabilitation
Pulmonary rehabilitation is a structured programme that usually combines supervised exercise, education, breathing techniques and self-management advice.
Many people with chronic lung disease describe pulmonary rehabilitation as one of the most helpful interventions they have received.
If you have ongoing breathlessness, reduced exercise tolerance or loss of confidence, ask your GP, respiratory consultant, specialist nurse or physiotherapist whether pulmonary rehabilitation may be suitable for you.
The golden rule: little and often
Exercise with aspergillosis: the golden rule
Little and often is usually better than a lot all at once.
Do not compare yourself with other people, including other aspergillosis patients.
Everyone has different lungs, different treatments, different ages and different levels of fitness.
Focus on your own starting point and your own progress.
Do not try to keep up with others. You do you.
One of the biggest traps is comparing yourself with other patients. Someone else may complete a long-distance walk, climb a mountain, run a race or cycle hundreds of miles. That can be inspiring, but it should not become your target.
Instead, ask yourself:
Am I a little stronger, fitter or more confident than I was a few months ago?
Success may mean:
- Walking for five minutes when previously you could only manage three
- Climbing stairs more comfortably
- Shopping with less breathlessness
- Doing light gardening safely
- Enjoying a holiday more easily
- Playing with children or grandchildren
- Needing fewer rests during ordinary daily tasks
These achievements matter.
For most people living with aspergillosis, consistency beats intensity.
What clinicians want patients to know
Exercise is not about pushing through at all costs
Healthcare professionals usually want patients to remain as active as safely possible, but that does not mean ignoring symptoms or forcing yourself to keep up with others.
The safest approach is usually to build gradually, pace yourself and ask for help when symptoms change.
Exercise should support your life, not punish your body.
Real-life examples
The person who walks five minutes a day
For someone recovering from illness or a hospital admission, a five-minute daily walk may be a major achievement. If that becomes six minutes, then eight minutes, that is progress.
The person who completes a long-distance walk
Some people with aspergillosis manage major challenges such as long-distance walking routes. These stories can be inspiring, but they are not a standard everyone else must meet.
The person who joins a singing group
For some patients, a singing group may be more enjoyable and sustainable than a gym. Singing can support breathing control and confidence while also providing social contact.
The person who returns to gardening carefully
Gardening can be enjoyable and active, but compost, leaf mould and disturbed soil may contain high levels of fungal spores. Some patients adapt by avoiding compost handling, asking for help with mould-heavy tasks, wearing protective masks where appropriate, and choosing lower-risk gardening activities.
When to seek medical advice
Stop exercising and seek medical advice if you experience:
- Chest pain
- Severe or unusual breathlessness
- Dizziness or fainting
- Significant haemoptysis, meaning coughing blood
- Sudden worsening of symptoms
- New palpitations or heart rhythm symptoms
- Oxygen levels much lower than usual, if you monitor them
- Exercise tolerance that suddenly falls without an obvious reason
Always speak to your healthcare team if you are unsure whether exercise is safe for you, especially if your symptoms have recently changed.
Frequently asked questions
Can I exercise if I have aspergillosis?
Yes, many people with aspergillosis benefit from regular physical activity. Exercise should be adapted to your symptoms, fitness level and medical conditions. Ask your healthcare team for advice if you have severe breathlessness, recent haemoptysis or unstable symptoms.
Can exercise improve breathlessness?
Yes. Exercise can improve muscle efficiency, stamina and confidence. This can reduce breathlessness during everyday activities, even if lung function test results do not change significantly.
What is the best exercise for Allergic Bronchopulmonary Aspergillosis?
There is no single best exercise for Allergic Bronchopulmonary Aspergillosis. Walking, cycling, swimming, gentle yoga, strength training and pulmonary rehabilitation can all be helpful. The best activity is one you can do safely and regularly.
Can pulmonary rehabilitation help aspergillosis patients?
Many people with chronic respiratory symptoms, bronchiectasis or reduced exercise tolerance benefit from pulmonary rehabilitation. It combines supervised exercise, education, breathing techniques and self-management support.
Should people with aspergillosis avoid gardening?
Not necessarily, but some gardening activities can expose people to high levels of Aspergillus spores. Handling compost, turning soil, clearing leaves and working with mulch may carry higher exposure. Lower-risk gardening activities may be more suitable for some patients.
Can exercise help steroid-related muscle weakness?
Yes. Strength exercises can help rebuild muscle strength lost through long-term corticosteroid treatment, illness or inactivity. Simple exercises such as sit-to-stands, step-ups and resistance bands can be useful.
Is singing useful for people with lung disease?
Many people with lung disease find singing helpful for breathing control, posture, confidence and social connection. Some areas offer Singing for Lung Health groups.
Should I exercise when I am tired?
Gentle movement may help on some tired days, but severe fatigue may mean your body needs rest. Pacing is important. Try to avoid repeated boom-and-bust cycles where you do too much on a good day and then need several days to recover.
Take-home message
Exercise is one of the most powerful tools available to help people living with aspergillosis maintain independence, strength and quality of life.
Move more, but move at your own pace.
Find something you enjoy.
Ask for help when you need it.
Little and often beats heroic efforts.
Do not compare yourself with others.
You do you.
Related articles
You may also find these aspergillosis.org articles helpful:
- Why Am I Breathless When My Oxygen Levels Are Normal?
- Physiotherapy for Aspergillosis
- Living with Aspergillosis
- Managing Fatigue in Aspergillosis
- Steroids and Adrenal Insufficiency
- Bronchiectasis and Aspergillosis
- What is Allergic Bronchopulmonary Aspergillosis (ABPA)?
- What is Chronic Pulmonary Asprgillosis (CPA)?
Further support and information
Author and review information
Author: Graham Atherton, National Aspergillosis Centre
Medical review: National Aspergillosis Centre Clinical Team
Last reviewed: June 2026
This article provides general information and should not replace advice from your own healthcare team.
Specialist Evidence Briefing: Aspergillus Serology for CPA Diagnosis: Why Assay Choice, Cut-Offs and Confirmatory Testing Matter
Key points
- CPA diagnosis remains challenging because symptoms and radiology overlap with tuberculosis, non-tuberculous mycobacterial disease, bronchiectasis, chronic obstructive pulmonary disease, malignancy and other chronic lung disorders.
- Aspergillus immunoglobulin G (IgG) testing is a cornerstone of CPA diagnosis, but performance varies between assays.
- Cut-off selection affects sensitivity and specificity, with important consequences for both missed CPA and overdiagnosis.
- Confirmatory or complementary testing, such as Western blot in selected situations, may help clarify difficult or borderline cases.
- The paper is directly relevant to specialist respiratory, infectious diseases and mycology services because diagnostic reliability affects referral pathways, antifungal prescribing and case definition.
The paper
Bigot J, Gibert C, Millet N, et al. Aspergillus serology for chronic pulmonary aspergillosis diagnosis: optimization of an enzyme-linked immunosorbent assay kit and assessment of a Western blot kit performance. Journal of Clinical Microbiology. Published 28 May 2026. doi:10.1128/jcm.00182-26.
Why this paper matters
CPA is a progressive and potentially fatal chronic lung infection that usually occurs in patients with underlying structural lung damage. Diagnosis depends on combining clinical symptoms, characteristic radiology and evidence of Aspergillus infection or immune response.
In practice, Aspergillus serology is often the decisive test. A positive Aspergillus IgG result can support the diagnosis when imaging and symptoms are compatible. A negative result can reduce diagnostic probability. But serology is not absolute. Different assays use different antigen preparations, platforms and reporting units. This means that results from one laboratory may not be directly comparable with results from another.
This paper is therefore important because it addresses a real-world diagnostic problem: how to optimise Aspergillus serological testing so that it performs reliably in the diagnosis of CPA.
Clinical background: why CPA serology is difficult
CPA often develops in patients with structurally abnormal lungs. Common underlying conditions include previous pulmonary tuberculosis, non-tuberculous mycobacterial infection, chronic obstructive pulmonary disease, bronchiectasis, sarcoidosis, prior lung surgery and other cavitary lung diseases.
These same conditions can also cause chronic symptoms and abnormal imaging without CPA. This creates a diagnostic grey zone. Patients may have cavities, pleural thickening, fibrosis, bronchiectasis, chronic cough, haemoptysis or weight loss for reasons other than Aspergillus disease.
Aspergillus IgG testing is therefore valuable because it provides evidence of an immune response to Aspergillus. However, it must be interpreted in context. A positive result does not, by itself, prove active CPA. A negative result does not always fully exclude CPA, particularly if clinical suspicion remains high.
What the study evaluates
The paper evaluates two related aspects of CPA serology:
- Optimisation of an enzyme-linked immunosorbent assay (ELISA) kit for Aspergillus serology in CPA diagnosis.
- Assessment of Western blot kit performance, potentially as a complementary or confirmatory approach.
This is clinically relevant because ELISA-based Aspergillus IgG testing is widely used in diagnostic pathways, while Western blot may offer additional qualitative information in selected cases. The practical question is whether assay optimisation and confirmatory testing improve diagnostic performance enough to change specialist practice.
Why assay cut-offs matter
The choice of diagnostic cut-off is not a technical detail; it changes clinical classification.
| Cut-off strategy | Likely effect | Clinical risk |
|---|---|---|
| Lower cut-off | Higher sensitivity | More false positives and possible overdiagnosis |
| Higher cut-off | Higher specificity | More false negatives and missed CPA |
| Population-specific cut-off | Potentially better clinical performance | May reduce comparability between centres |
| Single universal cut-off | Simpler implementation | May perform poorly across different populations |
In a specialist CPA service, false negatives may delay antifungal treatment and referral. False positives may lead to unnecessary anxiety, additional imaging, prolonged antifungal therapy and avoidable toxicity. The correct balance depends on the clinical setting, disease prevalence and consequences of diagnostic error.
Where Western blot may fit
Western blot testing may be useful where ELISA results are borderline, discordant with imaging, or difficult to interpret in patients with complex lung disease. It may also be useful as a complementary method in diagnostic algorithms, depending on availability and validated performance.
However, Western blot should not be seen as a simple replacement for ELISA. Its value depends on whether it adds diagnostic clarity beyond standard serology, whether it is reproducible between laboratories, and whether clinicians know how to act on the result.
Clinical interpretation: serology is supportive, not standalone
For specialists, the key principle remains:
Aspergillus serology supports the diagnosis of CPA but does not diagnose CPA in isolation.
A robust CPA diagnosis requires integration of:
- compatible symptoms, usually chronic cough, weight loss, fatigue, breathlessness or haemoptysis;
- compatible imaging, particularly cavities, pleural thickening, pericavitary infiltrates, fungal ball, nodules or progressive fibrosis;
- mycological or immunological evidence, especially Aspergillus IgG;
- exclusion or recognition of alternative and co-existing diagnoses, including active tuberculosis, non-tuberculous mycobacterial disease, malignancy and bacterial bronchiectasis.
Implications for specialist services
This paper supports the need for carefully governed CPA serology pathways. Specialist centres and diagnostic laboratories should consider:
- which Aspergillus IgG assay is used locally;
- what cut-off is applied and how it was validated;
- whether borderline zones should be reported rather than simple positive/negative categories;
- how results are interpreted in high-risk structural lung disease populations;
- whether confirmatory testing is available for selected cases;
- how serology is integrated with CT findings and microbiology;
- whether local reports include interpretive comments to reduce misuse.
Suggested diagnostic reporting approach
Rather than reporting Aspergillus serology as a binary answer, laboratories and specialist services may benefit from a more interpretive model:
| Result category | Possible interpretation | Suggested action |
|---|---|---|
| Clearly negative | CPA less likely, but not impossible if clinical suspicion is high | Review imaging and alternative diagnoses; repeat if disease evolves |
| Borderline or low positive | Uncertain significance | Correlate with CT, symptoms, cultures and prior results; consider repeat or confirmatory testing |
| Clearly positive | Supports CPA in the right clinical/radiological context | Assess full CPA criteria and consider specialist referral or treatment discussion |
| Discordant result | Serology conflicts with clinical picture | Reassess diagnosis, assay limitations and possibility of co-existing disease |
Relevance to post-tuberculosis lung disease
This paper is particularly relevant when considered alongside recent evidence that CPA may be detected during or soon after pulmonary tuberculosis treatment. In post-tuberculosis lung disease, cavities and chronic radiological abnormalities are common, but not all symptoms are due to active TB or permanent scarring.
Reliable Aspergillus serology is therefore essential. If the assay cut-off is poorly calibrated, clinicians may either miss CPA in symptomatic patients with cavities or overdiagnose CPA in patients with structural lung damage but no active Aspergillus disease.
Relevance to bronchiectasis and non-tuberculous mycobacterial disease
Patients with bronchiectasis or non-tuberculous mycobacterial lung disease may also have chronic symptoms, mucus production, recurrent infection, radiological change and occasional Aspergillus isolation. Aspergillus serology can be useful in identifying CPA, but positive results must be interpreted carefully because these patients often have complex chronic airway disease.
For this group, assay performance and cut-off choice may substantially affect diagnostic confidence.
Implications for antifungal stewardship
Improved CPA serology has direct stewardship implications. Antifungal treatment for CPA is often prolonged and requires monitoring for toxicity, drug interactions and therapeutic drug levels. Overdiagnosis can expose patients to unnecessary azoles. Underdiagnosis can allow progressive cavitary disease, haemoptysis and loss of lung function.
More reliable serological testing can therefore support both earlier treatment in true CPA and avoidance of unnecessary therapy in patients who do not meet diagnostic criteria.
Evidence strength
| Question | Evidence strength | Comment |
|---|---|---|
| Is Aspergillus IgG central to CPA diagnosis? | Strong | Recognised in major CPA diagnostic guidance |
| Do different assays and cut-offs affect performance? | Strong | Well-recognised practical issue in CPA serology |
| Can assay optimisation improve diagnostic classification? | Likely | This paper directly addresses optimisation, but local validation remains important |
| Should Western blot replace ELISA? | Not established | More likely to be complementary or confirmatory in selected cases |
| Should serology alone determine CPA treatment? | No | Must be interpreted with symptoms, imaging and microbiology |
Practical take-home messages for specialists
- Know which Aspergillus IgG assay your laboratory uses.
- Know the cut-off and whether it has been validated for CPA.
- Be cautious with borderline results.
- Do not diagnose CPA on serology alone.
- Do not dismiss CPA solely because one serological test is negative if the clinical and CT picture is highly suggestive.
- Consider repeat or complementary testing when results are discordant.
- Integrate serology with CT, symptoms, sputum fungal culture/PCR and assessment for tuberculosis or non-tuberculous mycobacteria.
Conclusion
This paper is a timely reminder that CPA diagnosis depends not only on whether Aspergillus serology is performed, but on how well the assay is optimised, how cut-offs are selected and how results are interpreted. For specialist services, improved serology can strengthen diagnostic confidence, support earlier recognition of CPA and reduce unnecessary antifungal treatment.
The broader implication is clear: CPA diagnostic pathways need standardised, validated and clinically interpreted Aspergillus serology, not isolated positive or negative blood test results.
References
- Bigot J, Gibert C, Millet N, et al. Aspergillus serology for chronic pulmonary aspergillosis diagnosis: optimization of an enzyme-linked immunosorbent assay kit and assessment of a Western blot kit performance.
Journal of Clinical Microbiology. Published 28 May 2026.
doi:10.1128/jcm.00182-26.
PubMed - Denning DW, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management.
European Respiratory Journal. 2016;47(1):45-68.
doi:10.1183/13993003.00583-2015.
PubMed - Patterson TF, Thompson GR, Denning DW, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America.
Clinical Infectious Diseases. 2016;63(4):e1-e60.
doi:10.1093/cid/ciw326.
PubMed
Commercial Aspergillus fumigatus real-time PCR for invasive pulmonary aspergillosis: specialist evidence briefing
Why this paper matters
Invasive pulmonary aspergillosis remains difficult to diagnose early, particularly in patients with haematological malignancy, haematopoietic stem cell transplantation, intensive chemotherapy, corticosteroid exposure or profound immunosuppression. Culture is insensitive, histology is often unavailable, and radiology is not specific. Galactomannan has become a central biomarker, but performance varies by specimen type, antifungal exposure, host group and disease stage.
Aspergillus PCR has long been promising, but implementation has been limited by assay heterogeneity, extraction differences, target selection, contamination concerns, and variable interpretation across centres. A clinically evaluated commercial real-time PCR assay is therefore important because commercialisation may improve standardisation, reproducibility and adoption outside specialist mycology laboratories.
Clinical context
The diagnosis of IPA is usually probabilistic. Clinicians combine:
- host factors, such as neutropenia, haematological malignancy, transplantation or corticosteroid exposure;
- compatible imaging, especially nodules, halo sign, cavitation or infarct-like lesions on computed tomography;
- mycological evidence, including galactomannan, culture, microscopy, PCR or lateral-flow assays;
- clinical course and response to antifungal therapy.
In this setting, a commercial Aspergillus fumigatus real-time PCR assay could support earlier diagnosis, improve confidence in probable IPA classification, and potentially reduce unnecessary empirical antifungal treatment when used as part of a diagnostic algorithm.
Main finding
The paper evaluates a commercial Aspergillus fumigatus real-time PCR assay for the diagnosis of invasive pulmonary aspergillosis in patients with haematological malignancies. The clinical relevance lies in validating a defined assay in a high-risk population where early diagnosis directly affects antifungal timing and survival.
The specialist significance is not simply that PCR “works”. The key question is whether a commercial PCR assay offers sufficiently reliable analytical and clinical performance to be used alongside galactomannan and imaging in routine pathways.
What is genuinely new?
The novelty is likely to sit in one or more of the following areas:
- evaluation of a specific commercial assay rather than an in-house laboratory-developed test;
- clinical validation in a defined haematology population;
- comparison against established diagnostic categories such as proven/probable IPA;
- assessment of analytical performance, including limit of detection, reproducibility or specificity;
- potential contribution to standardisation of Aspergillus PCR implementation.
This is not a new concept in principle: Aspergillus PCR has been studied for many years. What is more clinically useful is the transition from heterogeneous in-house assays towards assays that can be validated, quality-assured and compared across centres.
Relationship to existing evidence
Recent reviews of molecular fungal diagnostics emphasise that PCR can improve the diagnosis of invasive fungal disease but remains limited by standardisation, assay availability and interpretation. A 2025 review in Diagnostics noted that PCR is sensitive and specific for invasive fungal disease, but that implementation remains constrained by limited standardisation, few commercial options, and lack of clear guidance for interpreting results.
That surrounding evidence makes this type of paper important. Commercial PCR assays do not automatically solve diagnostic uncertainty, but they can reduce one major barrier: between-laboratory variability.
Strengths to look for in the paper
- Clearly defined patient population, especially haematological malignancy or transplant subgroups.
- Use of accepted case definitions for proven, probable and possible IPA.
- Separate analytical and clinical performance assessment.
- Comparison with galactomannan, culture and radiology.
- Evaluation by specimen type, especially bronchoalveolar lavage fluid versus blood.
- Consideration of antifungal exposure before sampling.
- Reporting of sensitivity, specificity, positive predictive value and negative predictive value.
Limitations and cautions
PCR performance depends strongly on specimen type. Bronchoalveolar lavage fluid generally provides a higher organism burden than blood in IPA, but it is more invasive and may not be feasible in unstable or thrombocytopenic patients. Blood PCR is less invasive but may be less sensitive, especially in localised airway-invasive disease.
False positives may arise from colonisation, contamination or detection of non-invasive airway presence. False negatives may occur with low fungal burden, prior antifungal therapy, sampling timing, extraction inefficiency or inhibitors. A positive PCR result should therefore not be interpreted in isolation.
A further issue is species coverage. A narrowly targeted Aspergillus fumigatus assay may perform well for A. fumigatus but could miss non-fumigatus Aspergillus species or cryptic species with different susceptibility patterns. In haematology patients, that may matter for epidemiology and antifungal resistance surveillance.
Clinical implications
For specialist services, the likely implication is that commercial Aspergillus PCR should be considered as part of a multi-modal diagnostic pathway rather than as a standalone rule-in or rule-out test.
A practical diagnostic model might include:
- early CT imaging in high-risk patients with persistent fever or respiratory symptoms;
- serum galactomannan in appropriate host groups;
- bronchoalveolar lavage where clinically safe;
- BAL galactomannan, fungal culture, microscopy and Aspergillus PCR;
- azole resistance testing or sequencing where Aspergillus is detected;
- multidisciplinary interpretation with haematology, infectious diseases, respiratory and mycology input.
Implications for antifungal stewardship
A validated commercial PCR assay may support earlier targeted antifungal therapy, but also more confident de-escalation when combined with negative biomarkers and low radiological probability. The stewardship value depends on pathway design. PCR added without interpretive governance may increase diagnostic noise; PCR embedded into a structured algorithm may reduce unnecessary empirical therapy and improve diagnostic confidence.
Implications for UK specialist mycology services
For UK centres, this type of paper supports the case for:
- standardised fungal PCR pathways;
- clear reporting language for positive and negative results;
- integration with antifungal stewardship rounds;
- external quality assessment participation;
- reflex testing for resistance where feasible;
- collaboration between local laboratories and specialist mycology reference services.
Evidence strength
| Question | Evidence strength | Comment |
|---|---|---|
| Can Aspergillus PCR detect fungal DNA in clinical specimens? | Strong | Longstanding molecular evidence |
| Can PCR support IPA diagnosis? | Moderate to strong | Best when combined with host, imaging and biomarker data |
| Are commercial assays ready for routine use? | Emerging | Depends on assay validation, specimen type and pathway integration |
| Can PCR alone rule in or rule out IPA? | No | Should not be used in isolation |
Conclusion
Commercial Aspergillus real-time PCR assays represent an important step towards standardised molecular diagnosis of invasive pulmonary aspergillosis. Their greatest value is likely to be in high-risk haematology pathways, especially when applied to bronchoalveolar lavage fluid and interpreted alongside galactomannan, culture, imaging and host risk.
The clinical message is not that PCR replaces existing tests. Rather, validated commercial PCR may strengthen diagnostic algorithms, improve early case recognition, support antifungal stewardship and reduce variation between laboratories.
References
- Gibert C, Bigot J, et al. Clinical and analytical evaluation of a commercial Aspergillus fumigatus real-time PCR assay for the diagnosis of invasive pulmonary aspergillosis in patients with hematological malignancies.
Journal details to confirm from PubMed record.
PubMed - Brown L, Cruciani M, Morton O, et al. The molecular diagnosis of invasive fungal diseases with a focus on PCR.
Diagnostics. 2025;15(15):1909.
doi:10.3390/diagnostics15151909.
PubMed - Patterson TF, Thompson GR, Denning DW, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America.
Clinical Infectious Diseases. 2016;63(4):e1-e60.
doi:10.1093/cid/ciw326.
PubMed
Research significance summary for specialists: Chronic pulmonary aspergillosis during tuberculosis treatment: emerging evidence, diagnostic pitfalls and implications for TB pathways
Why this matters
CPA remains substantially under-recognised in people with current or previous pulmonary tuberculosis. The clinical overlap is considerable: cough, haemoptysis, weight loss, fatigue, cavitation and progressive radiological change can be attributed to TB relapse, treatment failure, non-tuberculous mycobacterial infection, bacterial bronchiectasis, malignancy or post-TB lung disease.
For TB programmes and respiratory services, the practical question is no longer simply whether CPA occurs after TB. The question is whether there should be defined triggers for CPA assessment during TB treatment, particularly when symptoms persist despite microbiologically effective therapy.
The traditional model: CPA after tuberculosis
The conventional model is well established:
- Pulmonary tuberculosis causes cavitation, fibrosis, bronchiectasis and pleural distortion.
- Residual cavities may persist after microbiological cure.
- Aspergillus conidia can colonise these abnormal airspaces.
- In some patients, colonisation progresses to simple aspergilloma, chronic cavitary pulmonary aspergillosis or chronic fibrosing pulmonary aspergillosis.
This model is supported by older post-TB aspergilloma studies and by modern CPA burden estimates. Bongomin’s review of post-tuberculosis CPA highlights residual pulmonary cavities as a major risk substrate and summarises classic British data in which Aspergillus precipitins and aspergillomas increased over time after treated pulmonary TB.
The newer question: can CPA be present or emerge during TB treatment?
Several recent prospective studies suggest that CPA may be detected during the active TB treatment pathway, not only years after treatment completion.
1. Jha et al. 2024: serial CPA assessment during treatment of newly diagnosed PTB
Jha and colleagues conducted a prospective study of newly detected pulmonary tuberculosis cases and assessed CPA at baseline and at the end of anti-tubercular therapy. Of 255 initially recruited patients, 158 completed follow-up. The authors reported CPA at baseline and at end-of-treatment, with 23 of 158 assessed patients diagnosed with CPA at completion of TB therapy.
The study is important because it examined serial Aspergillus IgG changes and CPA incidence during the course of anti-tubercular therapy. The authors reported proven CPA in approximately 7% at baseline and 14.6% at end-of-treatment, broadly comparable with earlier Indonesian longitudinal data.
However, interpretation requires caution. Not all patients underwent HRCT at end-of-treatment, follow-up attrition was substantial, and the distinction between incident CPA, pre-existing CPA, transient Aspergillus immune response and radiological overlap with active TB remains difficult.
2. APICAL Indonesia study: CPA in patients treated for pulmonary TB
The APICAL study by Setianingrum and colleagues was a prospective longitudinal study in Indonesia. It investigated CPA in patients treated for pulmonary tuberculosis and reported CPA at baseline and at the end of TB therapy. Jha et al. cite APICAL as reporting 7.9% CPA at baseline and 13.3% at the end of TB therapy when proven and probable CPA were combined.
This study is one of the key pieces of evidence that the TB–CPA relationship is not purely post-treatment. CPA may be present within the treatment period, particularly where patients have cavitary disease or persistent symptoms.
3. Uganda study: persistent symptoms after two months of TB therapy
Namusobya and colleagues studied patients with microbiologically confirmed drug-sensitive PTB who had persistent respiratory symptoms after two months of standard anti-TB therapy. CPA was defined using persistent symptoms, suggestive radiology and evidence of Aspergillus infection, including Aspergillus IgG/IgM immunochromatographic testing and/or culture.
The study found CPA in around 20% of participants with persistent symptoms after the intensive phase of TB treatment. This is particularly relevant to clinical practice because two months is a natural review point in TB treatment pathways. Persistent symptoms at that stage are often interpreted as delayed recovery, adherence problems, drug resistance or alternative bacterial infection. CPA should be added to that differential in selected patients.
4. Ghana prospective follow-up: mainly post-treatment, but relevant to timing
Ocansey and colleagues followed patients after pulmonary TB treatment and found CPA emerging by the end of treatment and increasing further six months later. The study reported an overall 12-month CPA incidence of 10.7% among resurveyed patients, with 3% at end-of-treatment and 7.4% six months post-treatment.
This supports a continuum model: CPA risk may begin during active disease or treatment and continue after TB completion, especially in those with residual cavities.
Possible biological and diagnostic explanations
Detection of CPA during TB therapy may reflect more than one phenomenon. These categories are clinically important because they have different implications.
| Scenario | Interpretation | Clinical implication |
|---|---|---|
| Pre-existing CPA misdiagnosed as TB | CPA may mimic smear-negative or clinically diagnosed TB | Review microbiological confirmation and imaging; avoid repeated empiric TB treatment where evidence is weak |
| True PTB–CPA co-disease at diagnosis | Both Mycobacterium tuberculosis and Aspergillus-related disease are present | Requires parallel diagnostic reasoning and careful drug interaction management |
| Incident CPA during treatment | Aspergillus disease develops in newly formed or persistent cavities | Consider CPA if symptoms persist or imaging progresses despite adequate TB treatment |
| Colonisation or transient serological positivity | Aspergillus detected without established progressive CPA | Repeat assessment and avoid over-treatment unless full CPA criteria are met |
| Post-TB lung disease with later CPA | Classic pathway: CPA develops months to years after TB treatment | Long-term awareness in patients with residual cavities, haemoptysis or chronic symptoms |
Diagnostic criteria: why timing is difficult
Most CPA definitions require compatible symptoms, radiology and mycological or immunological evidence over at least three months. That creates difficulty during TB therapy because active PTB itself can produce prolonged symptoms and cavitary radiology.
Guideline-consistent CPA diagnosis generally requires:
- chronic respiratory or systemic symptoms, usually for at least three months;
- compatible imaging, such as one or more cavities, pleural thickening, pericavitary infiltrates, fungal ball, progressive fibrosis or nodules;
- microbiological or immunological evidence of Aspergillus infection, especially raised Aspergillus IgG;
- exclusion of alternative diagnoses, including active TB, non-tuberculous mycobacterial disease, malignancy and other chronic infections.
In active TB, the exclusion criterion is problematic because TB and CPA can genuinely co-exist. Therefore, rather than using “active TB” to exclude CPA automatically, clinicians may need to ask whether the observed course is fully explained by TB alone.
When should CPA be considered during TB treatment?
CPA assessment should be considered during TB treatment when one or more of the following are present:
- persistent cough, haemoptysis, weight loss, fatigue or breathlessness after the intensive phase of TB treatment;
- persistent or enlarging cavities despite microbiological response to anti-TB therapy;
- new intracavitary material or suspected fungal ball;
- pleural thickening or pericavitary infiltrates that progress despite TB treatment;
- repeatedly negative TB microbiology despite a clinical label of TB relapse;
- history of previous TB or other structural lung disease;
- unexplained haemoptysis after apparent TB response;
- patients being considered for repeat TB treatment without strong microbiological confirmation.
Suggested diagnostic approach
A pragmatic diagnostic approach in specialist respiratory or infectious disease settings could include:
- Confirm TB status: review baseline microbiology, GeneXpert/NAAT, culture, drug susceptibility and treatment response.
- Repeat imaging: CT is preferable to chest radiography where CPA is suspected, particularly to assess cavities, fungal ball, pleural thickening and pericavitary progression.
- Request Aspergillus IgG: a positive result is a major diagnostic component, though not sufficient alone.
- Send respiratory samples: fungal culture and/or Aspergillus PCR where available; also reassess for TB and non-tuberculous mycobacteria.
- Assess duration and trajectory: progressive symptoms or radiology over three months strengthens CPA diagnosis.
- Review differential diagnoses: malignancy, bacterial bronchiectasis, NTM, lung abscess, vasculitis and other chronic infections.
- Discuss complex cases with a specialist mycology or CPA centre: especially if antifungal therapy is being considered during rifampicin-based TB treatment.
Treatment implications and drug interactions
If CPA is diagnosed during TB therapy, management is complicated by major drug interactions. Rifampicin is a potent enzyme inducer and substantially reduces exposure to many triazole antifungals, including itraconazole, voriconazole and posaconazole. Co-administration is generally problematic and may render azole therapy ineffective.
Specialist input is therefore essential. Management may require:
- review of TB regimen and treatment phase;
- therapeutic drug monitoring for azoles where used;
- careful liver function monitoring;
- assessment of haemoptysis risk;
- consideration of timing of antifungal initiation;
- multidisciplinary discussion involving TB, respiratory, infectious diseases, pharmacy and mycology teams.
In some cases, observation and reassessment may be appropriate if CPA criteria are incomplete and the patient is clinically improving. In others, particularly with progressive cavitary disease, haemoptysis or strong Aspergillus IgG positivity, earlier specialist intervention may be justified.
What do guidelines currently say?
ERS/ESCMID
The ERS/ESCMID CPA guideline recognises tuberculosis as a major underlying condition for CPA and defines CPA using chronic symptoms, compatible radiology and Aspergillus evidence, typically over at least three months. It supports Aspergillus IgG as a central diagnostic test and recommends long-term oral triazole therapy for symptomatic or progressive chronic cavitary disease.
IDSA
The IDSA aspergillosis guideline similarly defines chronic cavitary pulmonary aspergillosis by at least three months of symptoms or progressive radiographic abnormalities, compatible cavitary disease, microbiological or serological evidence of Aspergillus, and minimal immunocompromise. It explicitly notes that CPA may complicate underlying pulmonary diseases, including tuberculosis and non-tuberculous mycobacterial infection.
BTS
The British Thoracic Society 2025 Clinical Statement on Aspergillus-related chronic lung disease provides current UK best-practice framing for diagnosis and management of chronic Aspergillus lung disease. Its publication reflects increasing recognition that Aspergillus-related chronic lung disease requires specific diagnostic pathways, antifungal stewardship and specialist respiratory-mycology collaboration.
WHO TB guidance
WHO TB guidance focuses on TB diagnosis, drug susceptibility, treatment regimens, monitoring, treatment failure and public health control. CPA is not yet embedded as a routine screening component of standard TB treatment pathways. This creates a gap between TB programme algorithms and emerging evidence from fungal disease studies.
Evidence strength
| Question | Evidence strength | Comment |
|---|---|---|
| Does TB predispose to CPA? | Strong | Consistent epidemiological, radiological and mechanistic evidence |
| Does CPA occur after TB treatment? | Strong | Well-established, especially with residual cavities |
| Can CPA be detected during TB treatment? | Moderate | Supported by prospective studies from Indonesia, Uganda and India |
| Does CPA truly begin during treatment rather than being pre-existing? | Uncertain | Requires better baseline CT, serial mycology and longer follow-up |
| Should all TB patients be screened for CPA? | Insufficient evidence | Targeted testing in high-risk or persistently symptomatic patients is more defensible |
| Does early CPA detection during TB treatment improve outcomes? | Unproven | Needs prospective interventional studies |
Implications for TB and respiratory services
The emerging evidence supports a targeted CPA assessment trigger within TB pathways, rather than universal screening at present.
A reasonable specialist position would be:
In patients receiving treatment for pulmonary tuberculosis, persistent symptoms, haemoptysis or non-resolving/progressive cavitary disease after the intensive phase should prompt consideration of CPA, especially where TB microbiology is negative or improving and imaging remains suspicious.
This is particularly relevant in high TB burden countries, but also in low TB burden settings where patients with previous TB, migrant health histories or unexplained cavitary disease may be seen in respiratory clinics.
Research priorities
- Prospective studies with baseline and serial CT imaging in microbiologically confirmed PTB.
- Serial Aspergillus IgG titres, fungal culture and molecular testing during TB therapy.
- Clear separation of proven CPA, probable CPA, Aspergillus colonisation and transient seropositivity.
- Studies of CPA screening at two months versus end-of-treatment versus six months post-treatment.
- Outcome studies assessing whether early CPA recognition reduces haemoptysis, lung destruction, retreatment for TB or mortality.
- Health-economic modelling of targeted CPA testing in TB programmes.
Conclusion
The evidence base is moving from a simple post-TB model towards a continuum model of TB-associated CPA. In this model, Aspergillus-related disease may be present at TB diagnosis, emerge during therapy, become apparent at treatment completion, or develop later in post-TB lung disease.
For specialists, the key implication is not that every patient with TB requires CPA screening. Rather, CPA should be actively considered when the clinical trajectory is not adequately explained by TB alone, particularly in patients with cavitation, haemoptysis, persistent symptoms or poor radiological resolution.
Embedding a CPA assessment trigger into TB follow-up pathways may reduce misdiagnosis, repeated empirical TB treatment and delayed antifungal management. The evidence is not yet definitive, but it is strong enough to justify specialist awareness, targeted testing and further prospective research.
References
-
Bongomin F. Post-tuberculosis chronic pulmonary aspergillosis: An emerging public health concern.
PLOS Pathogens. 2020;16(8):e1008742.
doi:10.1371/journal.ppat.1008742.
PubMed -
Denning DW, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management.
European Respiratory Journal. 2016;47(1):45-68.
doi:10.1183/13993003.00583-2015.
PubMed -
Jha D, Kumar U, Meena VP, et al. Chronic pulmonary aspergillosis incidence in newly detected pulmonary tuberculosis cases during follow-up.
Mycoses. 2024;67(5).
doi:10.1111/myc.13747.
PubMed -
Namusobya M, Bongomin F, Mukisa J, et al. Chronic pulmonary aspergillosis in patients with active pulmonary tuberculosis with persisting symptoms in Uganda.
Mycoses. 2022;65(6):625-634.
doi:10.1111/myc.13444.
PubMed -
Ocansey B, Otoo B, Gbadamosi H, et al. Importance of Aspergillus-specific antibody screening for diagnosis of chronic pulmonary aspergillosis after tuberculosis treatment: a prospective follow-up study in Ghana.
Journal of Fungi. 2022;9(1):26.
doi:10.3390/jof9010026.
PubMed -
Patterson TF, Thompson GR, Denning DW, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America.
Clinical Infectious Diseases. 2016;63(4):e1-e60.
doi:10.1093/cid/ciw326.
PubMed -
Setianingrum F, Rozaliyani A, Adawiyah R, et al. A prospective longitudinal study of chronic pulmonary aspergillosis in pulmonary tuberculosis in Indonesia (APICAL).
Thorax. 2022;77(8):821-828.
doi:10.1136/thoraxjnl-2020-216464.
PubMed