
Trying a New Diet? A Guide for People with Aspergillosis

Originally published: August 2018
Last reviewed: July 2026
If you have searched online for “the best diet for aspergillosis”, you may have found advice ranging from sensible healthy eating to highly restrictive diets claiming to treat fungal infections. It can be difficult to know what to believe.
This guide explains what diet can and cannot do, how to recognise marketing claims, and how to try dietary changes safely if you decide to do so.
A note from the National Aspergillosis Centre
People often ask whether changing their diet can help control aspergillosis. It is a sensible question, and many patients find that healthier eating improves their overall wellbeing. However, current research has not identified any specific diet that treats aspergillosis itself.
This guide is designed to help you separate evidence-based advice from common myths and make informed choices alongside your usual medical care.
Key points
- There is no proven “anti-fungal diet” that treats aspergillosis.
- A healthy, balanced diet can support general health, energy levels and recovery from illness.
- Dietary changes should not replace antifungal medicines, inhalers, steroids or other prescribed treatments.
- Be cautious of diets, supplements or programmes that promise cures.
- Marketing phrases such as “immune boosting”, “natural antifungal” or “clinically proven” do not always mean strong evidence.
- If you try a new diet, make one change at a time and monitor whether it genuinely helps.
- Speak to your healthcare team before making major dietary changes, especially if you have diabetes, kidney disease, weight loss or are taking antifungal medication.
Why do people with aspergillosis look at diet?
Living with aspergillosis can be frustrating and exhausting. People may experience breathlessness, fatigue, weight changes, repeated flare-ups, steroid side effects or uncertainty about the future. It is understandable to look for things you can control yourself.
Diet is one of the most common areas people explore. Some dietary changes may be helpful for general health, but many claims online go much further than the evidence supports.
Over the years, patients have asked about anti-fungal diets, Candida diets, sugar-free diets, ketogenic diets, low-carbohydrate diets, gluten-free diets, dairy-free diets, alkaline diets, detox programmes and supplement regimens. Some of these approaches may be appropriate for specific medical reasons, but none has been shown to treat aspergillosis itself.
So how can you separate reliable advice from persuasive marketing?
Recognising marketing claims
Many websites, social media posts and advertisements use scientific-sounding language to make products appear more effective than the evidence supports. This does not necessarily mean the product is ineffective, but it does mean you should look carefully for independent evidence rather than relying on marketing claims.
Be particularly cautious if you see terms such as:
- “clinically proven”
- “doctor recommended”
- “immune boosting”
- “natural antifungal”
- “detoxifies the body”
- “supports immunity”
- “research backed”
- “breakthrough formula”
- “ancient remedy”
- “pharmaceutical grade”
- “exclusive blend”
- “used by leading experts”
These phrases are commonly used in advertising but do not necessarily indicate strong clinical evidence. In some cases, the supporting research may involve only laboratory studies, animal research, very small human studies, or research funded by the manufacturer. Such studies can provide useful early information but are rarely enough on their own to show that a product benefits people with aspergillosis.
Similarly, remember that “natural” does not automatically mean safe, and “evidence based” does not necessarily mean there is good-quality evidence that a product works for people with aspergillosis. Even products described as “clinically tested” may only have been evaluated in a small number of people or for conditions unrelated to aspergillosis.
If a supplement or diet genuinely provides a meaningful health benefit, you should usually be able to find independent recommendations from organisations such as the NHS, registered dietitians, recognised medical societies or high-quality systematic reviews — not just testimonials, celebrity endorsements or promotional websites.
It is perfectly reasonable to ask whether a particular diet, supplement or health product might help. Your healthcare team can help you interpret the available evidence and identify any potential interactions with your medication before you spend money or make major changes.
A simple rule of thumb is to follow the evidence, not the marketing.
So what does the evidence actually tell us?
What does the evidence say?
Nutrition is important for everyone living with a chronic illness. A good diet can support general health, but current research has not identified any diet that treats aspergillosis itself.
What diet can help with
A healthy eating pattern may help you:
- maintain strength and muscle mass
- recover from illness
- manage weight
- support bone health
- control blood sugar
- reduce cardiovascular risk
- improve general wellbeing
This can be especially important for people living with long-term lung disease, chronic infection, steroid treatment or reduced physical activity.
What diet cannot do
Diet cannot:
- kill Aspergillus growing in the lungs
- cure chronic pulmonary aspergillosis
- cure allergic bronchopulmonary aspergillosis
- replace antifungal treatment
- replace specialist respiratory care
If someone claims that a diet can cure aspergillosis, it is reasonable to ask whether this has been tested in properly conducted clinical studies. At present, there is no good evidence that any specific diet cures aspergillosis.
How to judge a new diet
Before trying a diet you have found online, ask:
- Does it promise a cure?
- Does it claim to “starve” fungus from the body?
- Does it recommend stopping prescribed medicines?
- Does it require expensive supplements, tests or coaching?
- Does it remove whole food groups without a clear medical reason?
- Is it based mainly on personal stories rather than research?
- Is it supported by recognised healthcare organisations?
The more warning signs you see, the more cautious you should be.
If you decide to try a new diet
1. Be clear about your goal
Decide what you are trying to improve. For example:
- energy levels
- weight
- blood sugar
- digestion
- reflux
- general fitness
A clear goal makes it easier to judge whether the change is helping.
2. Change one thing at a time
If you change several things at once, it becomes difficult to know what made a difference. Try one change for a few weeks before adding another.
3. Keep a simple diary
You may want to record:
- what you changed
- symptoms
- energy levels
- weight
- blood sugar, if relevant
- exercise tolerance
- side effects
4. Do not stop prescribed treatment
Dietary changes should complement your medical care, not replace it. Do not stop antifungal medication, steroids, inhalers or other prescribed treatments without medical advice.
5. Review honestly
If a change has not helped after a reasonable trial, it may not be worth continuing. A diet should improve your life, not make it more stressful, expensive or restrictive.
Healthy eating in practice
For most people, the best starting point is not an extreme diet but a balanced eating pattern that can be maintained long term.
This usually means:
- plenty of vegetables and fruit
- whole grains where tolerated
- beans, pulses, nuts and seeds
- adequate protein
- fish, lean meat, eggs or suitable alternatives
- healthy fats such as olive oil
- enough fluid
- limiting highly processed foods and sugary drinks
A Mediterranean-style diet is often recommended for general health because it supports heart health and provides a wide range of nutrients. However, the best diet for an individual also depends on their medical conditions, preferences, culture, budget and ability to prepare food.
Special situations
If you take corticosteroids
Many people with ABPA or severe asthma take corticosteroids such as prednisolone. These medicines can be very useful, but they may also increase the risk of:
- weight gain
- raised blood sugar
- diabetes
- bone thinning
- muscle loss
If you take steroids regularly, it is worth paying attention to:
- adequate protein
- calcium intake
- vitamin D, if advised
- blood sugar control
- gradual weight management
- strength-building activity where possible
If you take antifungal medicines
Some antifungal medicines can interact with other medicines, supplements, herbal products and certain foods. Always tell your healthcare team about any supplements or alternative products you are taking or planning to take.
This includes:
- herbal remedies
- vitamin and mineral supplements
- protein powders
- weight-loss products
- traditional medicines
- detox products
“Natural” does not always mean safe. Some products can affect liver function or alter medicine levels.
If you have diabetes or steroid-induced high blood sugar
People with diabetes, or those who develop raised blood sugar while taking steroids, may need more specific dietary advice. Reducing excess sugar and refined carbohydrates may help blood sugar control, but very restrictive diets should be discussed with a healthcare professional.
If you monitor your blood sugar, it can be useful to record any dietary changes alongside your readings. This can help you and your healthcare team see what is actually making a difference.
Common questions
What about sugar?
A common claim is that sugar “feeds” Aspergillus in the lungs. This is an oversimplification.
Reducing excess sugar is sensible for general health, particularly if you have diabetes or take steroids. However, there is no evidence that eliminating sugar cures aspergillosis.
Should I avoid mouldy foods?
You should avoid obviously mouldy food, as anyone should. Mouldy food can contain harmful substances and may not be safe to eat.
This does not mean that everyone with aspergillosis needs to follow an extreme mould-free diet. If you are unsure about food safety, ask your healthcare team or a registered dietitian.
Do probiotics help?
There is growing interest in the gut microbiome. Probiotics may help some digestive problems, but there is currently little evidence that they directly improve aspergillosis.
For most people, a varied diet containing fibre-rich foods is a better long-term foundation for gut health than relying only on supplements.
Be cautious with miracle diets
Be especially careful with diets or programmes that promise to:
- cure fungal infection
- detox the body
- starve Aspergillus
- replace medication
- rapidly reset the immune system
These claims are rarely supported by good evidence. Very restrictive diets can also lead to weight loss, poor nutrition, social isolation and unnecessary anxiety around food.
When should I ask for professional advice?
Ask your GP, specialist team or a registered dietitian for advice if you:
- are losing weight without trying
- are struggling to eat enough
- feel breathless while eating
- have diabetes or steroid-induced high blood sugar
- have kidney disease
- are considering a very restrictive diet
- are using supplements alongside antifungal medicines
- have concerns about malnutrition
When should I seek urgent medical help?
Seek urgent medical advice if you develop:
- rapid unexplained weight loss
- persistent vomiting
- difficulty swallowing
- signs of dehydration
- confusion or severe weakness
- large amounts of coughing up blood
Summary
Living with aspergillosis often means making decisions about treatments, lifestyle and nutrition. While there is no diet that has been proven to treat aspergillosis, healthy eating can play an important role in maintaining strength, supporting recovery and improving overall wellbeing.
If you decide to make dietary changes, do so gradually, keep an open mind, and discuss major changes with your healthcare team. Be especially cautious of diets, supplements or programmes that promise more than the evidence can support.
The best dietary advice is usually the simplest: follow the evidence, not the marketing.
Further reading
Related articles on Aspergillosis.org
- Diet and Weight Management
- Living Well with Aspergillosis
- Exercise and Fatigue
- Prednisolone and Weight Gain
- Steroid-Induced Diabetes
- Living with ABPA
- Living with Chronic Pulmonary Aspergillosis (CPA)
- Antifungal Medicines
- Antifungal Drug Interactions
- Bone Health and Steroid Treatment
- Frequently Asked Questions
External evidence-based resources
- NHS: The Eatwell Guide
- British Dietetic Association: Food Facts
- British Dietetic Association: Healthy Eating Resources
- Asthma + Lung UK: Living Well with a Lung Condition
- NHS: Vitamins and Minerals
- NHS: Healthy Weight
- NHS: Type 2 Diabetes, Food and Keeping Active
- British Nutrition Foundation
Further reading for healthcare professionals
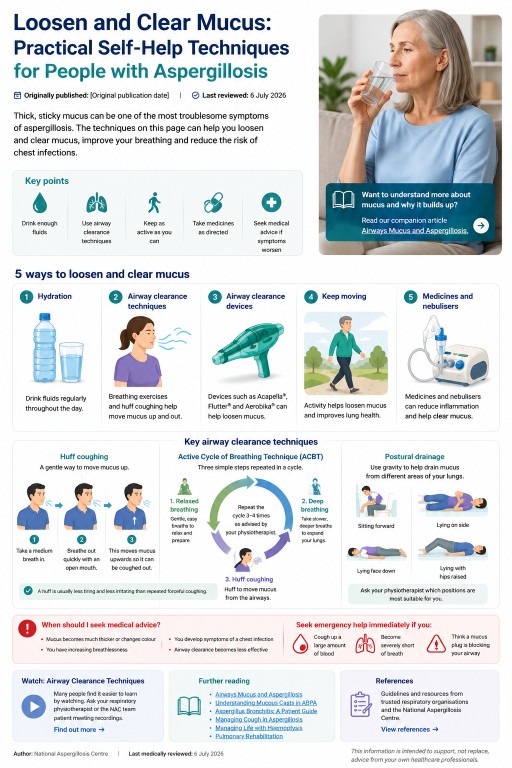
Loosen and Clear Mucus: Practical Self-Help Techniques for People with Aspergillosis
Originally published: 16 August 2018
Last reviewed: 6 July 2026
Many people living with aspergillosis find that thick, sticky mucus is one of their most frustrating symptoms. It can be difficult to cough up, make breathing harder, disturb sleep and sometimes contribute to repeated chest infections.
This guide explains practical ways to loosen and clear mucus safely. Everyone is different, so you may find that combining several approaches works better than relying on just one.
Key points
- Drink enough fluids to help keep mucus from becoming too thick.
- Use airway clearance techniques recommended by your respiratory physiotherapist.
- Keep as active as your health allows.
- Take prescribed medicines exactly as directed.
- Use gentle techniques if you are prone to coughing up blood.
- Seek urgent medical help if you cough up a large amount of blood, become severely breathless, or think a mucus plug is blocking your airway.
Why does aspergillosis cause thick mucus?
Healthy mucus protects the lungs by trapping dust, bacteria and fungal spores before they are removed by tiny hair-like structures called cilia.
In people with aspergillosis, asthma, bronchiectasis or chronic airway inflammation, mucus can become thicker and stickier. It can then build up in the airways and become harder to clear.
This may lead to:
- persistent coughing
- breathlessness
- wheezing
- chest discomfort
- recurrent chest infections
- mucus plugs that block part of the airway
For more background, read our companion article: Airways Mucus and Aspergillosis.
1. Keep well hydrated
Drinking enough fluid helps prevent mucus from becoming even thicker. Water will not dissolve mucus, but good hydration can make mucus less sticky and easier to clear.
Top tip: sip drinks regularly throughout the day rather than waiting until you feel thirsty.
Warm drinks may also feel soothing, and some people find they temporarily make mucus easier to cough up.
2. Practise airway clearance techniques
Respiratory physiotherapists teach breathing exercises designed to move mucus from the smaller airways into the larger airways, where it can be coughed out more easily.
Active Cycle of Breathing Technique (ACBT)
Active Cycle of Breathing Technique, often called ACBT, combines three stages:
- gentle relaxed breathing
- deep breathing exercises
- huff coughing
Many people with bronchiectasis, ABPA and Aspergillus bronchitis find that practising ACBT regularly makes mucus easier to clear.
Huff coughing
A huff is usually gentler and more effective than repeated forceful coughing.
Take a medium-sized breath, then breathe out quickly through an open mouth, as though steaming up a mirror. This helps move mucus upwards while placing less strain on your airways.
Remember: gentle, regular airway clearance is usually more effective than repeated forceful coughing, which can leave you exhausted and irritate your airways.
Postural drainage
Changing your position can allow gravity to help drain mucus from different parts of the lungs. Your respiratory physiotherapist can advise which positions are suitable for you.
Postural drainage may not be appropriate for everyone, especially if you have reflux, heart disease, severe breathlessness or a history of significant haemoptysis.
3. Consider airway clearance devices
Some people benefit from handheld devices that create gentle vibration or resistance while breathing out.
Examples include:
- Acapella®
- Flutter®
- Aerobika®
These devices are commonly used in bronchiectasis care and may help loosen mucus. Ask your respiratory physiotherapist whether one would be suitable for you.
If you have recently coughed up blood, check with your healthcare team before using airway clearance devices, especially devices that create pressure or vibration in the airways.
4. Keep moving
Physical activity is one of the simplest ways to help loosen mucus.
Depending on your health, this may include:
- walking
- gentle cycling
- pulmonary rehabilitation
- light strength exercises
- stretching and breathing exercises
Even a short walk can stimulate coughing and help move mucus towards the larger airways.
5. Medicines and nebulisers
Your healthcare team may prescribe treatments to improve mucus clearance or treat the underlying cause of excess mucus.
These may include:
- inhalers
- antifungal medicines
- antibiotics
- nebulised saline
- mucolytic medicines
- other treatments recommended by your respiratory team
Nebulised treatments should only be used as prescribed. Some can temporarily worsen wheezing or chest tightness in certain people.
Never start, stop or change medication without discussing it with your healthcare team.
Haemoptysis: what if I cough up blood?
Some people with aspergillosis, particularly those with bronchiectasis or chronic pulmonary aspergillosis (CPA), may occasionally cough up blood. This is called haemoptysis.
Haemoptysis can range from a few small streaks of blood in the sputum to larger amounts that need urgent medical attention.
If you notice a small amount of blood, try to remain calm and avoid repeated forceful coughing, which may irritate the airways further. Gentle techniques such as relaxed breathing and huff coughing may be more appropriate until you have spoken to your healthcare team.
Contact your respiratory team or GP for advice, especially if the bleeding is new, becoming more frequent or accompanied by worsening symptoms.
Seek emergency medical help immediately if:
- you cough up a large amount of blood
- the bleeding continues
- you become increasingly breathless
- you feel faint, weak or very unwell
- you think a mucus plug is stopping you from breathing normally
If your specialist team has given you a personalised haemoptysis action plan, follow that advice.
If you have experienced haemoptysis before, ask your respiratory physiotherapist or respiratory specialist for personalised guidance about airway clearance during and after an episode. They can advise when it is safe to restart techniques such as ACBT, huff coughing or airway clearance devices.
For more information, see:
When should I seek medical advice?
Contact your healthcare team if:
- your mucus suddenly becomes much thicker than usual
- your mucus changes colour and you feel more unwell
- you become increasingly breathless
- you develop fever or symptoms of a chest infection
- your usual airway clearance techniques are becoming less effective
- you start coughing up blood, even in small amounts
Frequently asked questions
Should I keep coughing until all the mucus has gone?
No. Repeated forceful coughing can be exhausting and may irritate your airways. Controlled airway clearance techniques are usually more effective.
Does drinking water dissolve mucus?
No. Water does not dissolve mucus, but good hydration can make mucus less sticky and easier to clear.
Are steam inhalations helpful?
Some people find warm steam soothing, although there is limited evidence that it improves mucus clearance. Avoid very hot steam because of the risk of burns.
Can exercise help clear mucus?
Yes. Many people find that movement helps loosen mucus and makes coughing more productive. Choose activity that is appropriate for your health and pace yourself.
Should I use an airway clearance device?
Some people benefit from devices such as Acapella®, Flutter® or Aerobika®, but they are not suitable for everyone. Ask your respiratory physiotherapist for advice.
Further reading
- Airways Mucus and Aspergillosis
- Understanding Mucous Casts in Allergic Bronchopulmonary Aspergillosis (ABPA)
- ABPA: Allergic Reaction or Fungal Presence in the Lungs?
- Aspergillus Bronchitis: A Patient Guide
- Managing Life with Haemoptysis
- Haemoptysis: Emergency Information
- Managing Cough in Aspergillosis: A Patient Guide
References
- British Thoracic Society Guideline for Bronchiectasis in Adults
- British Thoracic Society Guideline for Bronchiectasis in Adults, Thorax
- European Respiratory Society clinical practice guideline for bronchiectasis management
- BTS Guideline for Bronchiectasis in Adults: summary for the general public
Author: National Aspergillosis Centre
Last medically reviewed: 6 July 2026
This information is intended to support, not replace, advice from your own healthcare professionals.
```
Mindfulness, Meditation and Relaxation for People Living with Aspergillosis

Living with aspergillosis can be physically and emotionally demanding. Many people describe feeling anxious about breathlessness, frustrated by fatigue, worried while waiting for test results, or overwhelmed by the uncertainty of living with a long-term condition.
These feelings are entirely understandable. Mindfulness is not a treatment for aspergillosis, but many people find that it helps them manage stress, cope more effectively with symptoms, and improve their overall quality of life alongside their medical care.
Several people living with aspergillosis have told us that mindfulness, meditation or related approaches have helped them cope with the emotional challenges of living with a long-term respiratory condition. Some describe it as being similar to cognitive behavioural therapy (CBT), because it can help them notice anxious thoughts, recognise unhelpful cycles, and respond more calmly.
Mindfulness and CBT are not the same thing, but there is overlap. Both can help people become more aware of how thoughts, feelings, physical sensations and behaviours influence each other. This may be especially relevant when breathlessness, anxiety and stress start to reinforce one another.
Mind and body are connected. Our thoughts and feelings can affect how we breathe, and our breathing can affect how we feel. Mindfulness may help some people break the cycle of stress, anxiety and breathlessness.
What is mindfulness?
Mindfulness means paying attention to the present moment with openness and without judgement. It involves noticing your thoughts, emotions and body sensations as they are happening, rather than becoming caught up in worries about the future or memories of the past.
The NHS describes mindfulness as becoming more aware of what is happening both inside ourselves and in the world around us. This greater awareness can help us recognise stress earlier and respond to it in healthier ways.
Can mindfulness help?
Research suggests that mindfulness-based approaches may help some people living with long-term health conditions by:
- reducing stress and anxiety
- improving emotional wellbeing
- helping people cope with uncertainty
- improving sleep in some individuals
- increasing confidence in managing long-term illness
- supporting overall quality of life
Mindfulness is not a replacement for medical treatment, but it may be a useful addition to an overall self-management plan.
Mindfulness and breathing
Breathing is central to many mindfulness exercises.
People living with aspergillosis may become understandably focused on their breathing, particularly during episodes of breathlessness. Gentle breathing awareness can help some people slow their breathing, reduce feelings of panic and regain a greater sense of control.
The aim is not to force deeper breaths, but to develop a calm awareness of your natural breathing pattern.
If you become uncomfortable or increasingly breathless during any exercise, stop and return to your normal breathing. Always follow the advice of your respiratory team if you have concerns about breathlessness.
Meditation
Meditation is one way of practising mindfulness. Even five to ten minutes each day may help you develop greater awareness of your breathing, thoughts and emotions.
There are many different styles of meditation. Some focus on breathing, while others use guided relaxation, body awareness or gentle visualisation. There is no single correct approach, so it is worth trying different techniques to discover what works best for you.
Tai Chi and Yoga
Gentle activities such as Tai Chi and yoga combine movement, breathing and relaxation. Many people with chronic respiratory conditions find these activities helpful for improving confidence, flexibility, balance and emotional wellbeing.
Choose exercises that match your current level of fitness and avoid pushing yourself beyond your comfort level. If you are unsure whether an activity is suitable, discuss it with your healthcare team.
Getting started
You do not need any special equipment or previous experience.
You could begin by:
- spending five minutes focusing on your breathing each day
- taking a slow, mindful walk while noticing your surroundings
- trying a guided mindfulness session
- practising gentle stretching, yoga or Tai Chi
- using relaxation exercises before bed or during stressful periods
Many people find that practising little and often is easier than trying long sessions.
Useful resources
- NHS: Mindfulness
- NHS: Stress, anxiety and wellbeing support
- Aspergillosis.org: Living well with aspergillosis
You may also find it helpful to explore aspergillosis.org resources on breathing exercises, fatigue, emotional wellbeing, exercise and gentle movement.
When should I seek additional support?
Living with a long-term illness can affect emotional wellbeing. If anxiety, low mood or stress are becoming overwhelming, speak with your GP or specialist team. Support is available, and looking after your mental wellbeing is an important part of living well with aspergillosis.
Originally published: July 2018
Last substantially updated: July 2026
Next review due: July 2028
Living with Aspergillosis: Understanding the Brain–Lung Connection
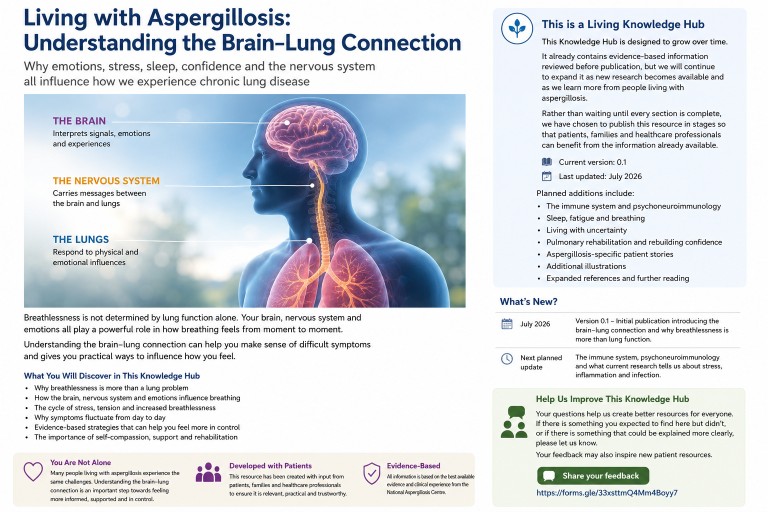
Why emotions, stress, sleep, confidence and the nervous system all influence how we experience chronic lung disease
Aspergillosis Living Knowledge Hub | Built with patients | Living document
This is a Living Knowledge Hub
Unlike a traditional article, this Knowledge Hub is designed to evolve.
As new scientific research becomes available, and as people living with aspergillosis ask new questions, we will continue to expand and improve this resource.
The current version already contains evidence-based information that has been reviewed before publication, but it is only the beginning.
This approach allows us to share useful information now, rather than waiting until every section is complete, while continuing to improve the resource over time.
- Current version: 0.1
- Last updated: July 2026
- Status: Living Knowledge Hub
- Reading time: approximately 18 minutes
- Who is this for? People living with aspergillosis, families, carers and healthcare professionals
- Review policy: This Knowledge Hub is reviewed whenever important new evidence becomes available and at least annually to ensure it remains accurate and up to date.
Planned additions
- The immune system and psychoneuroimmunology
- Sleep, fatigue and breathing
- Stress hormones, inflammation and infection
- Living with uncertainty
- Pulmonary rehabilitation and rebuilding confidence
- Additional illustrations and diagrams
- Expanded references and further reading
Contents
Before you begin...
If you have arrived here because someone suggested that stress or anxiety might be affecting your breathing, this page is for you.
If you have arrived here because you are wondering why some days are so much harder than others, this page is for you.
If you have ever worried that family members, friends or even healthcare professionals thought your symptoms were “all in your head”, this page is for you too.
And if you are a family member or healthcare professional trying to understand what it is really like to live with aspergillosis, we hope this guide helps explain an aspect of chronic lung disease that is rarely discussed in detail.
The most important message comes first.
Your illness is real.
Your symptoms are real.
Modern respiratory medicine recognises that the brain, lungs, nervous system and immune system constantly work together. Understanding that relationship does not make your illness any less real. It helps explain why living with chronic lung disease can sometimes be so challenging.
Why we wrote this guide
Over many years at the National Aspergillosis Centre, we have listened to many people living with aspergillosis.
Again and again, we hear similar questions.
“Why do I feel much worse today when my scan hasn’t changed?”
“Why does poor sleep affect my breathing so much?”
“Can stress make my symptoms worse?”
“If my emotions affect my breathing, does that mean my illness isn’t real?”
These are important questions. Unfortunately, they can be difficult to answer fully during a busy clinic appointment.
This guide has been written to provide the explanation many people tell us they never had.
It brings together modern respiratory medicine, neuroscience, immunology, pulmonary rehabilitation and the lived experience of people with aspergillosis.
Our aim is not simply to explain the science. Our aim is to help you understand your own experience.
A false choice
Many people living with chronic illness feel they have been offered two very different explanations for their symptoms.
Either the symptoms are caused by the lungs, or the symptoms are caused by anxiety.
Modern medicine increasingly recognises that this is a false choice.
The lungs are real. The brain is real. The nervous system is real. The immune system is real. Hormones are real.
Every one of these systems communicates continuously with the others. When we understand that partnership, many experiences that once seemed confusing begin to make sense.
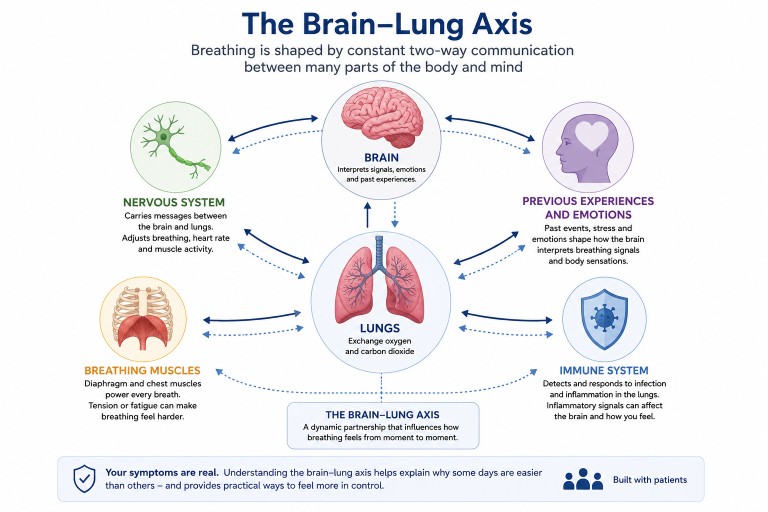
More than just the lungs
Most of us think breathing happens entirely inside the lungs. In reality, every breath depends on an extraordinary partnership between many different parts of the body.
| Body system | Its role in breathing |
|---|---|
| The lungs | Exchange oxygen and carbon dioxide. |
| The brain | Interprets breathing signals and decides how much air the body needs. |
| The nervous system | Adjusts breathing, heart rate and muscle activity. |
| The breathing muscles | Power every breath you take. |
| The immune system | Responds to infection and inflammation in the lungs. |
| Your previous experiences | Help the brain judge whether breathing feels safe or threatening. |
Scientists often describe this constant communication as the brain–lung axis.
Understanding how this partnership works has transformed the way respiratory specialists think about chronic breathlessness.
What you will learn
By the end of this guide you will understand:
- why scans and lung function tests do not always match how you feel
- why frightening experiences can change the way breathing feels
- why sleep, fatigue and emotions influence symptoms
- what scientists know about stress and the immune system
- why pulmonary rehabilitation works
- how confidence can be rebuilt after serious illness
- what is known, and what is still uncertain, about these important questions.
If you remember only one thing from this opening section, remember this:
Your illness is real. Your symptoms are real. The science that explains the connection between the brain and lungs is real too.
Why Does My Breathing Feel Worse When My Scan Hasn’t Changed?
This is probably one of the most common questions asked by people living with chronic lung disease.
“My doctor says my CT scan looks stable, so why do I feel so much worse?”
It is an excellent question. It is also one that causes enormous frustration.
Many people begin wondering whether they are imagining their symptoms or whether something has been missed.
Fortunately, modern respiratory medicine has a much better explanation.
The first thing to understand
A CT scan is an extraordinarily useful investigation. It allows doctors to see inflammation, cavities, bronchiectasis, scarring and many other important changes inside the lungs.
But a scan has one important limitation.
It shows what your lungs look like.
It cannot show what breathing feels like.
Those are two different things.
Structure versus function
A useful way to think about this is to separate structure from function.
| Structure | Function and lived experience |
|---|---|
| CT scans | Breathing comfort and effort |
| X-rays | Exercise tolerance |
| Blood tests | Energy and fatigue |
| Lung function tests | Quality of life and confidence |
Your medical team needs both kinds of information. One does not replace the other.
Breathlessness is an experience
The American Thoracic Society defines breathlessness, also called dyspnoea, as:
“A subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity.”
That definition is important. It tells us that breathlessness is something that is experienced.
The lungs send information. The brain turns that information into the experience of breathing.
An orchestra, not a solo instrument
Imagine listening to an orchestra. You do not hear only the violins. You hear the combined sound of strings, woodwind, brass and percussion.
Breathing works in much the same way. What you experience is produced by many different systems working together.
| System | Contribution |
|---|---|
| Lungs | Move oxygen and carbon dioxide. |
| Heart | Delivers oxygen. |
| Breathing muscles | Generate each breath. |
| Brain | Interprets signals. |
| Nervous system | Adjusts breathing. |
| Sleep | Influences fatigue and resilience. |
| Confidence | Changes how safe breathing feels. |
| Previous experiences | Influence future breathing responses. |
No single instrument produces the whole performance.
What your scan cannot see
Your CT scan cannot show:
- how well you slept
- whether your breathing muscles are tired
- whether you recently recovered from a viral infection
- whether you feel anxious about another haemoptysis
- whether today’s humidity is making your chest feel tight
- whether your body is still recovering from yesterday’s activity
- how much mental effort breathing requires today.
All of these may influence how breathing feels. None of them mean your illness is imaginary.
Research Spotlight
Why the modern definition of breathlessness matters
Older medical thinking often treated breathlessness as a simple consequence of lung damage.
Research over recent decades has shown that the experience of breathlessness depends upon interactions between the lungs, brain, nervous system and many other factors.
This is why modern respiratory medicine increasingly measures quality of life alongside scans and lung function tests.
Why this matters: it validates what patients have always known: how they feel cannot always be predicted by test results alone.
Why this matters if you have aspergillosis
If your scan has not changed but your breathing feels worse, this does not automatically mean:
- the disease has suddenly progressed
- the scan is wrong
- your symptoms are “all in your head”.
It means breathing is influenced by many different parts of the body working together.
Understanding those interactions is one of the biggest advances in modern respiratory medicine.
Why Does the Brain Matter If My Lungs Are the Problem?
This question worries many people.
“If my doctor starts talking about my brain, are they saying my illness isn’t real?”
The answer is simple. No.
Talking about the brain is not changing the diagnosis. It is explaining how breathing works.
Your lungs cannot create the sensation of breathlessness on their own, just as your ears cannot create music on their own, or your eyes cannot create vision on their own.
Every one of these experiences depends on the brain interpreting information coming from the body. Breathing is no different.
Your brain is your body’s prediction machine
Most of us imagine the brain as a computer that simply receives information. Modern neuroscience paints a much more interesting picture.
The brain is constantly trying to predict what is about to happen.
Every second it asks questions such as:
- Am I safe?
- Am I getting enough oxygen?
- Should I breathe faster?
- How hard are my breathing muscles working?
- Does this feel familiar?
It compares what it expects to happen with what is actually happening.
If everything matches, breathing usually fades into the background. If something unexpected happens, breathing suddenly becomes the centre of attention.
This is one reason healthy people rarely notice their breathing, while people living with chronic lung disease may think about it many times each day.
The smoke alarm inside your brain
A smoke alarm has one job: to detect danger. It would rather ring unnecessarily than miss a real fire.
Your brain works in much the same way.
If you have experienced:
- a severe asthma attack
- haemoptysis
- being unable to catch your breath
- an emergency admission to hospital
- months of unexplained symptoms before diagnosis
your brain learns something very important.
“Breathing can sometimes become dangerous.”
Once that lesson has been learned, your brain naturally pays much closer attention to breathing than it did before.
This is not a fault. It is exactly what evolution intended. Your brain is trying to protect you.
Patient Perspective
“After coughing up blood I became frightened every time I coughed.
I knew the bleeding had stopped, but every cough made me wonder whether it was happening again.
Learning that my brain was trying to protect me, not trick me, changed the way I understood my recovery.”
The Brain–Lung Axis
Scientists describe the close communication between the brain and lungs as the brain–lung axis.
This communication works in both directions.
| The lungs tell the brain... | The brain tells the lungs... |
|---|---|
| How much oxygen is available. | How fast to breathe. |
| How much carbon dioxide is present. | How deeply to breathe. |
| Whether the airways are irritated. | When to cough. |
| How hard the breathing muscles are working. | How to respond to exercise. |
Every breath is the result of this continuous conversation.
Why this matters if you have aspergillosis
If you understand that breathing is created by a partnership between the lungs and brain, several confusing experiences suddenly make much more sense.
- Why one day can feel much harder than another.
- Why sleep affects breathing.
- Why fatigue affects breathing.
- Why confidence affects breathing.
- Why pulmonary rehabilitation improves symptoms even when scans remain unchanged.
- Why frightening respiratory events can continue to affect confidence long after the lungs have recovered.
None of these observations suggest your illness is psychological.
They demonstrate how remarkably sophisticated the breathing system really is.
Research Spotlight
Brain imaging studies have shown that breathlessness activates areas of the brain involved in attention, emotion and decision-making, as well as areas involved in sensory processing.
This reinforces an important message:
Breathlessness is not simply a signal from the lungs. It is a whole-body experience.
Can Emotions Really Change My Breathing?
Many people living with aspergillosis are reluctant to ask this question.
Some worry that even mentioning stress or emotions will mean their symptoms are no longer taken seriously. Others have experienced exactly that in the past.
Modern respiratory medicine takes a very different view.
It recognises two equally important facts.
- Your lung disease is real.
- Your emotional state can influence how that disease is experienced.
These statements are not contradictory. They describe how the human body normally works.
Every emotion has a physical effect
Think about the last time you were startled. Before you had time to think, your body had already responded.
- Your heart rate increased.
- Your breathing became faster.
- Your muscles tightened.
- Your mouth became dry.
- Your attention narrowed onto the potential danger.
You did not choose any of those reactions. They happened automatically.
This is because emotions are not separate from the body. They are produced by the body and immediately affect the body’s physiology.
Breathing is especially sensitive
Unlike many other organs, the breathing system has to respond continuously to both physical demands and emotional demands.
| Situation | What happens? |
|---|---|
| Walking upstairs | Your breathing increases because your muscles need more oxygen. |
| Receiving frightening news | Your breathing may also increase, even though your muscles are resting. |
| Laughing | Your breathing pattern changes completely. |
| Crying | Your breathing becomes irregular and deeper. |
| Feeling calm and relaxed | Your breathing usually slows and becomes more efficient. |
These changes happen in everyone.
People with chronic lung disease often notice them more because their breathing system is already working harder.
Why frightening experiences matter
Imagine two people climbing exactly the same flight of stairs.
One has never experienced serious breathing problems. The other has previously been admitted to hospital with severe breathlessness.
Their lungs may be working equally hard. But their brains interpret those signals differently.
The first person thinks:
“I’m out of breath because I climbed the stairs.”
The second person may immediately wonder:
“Is something going wrong again?”
Neither response is irrational. They reflect different life experiences.
This is one reason why previous severe respiratory events can continue to influence confidence long after recovery.
Patient Perspective
“I realised I wasn’t frightened of exercise.
I was frightened of becoming breathless because, in the past, breathlessness had meant I was seriously ill.”
The vicious circle of fear
Fear itself does not damage the lungs. However, fear can unintentionally make breathing feel more difficult.
Breathlessness
↓
Concern
↓
Breathing becomes faster
↓
Chest muscles tighten
↓
Breathing feels harder
↓
More concern
This is not imaginary. Every stage involves genuine physical changes.
The encouraging news is that this cycle can also be interrupted.
Understanding
↓
Greater confidence
↓
Calmer breathing
↓
More efficient breathing
↓
Activity feels easier
↓
Confidence grows
This does not remove aspergillosis. It changes how effectively the whole breathing system works together.
Research Spotlight
Why pulmonary rehabilitation improves confidence
Research consistently shows that pulmonary rehabilitation improves quality of life, exercise capacity and confidence, even when lung function changes only modestly.
Patients often describe feeling more in control of their breathing.
This improvement reflects better physical conditioning, improved breathing efficiency, increased confidence and a better understanding of symptoms.
These benefits are recognised internationally and form an important part of managing many chronic respiratory diseases.
Why this matters if you have aspergillosis
You are not expected to ignore your emotions.
You are not expected to “stay positive” all the time.
You are not expected to pretend your illness is less serious than it is.
Instead, understanding how emotions influence breathing gives you another tool.
It helps explain why:
- some days feel harder than others
- confidence matters
- breathing techniques can help
- pulmonary rehabilitation works
- being listened to is part of good medical care
Knowledge does not remove the disease.
But it can remove unnecessary fear and replace it with understanding.
Emotions do not make aspergillosis imaginary.
They are one of the many biological systems that influence how living with aspergillosis feels from day to day.
What's New?
This Knowledge Hub is updated regularly as new evidence becomes available and in response to questions from readers.
Version 0.1 – July 2026
- Initial publication.
- Introduced the Brain–Lung Connection.
- Explained why breathlessness is more than lung function alone.
- Explored how previous experiences and emotions can influence breathing.
Next planned update
- The immune system and psychoneuroimmunology.
- Stress hormones, inflammation and infection.
- Sleep and breathing.
Help Shape Future Editions
Every month we review this Knowledge Hub.
Some improvements come from newly published scientific research.
Others come directly from the questions and experiences shared by people living with aspergillosis, their families and healthcare professionals.
Many of the most valuable pages on aspergillosis.org have started with a single patient question.
If there was something you expected to find but didn't...
If something wasn't explained clearly...
If your own experience has been different...
Or if there is a question you think every patient should have answered...
Please tell us.
Your feedback will help shape future editions of this Knowledge Hub and may inspire entirely new patient resources.
📝 Share your feedback (2–3 minutes)
Thank you for helping us build one of the world's most comprehensive patient education resources on aspergillosis.
This Knowledge Hub has evolved thanks to our readers
Future updates will be listed here so you can see how this resource has grown over time.
| Version | What's changed |
|---|---|
| 0.1 | Initial publication introducing the Brain–Lung Connection, explaining why breathlessness is more than lung function, and describing how previous experiences and emotions can influence breathing. |
| 0.2 | Coming soon: immune system, psychoneuroimmunology, stress hormones, inflammation and sleep. |
| 0.3 | Coming soon. |
| 1.0 | First complete edition. |
Further reading and references
- American Thoracic Society Statement: Update on the Mechanisms, Assessment, and Management of Dyspnea
- American Thoracic Society PDF: Mechanisms, Assessment, and Management of Dyspnea
- American Thoracic Society patient information: Pulmonary Rehabilitation
- British Thoracic Society: Pulmonary Rehabilitation resources
- Global Initiative for Asthma (GINA)
- Global Initiative for Chronic Obstructive Lung Disease (GOLD)
- PubMed search: brain imaging and dyspnoea reviews
- PubMed search: quality of life in chronic pulmonary aspergillosis
- Aspergillosis Patients & Carers website
Suggested citation: National Aspergillosis Centre. Living with Aspergillosis: Understanding the Brain–Lung Connection. Aspergillosis.org. Version 0.1. July 2026.
Weekly Aspergillosis Research Update: June 29
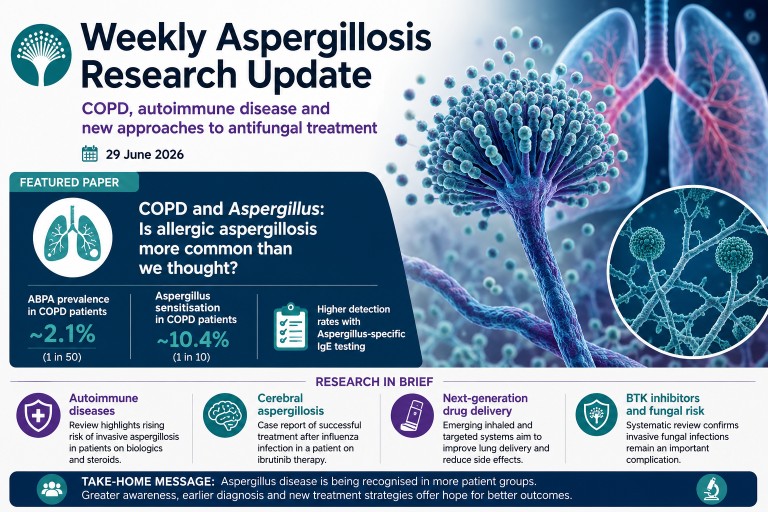
COPD, autoimmune disease and new approaches to antifungal treatment
Published: 29 June 2026
Every week we review the latest research on aspergillosis and related fungal diseases, selecting the studies most likely to influence patient care and clinical practice. This week's research focuses on an increasingly important theme: recognising Aspergillus disease in patient groups where it has traditionally been overlooked.
The highlight is a large systematic review suggesting that allergic Aspergillus disease may be more common in people living with chronic obstructive pulmonary disease (COPD) than previously appreciated.
Featured Paper
COPD and Aspergillus: Is allergic aspergillosis more common than we thought?
For decades, allergic bronchopulmonary aspergillosis (ABPA) has been regarded primarily as a complication of asthma and cystic fibrosis. However, respiratory specialists have increasingly reported Aspergillus-related disease in patients with COPD.
A new systematic review and meta-analysis has now brought together the available evidence.
Paper: Ajayababu A, Antony A, Goyal B, Ray A. Prevalence of allergic bronchopulmonary aspergillosis/Aspergillus sensitization in chronic obstructive pulmonary disease: A systematic review and meta-analysis. Respiratory Investigation. 2026. PubMed PMID: 42361722
What did the researchers do?
The authors searched four major medical databases for studies reporting either:
- Allergic bronchopulmonary aspergillosis (ABPA)
- Aspergillus sensitisation (AS)
Among patients with COPD, the review identified 23 suitable studies, including:
- 1,529 patients for analysis of ABPA
- 3,505 patients for analysis of Aspergillus sensitisation
Pooling data from many studies provides a more reliable estimate than individual reports alone.
What did they find?
The results suggest Aspergillus-related disease is not rare in COPD.
The pooled prevalence was:
- ABPA: 2.1%
- Aspergillus sensitisation: 10.4%
Put another way:
- around 1 in 50 people with COPD may have ABPA
- approximately 1 in 10 have evidence of sensitisation to Aspergillus
Studies using Aspergillus-specific IgE as part of their diagnostic strategy detected more ABPA than studies using skin testing or total IgE alone. This suggests that the choice of diagnostic tests may influence how many patients are identified.
Why is this important?
Many symptoms of COPD overlap with Aspergillus-related disease, including:
- persistent cough
- breathlessness
- increased sputum production
- recurrent exacerbations
As a result, some patients may continue to receive repeated courses of antibiotics or steroids while an underlying Aspergillus-related condition remains unrecognised.
This study does not suggest that everyone with COPD should undergo routine fungal testing. However, it supports considering Aspergillus investigations in selected patients with:
- recurrent exacerbations despite optimal therapy
- unexplained eosinophilia or raised IgE
- bronchiectasis
- persistent mucus plugging
- radiological abnormalities that do not fit the expected pattern
Strengths and limitations
This is currently one of the largest reviews examining COPD and Aspergillus disease.
Its strengths include:
- systematic literature search
- formal meta-analysis
- inclusion of more than 5,000 patients overall
However, the included studies differed considerably in patient populations, diagnostic methods and disease severity. This statistical heterogeneity means the true prevalence almost certainly varies between different clinical settings.
The review also demonstrates an association rather than proving that COPD itself causes ABPA.
What does this mean for patients?
The main message is one of greater awareness.
For patients with COPD whose symptoms remain difficult to explain despite appropriate treatment, clinicians may increasingly consider whether Aspergillus sensitisation or ABPA could be contributing to ongoing respiratory problems.
Earlier recognition has the potential to improve diagnosis and ensure that patients receive the most appropriate investigations and treatment.
Research in Brief
Invasive aspergillosis in autoimmune inflammatory rheumatic diseases
Paper: Liang P, Zhang X, Cai S, Hu Z, Dong L. Invasive aspergillosis in autoimmune inflammatory rheumatic diseases: epidemiology, risk factors, diagnosis, management and challenges. Annals of Medicine. 2026. PubMed PMID: 42343869
A comprehensive new review highlights the growing importance of invasive aspergillosis in people with autoimmune inflammatory rheumatic diseases such as rheumatoid arthritis and systemic vasculitis.
The increasing use of corticosteroids, biologic therapies and other immunosuppressive medications has expanded the population at risk. The authors note that invasive aspergillosis remains uncommon but carries a high mortality when diagnosis is delayed.
A particular challenge is that symptoms and imaging findings can resemble a flare of the underlying autoimmune disease, making diagnosis difficult. The review emphasises combining clinical assessment with microbiological tests, including galactomannan, PCR and bronchoalveolar lavage where appropriate, and careful interpretation of imaging findings.
Why it matters: Clinicians should maintain a high index of suspicion for invasive fungal disease in immunosuppressed patients who fail to respond as expected to conventional treatment.
Cerebral aspergillosis following influenza and ibrutinib therapy
Paper: Haraguchi M, Kimura M, Uruga H, Takahashi Y, Takaya H, Arisawa K, et al. Cerebral aspergillosis caused by Aspergillus flavus following seasonal influenza infection in a patient receiving ibrutinib for Waldenström's macroglobulinemia. Journal of Infection and Chemotherapy. 2026. PubMed PMID: 42331321
A Japanese case report describes successful treatment of cerebral aspergillosis caused by Aspergillus flavus in a patient receiving the Bruton tyrosine kinase inhibitor ibrutinib after seasonal influenza infection.
The patient developed both pulmonary and cerebral aspergillosis, underwent neurosurgical debridement and was successfully treated with isavuconazole.
Although this represents a single case, it reinforces growing evidence that BTK inhibitors and severe viral infections are emerging risk factors for invasive aspergillosis.
Why it matters: Patients receiving targeted therapies who develop persistent respiratory or neurological symptoms following influenza warrant careful assessment for opportunistic fungal infection.
Looking ahead: New ways to deliver antifungal drugs
Paper: Martins YA, Anselmo-Lima WT, Tamashiro E, Ho E, Valera FCP. Next-generation drug delivery systems for aspergillosis: Overcoming barriers in antifungal therapy. Biomedicine & Pharmacotherapy. 2026. PubMed PMID: 42361622
Another review this week explores next-generation drug delivery systems designed to improve treatment of aspergillosis.
Researchers are developing inhaled formulations, nanoparticles and targeted drug-delivery technologies that aim to increase antifungal concentrations directly within the lungs while reducing systemic side effects.
Most of these approaches remain experimental, but they offer possibilities for the future management of chronic pulmonary aspergillosis and other forms of pulmonary fungal disease.
What this week's research tells us
Although these papers address different aspects of aspergillosis, they all point in the same direction.
Increasingly, Aspergillus disease is being recognised in patient groups previously considered to be at relatively low risk, including people with COPD and those receiving modern immunosuppressive therapies.
At the same time, advances in diagnostics and drug delivery are creating opportunities for earlier diagnosis and more targeted treatment.
For patients, the message is reassuring but important: persistent or unexplained respiratory symptoms deserve careful evaluation, particularly when standard treatments are not achieving the expected improvement.
As awareness continues to grow, more patients may receive the correct diagnosis earlier in the course of their illness.
References
- Ajayababu A, Antony A, Goyal B, Ray A. Prevalence of allergic bronchopulmonary aspergillosis/Aspergillus sensitization in chronic obstructive pulmonary disease: A systematic review and meta-analysis. Respiratory Investigation. 2026. doi:10.1016/j.resinv.2026.101469. PubMed
- Liang P, Zhang X, Cai S, Hu Z, Dong L. Invasive aspergillosis in autoimmune inflammatory rheumatic diseases: epidemiology, risk factors, diagnosis, management and challenges. Annals of Medicine. 2026. doi:10.1080/07853890.2026.2685285. PubMed
- Haraguchi M, Kimura M, Uruga H, Takahashi Y, Takaya H, Arisawa K, et al. Cerebral aspergillosis caused by Aspergillus flavus following seasonal influenza infection in a patient receiving ibrutinib for Waldenström's macroglobulinemia. Journal of Infection and Chemotherapy. 2026. doi:10.1016/j.jiac.2026.103020. PubMed
- Martins YA, Anselmo-Lima WT, Tamashiro E, Ho E, Valera FCP. Next-generation drug delivery systems for aspergillosis: Overcoming barriers in antifungal therapy. Biomedicine & Pharmacotherapy. 2026. doi:10.1016/j.biopha.2026.119691. PubMed
```
Catch Up on the Latest National Aspergillosis Centre Monthly Update
DNA Diagnostics, Adrenal Health, Damp Homes Research and Community Discussion
The National Aspergillosis Centre (NAC) Monthly Update brings together patients, carers, healthcare professionals and researchers to discuss the latest developments in aspergillosis care, research and day-to-day management.
Held on the first Friday of each month, these sessions combine expert presentations, research updates, practical information and community discussion. They provide an opportunity to learn about emerging developments in diagnosis and treatment while hearing directly from people living with aspergillosis and other chronic respiratory conditions.
In this month's update we discussed several important topics, including respiratory virus activity, corticosteroid management, adrenal insufficiency, new DNA-based diagnostic technologies and research into damp homes and mould exposure.
If you were unable to join us live, the full recording is available below.
Watch the Recording
Watch the full National Aspergillosis Centre Monthly Update using the embedded YouTube player below.
What Was Covered?
Respiratory Viruses and Seasonal Infections
The meeting opened with a discussion of current respiratory virus activity and the ongoing challenges that infections can present for people living with chronic respiratory disease.
Topics included seasonal trends, infection prevention and the importance of remaining aware of changing respiratory virus activity throughout the year.
Chapter: 24:30
Improving Corticosteroid Management
Corticosteroids remain an important treatment for many people with allergic and inflammatory lung conditions, including some forms of aspergillosis. However, long-term steroid use can also lead to significant side effects and complications.
This session explored current approaches to steroid management and the importance of balancing symptom control with minimising long-term risks.
Topics included:
- Why corticosteroids are used
- Monitoring treatment effectiveness
- Recognising steroid-related side effects
- Practical challenges faced by patients
Chapters: 25:30–58:00
Adrenal Insufficiency and Cortisol Replacement
A major focus of the meeting was adrenal insufficiency, a condition that can develop when prolonged corticosteroid treatment suppresses the body's natural cortisol production.
Discussion included:
- How adrenal insufficiency develops
- Common symptoms and warning signs
- Cortisol replacement therapy
- Managing illness and stress when adrenal function is reduced
- Questions raised by patients with lived experience
For many attendees this was one of the most relevant and practical discussions of the session.
Chapter: 27:00
New Approaches to Steroid Replacement Therapy
The meeting also explored newer approaches to cortisol replacement therapy that aim to more closely mimic the body's natural hormone rhythms.
Research in this area continues to develop and may improve quality of life for some patients in the future.
Chapter: 36:00
DNA-Based Bedside Diagnostics
One of the most exciting research topics discussed was the development of rapid DNA-based diagnostic technologies.
Traditional fungal diagnosis can sometimes take days or even weeks. New molecular approaches have the potential to identify pathogens much more quickly, helping clinicians make earlier and more informed treatment decisions.
The discussion explored:
- How DNA-based diagnostics work
- Why rapid diagnosis matters
- Current research developments
- Potential future applications in clinics and hospitals
Chapter: 58:00
How Rapid Genetic Testing Could Change Fungal Diagnosis
Advances in molecular biology and sequencing technology are opening the possibility of identifying fungal infections directly from patient samples without the need for lengthy culture-based methods.
Potential benefits include:
- Faster diagnosis
- Earlier treatment decisions
- Improved identification of difficult-to-detect infections
- More personalised approaches to care
Although many technologies remain under evaluation, this is one of the most rapidly developing areas of fungal medicine.
Chapter: 01:05:00
Damp Homes, Mould and Health Research
The second half of the update focused on growing evidence linking damp indoor environments and mould exposure to respiratory health problems.
This topic has received increasing attention following recent public health initiatives and growing awareness of housing-related health risks.
Discussion included:
- Current evidence linking damp homes and respiratory disease
- Ongoing research projects
- Challenges in measuring exposure
- Areas where further research is needed
Chapter: 01:55:00
Citizen Science Damp Homes and Health Project
Attendees also heard about the Citizen Science Damp Homes and Health Project, which aims to involve members of the public directly in collecting data and contributing to research.
Citizen science projects have the potential to improve understanding of real-world housing conditions and their impact on respiratory health.
Chapter: 01:56:00
Why Damp and Mould Matter for Respiratory Health
The meeting explored the ways in which damp environments can contribute to poor respiratory health, including increased exposure to mould spores, allergens and other environmental factors.
For people living with asthma, bronchiectasis and aspergillosis, understanding these risks can be an important part of managing their condition.
Chapter: 02:05:00
Patient Experiences and Open Discussion
As always, one of the most valuable aspects of the Monthly Update was the opportunity for attendees to share experiences, ask questions and support one another.
These discussions help connect people facing similar challenges while providing valuable insight into the real-world impact of living with aspergillosis.
Chapter Guide
- 00:00 Welcome and introductions
- 00:25 Community catch-up and discussion
- 24:30 Respiratory virus update and seasonal infections
- 25:00 Meeting agenda and topic selection
- 25:30 Improving corticosteroid management
- 27:00 Adrenal insufficiency and cortisol replacement
- 36:00 New approaches to steroid replacement therapy
- 43:00 Questions and discussion
- 58:00 DNA-based bedside diagnostics
- 01:05:00 How rapid genetic testing could change fungal diagnosis
- 01:20:00 Questions and patient discussion
- 01:31:00 Break and community discussion
- 01:55:00 Damp homes, mould and health research
- 01:56:00 Citizen Science Damp Homes and Health Project
- 02:05:00 Why damp and mould matter for respiratory health
- 02:20:00 Patient experiences and questions
- 02:30:00 Meeting summary and closing discussion
Why We Share These Updates
Not everyone can attend live events. Health issues, work commitments, caring responsibilities and geographical distance can all make participation difficult.
By recording and sharing our Monthly Updates, we hope to make expert information, research developments and community discussion accessible to as many people as possible.
The recordings also provide a valuable archive of emerging research, practical advice and patient experiences that can help people better understand and manage aspergillosis.
Join Future Monthly Updates
The National Aspergillosis Centre hosts regular online community meetings throughout the month, alongside the longer Monthly Update held on the first Friday.
Whether you are newly diagnosed, caring for someone with aspergillosis or have been living with the condition for many years, you are very welcome to join us.
For information about future events and resources, visit:
Weekly Aspergillosis Research Update: New Diagnostics, CAPA Evidence, and Why Azole Tolerance Matters
Last reviewed: 23 June 2026
Author: National Aspergillosis Centre Team
Audience: People living with aspergillosis, carers, healthcare professionals, and interested readers.
In one sentence: This week's aspergillosis research highlights a possible new bronchoscopic approach to aspergilloma management, growing use of PCR diagnostics, a major review of COVID-19-associated pulmonary aspergillosis, and new discoveries explaining how Aspergillus fumigatus may survive antifungal treatment.
Research Highlight of the Week
Why azole tolerance is more complex than resistance
The most important scientific theme this week is the growing recognition that Aspergillus fumigatus can sometimes survive antifungal treatment without possessing classic resistance mutations. Three separate studies suggest that iron availability, cellular stress responses, epigenetic regulation and long non-coding RNA may all influence how the fungus responds to azole drugs. These findings do not change treatment today, but they could shape future approaches to antifungal resistance monitoring and antifungal drug development.
Who Should Read This Update?
This update may be particularly relevant for:
- People living with chronic pulmonary aspergillosis (CPA)
- People with aspergilloma or a history of haemoptysis (coughing up blood)
- Patients receiving antifungal treatment such as itraconazole, voriconazole, posaconazole or isavuconazole
- Healthcare professionals interested in aspergillosis diagnostics and antifungal resistance
- Anyone following developments in fungal disease research
Key Points
- A study explored bronchoscopic removal of aspergilloma in selected patients with post-tuberculosis chronic cavitary pulmonary aspergillosis.
- Real-time polymerase chain reaction (PCR) testing may provide additional support when diagnosing invasive aspergillosis.
- A major review confirms that COVID-19-associated pulmonary aspergillosis (CAPA) remains a serious complication of severe COVID-19.
- New research suggests that antifungal treatment response is influenced by much more than simple resistance mutations.
- None of these findings should lead patients to change treatment without specialist medical advice.
Contents
- Overview
- A possible new approach for aspergilloma
- PCR testing and invasive aspergillosis
- COVID-19-associated pulmonary aspergillosis
- Why azole tolerance is more complex than resistance
- Also noted this week
- What this means for patients
- When to speak to your clinical team
- References
Overview
Research into aspergillosis continues to advance on several fronts. This week's papers range from practical clinical studies investigating new ways to manage aspergilloma, through to laboratory research exploring how Aspergillus fumigatus survives antifungal treatment.
While none of these studies are likely to change patient care immediately, they highlight important trends in the field. Researchers are working to improve diagnosis, develop new treatment approaches, and better understand why some infections persist despite treatment.
The strongest overall message this week is that aspergillosis research is moving beyond simple categories such as “susceptible” or “resistant”. Aspergillus fumigatus can adapt to stress, tolerate antifungal pressure, and sometimes survive long enough to acquire more stable resistance.
Most of the studies featured this week improve our understanding of aspergillosis rather than changing treatment directly. Nevertheless, several findings point towards future improvements in diagnosis, patient monitoring and antifungal therapy.
A Possible New Approach for Aspergilloma
One of the most clinically interesting papers this week investigated bronchoscopic removal of aspergilloma in patients with post-tuberculosis chronic pulmonary aspergillosis (CPA).
An aspergilloma, sometimes called a fungal ball, develops when Aspergillus grows within an existing cavity in the lung. These cavities can develop after conditions such as tuberculosis, sarcoidosis, or previous severe lung infections.
Post-tuberculosis chronic cavitary pulmonary aspergillosis refers to CPA developing in lung cavities left behind after previous tuberculosis.
Traditionally, treatment options include antifungal medication, surgery in carefully selected patients, and procedures such as bronchial artery embolisation to control significant bleeding.
This study explored whether bronchoscopy could be used to remove fungal material directly from affected cavities.
Why many patients will find this interesting: Antifungal treatment can help control chronic pulmonary aspergillosis, but it does not usually remove an established fungal ball. Surgery can sometimes be curative, but many patients are not suitable surgical candidates because of reduced lung function or other medical conditions. A successful bronchoscopic approach could eventually provide an additional option for selected patients.
Why is this important?
Many patients with chronic pulmonary aspergillosis are not suitable candidates for surgery because of reduced lung function or other health problems. A bronchoscopic approach could potentially offer a less invasive alternative in selected cases.
However, several important questions remain unanswered:
- Which patients benefit most?
- How often does the aspergilloma return?
- What is the risk of bleeding?
- Is antifungal treatment still required afterwards?
- How durable are the results over longer follow-up?
At present, this should be viewed as a promising specialist-centre approach rather than a new standard of care.
Evidence strength: Clinical interventional study.
Practice-changing now? No. Potentially important, but not yet routine management.
Bottom line: Bronchoscopic removal of aspergilloma is an interesting specialist approach that may eventually help some patients who are unsuitable for surgery, but it is not yet standard treatment.
Read more:
Investigating the efficacy and safety of bronchoscopic removal of aspergilloma in PTB-CCPA
PCR Testing May Help Diagnose Invasive Aspergillosis
Another paper examined the role of real-time polymerase chain reaction (PCR) testing in diagnosing invasive aspergillosis.
PCR detects fungal genetic material and can potentially identify infection more quickly than conventional culture methods.
Why is this important?
Diagnosing invasive aspergillosis remains challenging. No single test is perfect, and clinicians often need to combine information from:
- CT scans and other imaging
- Bronchoscopy findings
- Fungal culture
- Microscopy
- Galactomannan testing
- Clinical risk factors
PCR has been studied for many years, but its performance varies depending on the patient group, sample type, laboratory method and whether the patient has already received antifungal treatment.
This study supports the growing role of molecular diagnostics but does not suggest that PCR should replace existing tests. Instead, it reinforces the idea that combining several diagnostic approaches usually provides the most reliable diagnosis.
A key caution is that PCR detects fungal DNA. It does not always prove invasive disease. This is especially important in people with structurally abnormal lungs, where colonisation can complicate interpretation.
Evidence strength: Diagnostic utility study.
Practice-changing now? No. PCR may be a useful additional test but should always be interpreted alongside the wider clinical picture.
Bottom line: PCR is becoming an increasingly useful diagnostic tool, but it works best when combined with scans, biomarkers, culture results and clinical assessment.
Read more:
Utility of Real-Time PCR in the Diagnosis of Invasive Aspergillosis
Five Years of Evidence on COVID-19-Associated Pulmonary Aspergillosis
Researchers also published a major umbrella review examining evidence from 2020 to 2025 on COVID-19-associated pulmonary aspergillosis (CAPA).
CAPA emerged during the COVID-19 pandemic as an important complication affecting some patients with severe COVID-19, particularly those requiring intensive care.
What did the review find?
The review confirms that CAPA remains associated with:
- Severe illness
- Intensive care admission
- Mechanical ventilation
- High mortality
However, estimating exactly how common CAPA is remains difficult.
Different studies used different definitions, diagnostic methods and screening approaches, making direct comparison challenging. Bronchoscopy was also limited in many settings early in the pandemic, which affected how cases were detected and classified.
Studies have also differed because of:
- Different diagnostic criteria
- Changes in COVID-19 treatment over time
- Vaccination status
- Use of corticosteroids and immunomodulators
- Different intensive care unit screening practices
The review is valuable because it brings together several years of evidence, but it is unlikely to change current management directly.
Evidence strength: Umbrella review and meta-meta-analysis.
Practice-changing now? No. It reinforces awareness rather than introducing a new treatment approach.
Bottom line: CAPA remains a serious complication of severe COVID-19, but this review largely confirms what clinicians already suspected rather than changing current practice.
Read more:
Incidence, Mortality and Risk Factors in COVID-19-Associated Pulmonary Aspergillosis (CAPA)
Why Azole Tolerance Is More Complex Than Resistance
The most scientifically important theme this week comes from three studies investigating how Aspergillus fumigatus survives exposure to azole antifungal drugs.
For many years, discussions about antifungal treatment failure have focused heavily on resistance mutations, particularly changes involving the CYP51A gene. These mutations can make the fungus less susceptible to antifungal drugs such as itraconazole, voriconazole, posaconazole and isavuconazole.
However, these new studies suggest the situation may be considerably more complicated.
Researchers found that fungal survival may also be influenced by:
- Iron availability
- Mitochondrial function
- Epigenetic regulation
- Long non-coding RNA molecules
Why this matters for patients: Laboratory testing may sometimes suggest that an Aspergillus isolate is susceptible to treatment, yet the infection can still prove difficult to control. Researchers increasingly believe that fungal tolerance and stress-response mechanisms may help explain some of these situations. Understanding these processes could eventually lead to better resistance monitoring and more effective treatments.
Resistance vs Tolerance: What's the Difference?
Resistance and tolerance are related but different concepts.
Resistance usually refers to genetic changes that allow the fungus to continue growing despite exposure to an antifungal drug.
Tolerance refers to the ability of some fungal cells to survive drug exposure without necessarily having permanent resistance mutations.
This distinction matters because tolerance may allow the fungus to persist long enough to eventually acquire more stable resistance.
In simple terms, researchers are increasingly asking whether some cases of treatment failure occur because the fungus first becomes tolerant and only later becomes resistant.
The emerging model:
Azole exposure → Temporary tolerance → Fungal survival → Opportunity for resistance mutations → Stable resistance
Iron Starvation and Azole Tolerance
One study found that iron starvation may increase azole tolerance in Aspergillus fumigatus through effects on mitochondrial function.
Iron is essential for both humans and fungi. During infection, the immune system attempts to limit fungal access to iron as part of a defence strategy known as nutritional immunity.
The study suggests that when iron becomes scarce, the fungus may alter its metabolism in ways that help it survive antifungal stress.
This does not mean that iron supplements or dietary changes would affect antifungal treatment. The work is exploring complex biological processes occurring within infected tissues.
Instead, the study provides another clue about how the fungus adapts to hostile conditions inside the body.
Evidence strength: Mechanistic laboratory research.
Practice-changing now? No.
Epigenetics and the Development of Resistance
Perhaps the most influential paper this week examined an epigenetic mechanism that appears to promote azole tolerance and facilitate the later development of antifungal resistance.
Epigenetics refers to changes in gene activity that occur without altering the underlying DNA sequence itself.
In recent years, researchers have increasingly recognised that fungal adaptation is not driven solely by permanent genetic mutations. Instead, fungi can alter gene activity in response to environmental stress.
This study supports a model in which antifungal exposure may trigger a temporary tolerant state. That tolerant state may then allow some fungal cells to survive long enough to acquire permanent resistance mutations.
Importantly, this does not replace the existing understanding of CYP51A-mediated resistance. Instead, it expands it.
Rather than viewing resistance as a single event, researchers are increasingly seeing it as a process that may develop over time.
Evidence strength: Strong mechanistic evidence.
Practice-changing now? No, but potentially important for future resistance monitoring and antifungal development.
Long Non-Coding RNA and Antifungal Susceptibility
The third paper identified a long non-coding RNA that appears to influence triazole susceptibility in Aspergillus fumigatus.
Long non-coding RNAs are molecules that do not produce proteins themselves but can still influence how genes are switched on or off.
Although these molecules are increasingly recognised as important regulators of biological processes, their role in fungal antifungal susceptibility remains relatively unexplored.
The researchers found that altering the activity of a specific long non-coding RNA changed how the fungus responded to azole antifungal drugs in laboratory experiments and animal models.
This is still early-stage science and has no immediate impact on patient treatment. However, it provides another example of how fungal responses to antifungal drugs may be regulated by multiple biological pathways.
Evidence strength: Moderate to strong mechanistic evidence.
Practice-changing now? No.
Bottom line: These studies suggest that antifungal treatment response is influenced by much more than classic resistance mutations. Scientists are uncovering a complex network of stress responses, metabolic adaptations and gene regulation mechanisms that may help Aspergillus survive antifungal exposure. While this research will not change treatment today, it may eventually lead to better ways of predicting, preventing and overcoming antifungal resistance.
Also Noted This Week
Breakthrough Aspergillosis Despite Prophylaxis
A case report described tracheobronchial aspergillosis developing in a lung transplant recipient despite receiving combined antifungal prophylaxis. The infection involved Aspergillus calidoustus and Aspergillus niger.
While only a single case, it serves as a reminder that prophylactic treatment reduces risk but cannot eliminate it completely, particularly in highly immunosuppressed patients and where less common or resistant Aspergillus species may be involved.
Evidence strength: Case report. Clinically notable, but very low-level evidence.
Practice-changing now? No.
Read more:
View on PubMed |
Read via DOI
Therapeutic Drug Monitoring Remains Important
A bibliometric review highlighted growing interest in antifungal therapeutic drug monitoring (TDM).
Therapeutic drug monitoring means measuring antifungal drug levels in the blood to help ensure that treatment is high enough to be effective while minimising toxicity and drug interactions.
This does not provide new clinical trial evidence, but it supports the growing importance of antifungal stewardship, pharmacokinetic monitoring, toxicity prevention and pharmacy-led optimisation of antifungal treatment.
Evidence strength: Bibliometric and service-focused review.
Practice-changing now? No, but relevant to service development and pharmacy practice.
Read more:
View on PubMed |
Read via DOI
Potential Future Drug Targets
A bioRxiv preprint investigated the mannitol biosynthesis pathway in Aspergillus fumigatus, focusing on mannitol-2-dehydrogenase as a possible antifungal target.
This is early preclinical research and does not affect current treatment. However, it is worth watching as part of wider efforts to identify fungal-specific metabolic vulnerabilities that could eventually support new antifungal strategies.
Evidence strength: Preclinical antifungal-target discovery.
Practice-changing now? No. Interesting, but very early.
Read more:
Search bioRxiv for this preprint
Why This Research Matters
- Diagnosis continues to improve through molecular testing.
- Researchers are exploring less invasive options for managing aspergilloma.
- COVID-19-associated pulmonary aspergillosis remains an important complication of severe COVID-19.
- Scientists are discovering new mechanisms that help Aspergillus survive antifungal treatment.
- Future antifungal therapies may target fungal stress responses as well as traditional resistance mechanisms.
What Researchers Will Be Watching Next
- Whether bronchoscopic aspergilloma removal can be replicated in larger studies and specialist centres.
- How PCR testing can be integrated most effectively into routine diagnostic pathways.
- Whether CAPA rates continue to change as COVID-19 evolves and vaccination remains widespread.
- How fungal tolerance contributes to treatment failure and acquired azole resistance.
- Whether new antifungal drugs can exploit pathways such as mannitol metabolism, stress adaptation and epigenetic regulation.
What This Means for Patients
This week's research illustrates how aspergillosis science is advancing in two important directions at the same time.
Firstly, researchers are developing better ways to diagnose and manage disease through improved testing and new interventional approaches.
Secondly, scientists are learning much more about the biology of Aspergillus itself, particularly how it survives antifungal treatment and adapts to stressful environments.
Although none of these studies should change individual treatment decisions today, they contribute to a growing body of knowledge that may improve diagnosis, monitoring and treatment options in the future.
The most immediate clinical relevance comes from studies investigating diagnosis and management. The laboratory studies are less likely to affect care in the short term but may contribute to future advances in treatment and resistance prevention.
For now, the main message is that aspergillosis remains a complex condition that requires specialist assessment and interpretation of test results within the wider clinical picture.
None of the papers discussed in this update support changing treatment without specialist medical advice.
When to Speak to Your Clinical Team
Contact your clinical team promptly if you experience:
- Significant haemoptysis (coughing up blood)
- Worsening breathlessness
- Persistent fever
- New or worsening chest pain
- Severe side effects from antifungal treatment
- New confusion or sudden deterioration
- A sudden worsening of your usual aspergillosis symptoms
Do not stop, reduce, or change antifungal treatment without discussing it with your healthcare team first.
If you cough up a large amount of blood, have severe breathlessness, chest pain, collapse, or feel acutely unwell, seek urgent medical help.
Evidence Strength Summary
| Topic | Evidence type | Clinical relevance | Practice-changing now? |
|---|---|---|---|
| Bronchoscopic aspergilloma removal in post-tuberculosis CPA | Clinical interventional study | Medium to high | No |
| Real-time PCR for invasive aspergillosis | Diagnostic utility study | Moderate | No |
| CAPA umbrella review | Evidence synthesis | High | No |
| Iron starvation and azole tolerance | Mechanistic study | Medium | No |
| Epigenetic azole tolerance | Mechanistic study | Medium to high | No |
| Long non-coding RNA and triazole susceptibility | Mechanistic study | Medium | No |
| Breakthrough tracheobronchial aspergillosis case report | Case report | Low to moderate | No |
| Antifungal therapeutic drug monitoring | Bibliometric/service review | Moderate for services | No |
| Mannitol pathway preprint | Preclinical target discovery | Low at present | No |
Frequently Asked Questions
What is azole tolerance in Aspergillus?
Azole tolerance describes the ability of some Aspergillus cells to survive exposure to antifungal drugs without possessing the classic resistance mutations normally associated with azole resistance. Researchers believe tolerance may sometimes contribute to persistent infection and could provide an opportunity for more stable resistance to develop later.
Can PCR diagnose aspergillosis?
Polymerase chain reaction (PCR) testing can help detect Aspergillus genetic material and may support diagnosis, particularly when combined with imaging, culture, galactomannan testing and clinical assessment. PCR alone cannot confirm invasive disease.
What is COVID-19-associated pulmonary aspergillosis (CAPA)?
COVID-19-associated pulmonary aspergillosis, or CAPA, is a form of aspergillosis that can occur in some patients with severe COVID-19, particularly those requiring intensive care treatment.
Can aspergilloma be removed without surgery?
Research is exploring bronchoscopic removal of aspergilloma in carefully selected patients. However, this remains a specialist procedure and is not currently considered standard treatment. Further studies are needed to determine which patients benefit most.
Does antifungal resistance mean treatment will stop working?
Not necessarily. Many patients respond well to antifungal treatment. Resistance is only one factor influencing treatment success. Drug levels, immune function, disease severity and fungal tolerance mechanisms may also influence outcomes.
Should I change my antifungal treatment because of these studies?
No. None of the studies discussed in this update support changing treatment without specialist medical advice. Patients should always discuss treatment decisions with their clinical team.
Electric Fans in Hot Weather: Helpful or Harmful?
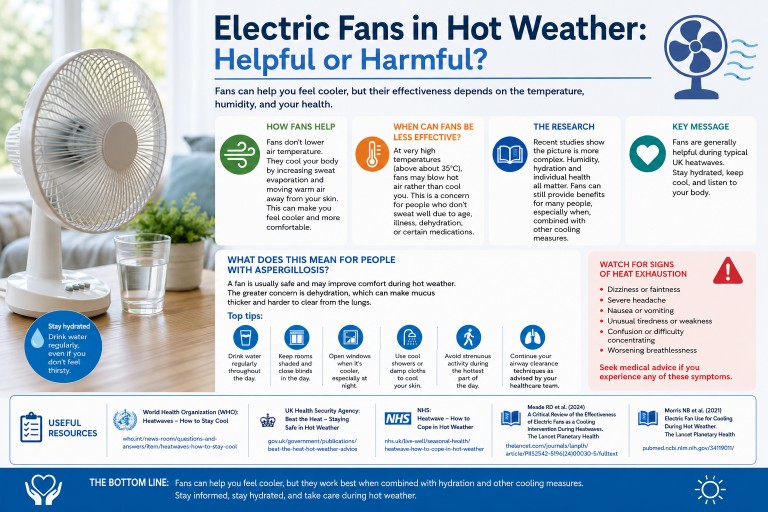
As temperatures rise across the UK, many people reach for an electric fan to stay cool. However, you may have seen advice suggesting that fans should be used with caution during very hot weather. Why is that, and what does it mean for people living with aspergillosis and other chronic lung conditions?
Key Points
- Electric fans can help most people stay comfortable during UK heatwaves.
- Fans cool the body by increasing the evaporation of sweat.
- In extreme heat (above about 35°C), fans may become less effective for some people.
- Hydration remains one of the most important ways to protect yourself during hot weather.
- People with chronic lung conditions should pay particular attention to avoiding dehydration, which can make mucus thicker and harder to clear.
How do electric fans cool us?
Electric fans do not lower the temperature of the air. Instead, they move air across the skin, helping sweat evaporate more quickly. Because evaporation removes heat from the body, this can make you feel cooler and more comfortable.
For most people, particularly during typical UK summer temperatures, fans are a useful and inexpensive way to reduce discomfort during hot weather.
Why is there advice to limit fan use in extreme heat?
Some public health guidance advises caution when temperatures rise above about 35°C. At these temperatures, a fan may simply blow very hot air across the body. If a person is unable to sweat effectively because of age, illness, dehydration, or certain medications, the cooling benefit may be reduced.
This concern led organisations such as the NHS, UK Health Security Agency (UKHSA), and World Health Organization (WHO) to recommend that fans should not be relied upon as the only cooling strategy during extreme heat.
However, research over the last few years has shown that the situation is more complicated than a simple temperature cut-off. Factors such as humidity, hydration, age, and overall health all influence whether a fan is helpful.
What does the research say?
Recent studies suggest that electric fans may still provide benefits for many people, even when temperatures exceed 35°C, particularly if humidity levels are high and the body is able to sweat normally.
Researchers now recognise that there is no single temperature at which fans suddenly become harmful. Instead, their effectiveness depends on the balance between heat gained from the surrounding air and heat lost through sweat evaporation.
The overall message from researchers and public health organisations is that fans remain useful for many people but should be combined with other cooling measures such as drinking fluids, seeking shade, and cooling the skin with water.
What does this mean for people with aspergillosis?
For people living with aspergillosis, asthma, chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), or bronchiectasis, a fan is generally safe and may improve comfort during hot weather.
The greater concern is often dehydration. Hot weather can lead to fluid loss through sweating, which may cause mucus and sputum to become thicker and more difficult to clear from the lungs. This can increase coughing, breathlessness, and discomfort.
If you use a fan during hot weather:
- Drink water regularly throughout the day.
- Keep curtains or blinds closed on sun-facing windows.
- Open windows when outdoor temperatures are cooler, particularly overnight.
- Use cool showers, damp cloths, or a spray bottle to cool the skin.
- Avoid strenuous activity during the hottest part of the day.
- Continue any airway clearance techniques recommended by your healthcare team.
Watch for signs of heat exhaustion
Seek medical advice if you experience:
- Dizziness or fainting
- Severe headache
- Nausea or vomiting
- Excessive tiredness or weakness
- Confusion or difficulty concentrating
- Worsening breathlessness
The bottom line
For most people in the UK, electric fans remain a helpful way to stay comfortable during hot weather. Current evidence suggests that fans are generally beneficial during typical UK heatwaves, especially when used alongside other cooling measures.
The most important message for people with chronic lung conditions is to stay hydrated. Fans can help you feel cooler, but drinking enough fluids, avoiding overheating, and recognising the signs of heat-related illness are equally important.
Further Reading
- World Health Organization (WHO): Heatwaves – How to Stay Cool
- UK Health Security Agency (UKHSA): Beat the Heat – Staying Safe in Hot Weather
- NHS: Heatwave – How to Cope in Hot Weather
- Meade RD et al. A Critical Review of the Effectiveness of Electric Fans as a Cooling Intervention During Heatwaves. Lancet Planetary Health.
- Morris NB et al. Electric Fan Use for Cooling During Hot Weather. Lancet Planetary Health.
Further Reading
- World Health Organization (WHO): Heatwaves – How to Stay Cool
- UK Health Security Agency (UKHSA): Beat the Heat – Staying Safe in Hot Weather
- NHS: Heatwave – How to Cope in Hot Weather
- Meade RD et al. A Critical Review of the Effectiveness of Electric Fans as a Cooling Intervention During Heatwaves. The Lancet Planetary Health (2024)
- Morris NB et al. Electric Fan Use for Cooling During Hot Weather. The Lancet Planetary Health (2021)
Author: National Aspergillosis Centre Team
Reviewed: June 2026
Next Review: June 2027
This article is intended for educational purposes and should not replace advice from your healthcare team.
Hot Weather Advice for People Living with Aspergillosis
Key Points
- Hot weather can worsen breathlessness, fatigue and sleep quality.
- Dehydration can make mucus thicker and more difficult to clear.
- People with asthma, bronchiectasis, Chronic Pulmonary Aspergillosis (CPA) and Allergic Bronchopulmonary Aspergillosis (ABPA) may notice increased symptoms during heatwaves.
- Stay hydrated, keep cool and avoid strenuous activity during the hottest part of the day.
- Some antifungal medications can increase sensitivity to sunlight.
- Seek medical advice if symptoms worsen significantly or you develop signs of heat-related illness.
Can Hot Weather Make Aspergillosis Worse?
Yes. Hot weather can worsen symptoms for some people living with aspergillosis.
Heat can increase breathlessness, contribute to dehydration, make mucus thicker
and harder to clear, disturb sleep, and increase fatigue.
People with Chronic Pulmonary Aspergillosis (CPA), Allergic Bronchopulmonary
Aspergillosis (ABPA), bronchiectasis, asthma, or adrenal insufficiency may need
to take extra precautions during heatwaves.
Why Heat Can Affect Breathing
When temperatures rise, the body works harder to keep cool. This increases demand
on the heart and lungs and can make breathing feel more difficult.
- Increased breathing rate
- Worsening breathlessness
- Increased fatigue
- More difficult airway clearance
- Poorer sleep
- Reduced exercise tolerance
Stay Well Hydrated
Good hydration is one of the most important steps you can take during hot weather.
Dehydration can make sputum thicker and harder to clear, particularly for people
with bronchiectasis or Chronic Pulmonary Aspergillosis (CPA).
- Drink regularly throughout the day.
- Carry water when travelling.
- Increase fluid intake if sweating heavily.
- Avoid waiting until you feel thirsty before drinking.
Signs of dehydration may include:
- Dark urine
- Dizziness or light-headedness
- Headache
- Dry mouth
- Increased fatigue
- Thick, sticky sputum
If you have heart failure, severe kidney disease or have been advised to restrict
fluids, follow the guidance provided by your healthcare team.
Keep Your Home Cool
- Close curtains and blinds during the day.
- Open windows overnight when temperatures fall.
- Use fans to improve airflow.
- Spend time in the coolest room of the house.
- Avoid ovens and other heat-producing appliances during the hottest periods.
Plan Activities Carefully
Try to avoid strenuous activity between approximately 11am and 4pm when
temperatures are highest.
- Walk early in the morning or later in the evening.
- Take frequent breaks.
- Pace yourself.
- Ask for help with physically demanding tasks during the hottest days.
Medication Considerations
Inhalers
Continue taking inhalers exactly as prescribed. Carry reliever inhalers when away
from home and avoid leaving inhalers in hot cars or direct sunlight.
Antifungal Medicines and Sunlight
Some antifungal medicines can increase sensitivity to sunlight. This is
particularly important for people taking voriconazole.
- Use high-factor sunscreen.
- Wear a hat and protective clothing.
- Avoid prolonged exposure to direct sunlight.
- Report new or changing skin lesions to your healthcare team.
Adrenal Insufficiency
People with adrenal insufficiency may be more vulnerable to dehydration, low blood
pressure and heat-related illness.
- Maintain good hydration.
- Carry steroid emergency information.
- Follow sick-day guidance if you become unwell.
- Seek urgent medical advice if you cannot keep fluids or medication down.
Air Quality Matters Too
Hot weather is often associated with increased pollen levels, elevated ozone
pollution, wildfire smoke or other poor air-quality episodes. These can aggravate
asthma, bronchiectasis and aspergillosis-related respiratory symptoms.
- Check local air-quality forecasts if symptoms worsen.
- Consider staying indoors during peak pollution periods.
- Keep rescue medication available.
Protect Your Sleep
- Use lightweight bedding.
- Close curtains during the day.
- Use a fan at night if helpful.
- Keep water nearby.
- Cool wrists or feet with cool water before bed.
When to Seek Medical Advice
Do not assume that worsening symptoms are always caused by the heat. Seek medical
advice if you experience:
- Markedly worsening breathlessness
- New chest pain
- A significant fall in oxygen saturation, if monitored
- Confusion or fainting
- High fever
- Inability to clear sputum
- Severe weakness
- Vomiting or inability to keep fluids down
Seek urgent medical attention for severe breathing difficulties, collapse, or
signs of heatstroke.
Hot Weather Checklist
- Drink regularly throughout the day.
- Keep cool indoors.
- Avoid strenuous activity during peak heat.
- Monitor breathlessness and sputum changes.
- Continue medicines as prescribed.
- Protect your skin if taking voriconazole.
- Check air-quality forecasts.
- Keep bedrooms cool.
- Seek medical advice if symptoms worsen unexpectedly.
Further Information and Trusted Resources
General Hot Weather Advice
- NHS: How to cope in hot weather
- NHS: Heat exhaustion and heatstroke
- UK Health Security Agency: Beat the Heat
- UKHSA Heat Health Alerts
Related Aspergillosis.org Resources
- Living Well with Aspergillosis
- Managing Breathlessness
- Bronchiectasis and Aspergillosis
- Air Pollution and Lung Health
- Travelling with Aspergillosis
- Exercise, Fatigue and Energy Management
- Adrenal Insufficiency and Steroid Treatment
Frequently Asked Questions
Can hot weather make aspergillosis symptoms worse?
Yes. Heat can worsen breathlessness, fatigue, dehydration and sleep quality, all
of which may make symptoms feel more severe.
Why is hydration so important?
Dehydration can make mucus thicker and more difficult to clear, potentially
worsening cough and breathlessness.
Does hot weather affect Allergic Bronchopulmonary Aspergillosis (ABPA)?
Some people with Allergic Bronchopulmonary Aspergillosis (ABPA) find that heat,
pollen and poor air quality can aggravate asthma symptoms and increase
breathlessness.
Does hot weather affect Chronic Pulmonary Aspergillosis (CPA)?
People with Chronic Pulmonary Aspergillosis (CPA) may notice increased fatigue,
breathlessness and difficulty clearing sputum during hot weather, particularly if
they become dehydrated.
Should I avoid going outside?
Not necessarily. However, avoiding strenuous activity during the hottest part of
the day is often sensible, especially if you have significant lung disease.
What if I take voriconazole?
Voriconazole can increase sensitivity to sunlight. Extra sun protection is
recommended during hot weather.
When to Seek Medical Help
Contact your healthcare team if you experience worsening respiratory symptoms,
increasing fatigue, difficulty clearing sputum, or concerns about dehydration.
Seek urgent medical attention for severe breathing difficulties, collapse,
confusion, or suspected heatstroke.
Author: National Aspergillosis Centre (NAC)
Last reviewed: June 2026
Next review: June 2027
Has My Omalizumab Stopped Working? Understanding Worsening Symptoms, Infections and Flare-Ups in Asthma and ABPA
Last reviewed: June 2026
Key Points
- Omalizumab can remain effective for many years.
- Worsening symptoms do not automatically mean the treatment has stopped working.
- Increasing chest infections may be caused by bronchiectasis, bacterial infection, mucus plugging or another lung condition.
- Asthma and Allergic Bronchopulmonary Aspergillosis (ABPA) can change over time.
- Biologics are usually one part of a wider treatment plan and do not replace inhalers, airway clearance or routine monitoring.
- A specialist review may include blood tests, sputum cultures, lung function tests and CT imaging.
Contents
- Why patients ask this question
- What is omalizumab?
- Does omalizumab wear off?
- Why symptoms may worsen after years of treatment
- What else could be going on?
- Possible reasons for worsening symptoms
- The role of bronchiectasis and infection
- Don't forget the basics
- What tests might help?
- Questions to ask your specialist
- Frequently asked questions
- When to seek medical advice
- The bottom line
Why Patients Ask This Question
Many people living with severe asthma or Allergic Bronchopulmonary Aspergillosis (ABPA) experience major improvements after starting omalizumab. They may have fewer flare-ups, require fewer courses of oral steroids and enjoy a much better quality of life.
However, some patients notice that after several years they begin needing more antibiotics, more steroid courses or more medical reviews. Symptoms such as cough, sputum production, wheeze or breathlessness may start to increase again.
This often leads to a worrying question:
"Has my biologic stopped working?"
In reality, the answer is often more complicated than a simple yes or no.
What Is Omalizumab?
Omalizumab (Xolair®) is a biologic medication that targets immunoglobulin E (IgE), an antibody involved in allergic inflammation.
It is commonly used to treat severe allergic asthma and is also used in some patients with ABPA where allergic inflammation is an important part of the disease.
By reducing IgE activity, omalizumab can help reduce asthma exacerbations, improve symptom control and reduce the need for oral corticosteroids in many patients.
Does Omalizumab Wear Off?
Current evidence suggests that omalizumab can remain effective for many years. Studies following patients with severe allergic asthma have shown sustained benefits in many people over five years or more.
There is currently no strong evidence that most patients develop predictable tolerance to omalizumab simply because they have been taking it for a long time.
This means that if symptoms worsen after four, five or more years of treatment, specialists will usually look for other explanations before concluding that the medication has stopped working.
Why Symptoms May Worsen After Years of Treatment
There are several reasons why symptoms may worsen despite ongoing biologic treatment.
Lung Damage Can Continue to Cause Problems
Many patients with ABPA also have bronchiectasis. Bronchiectasis is permanent widening and damage of the airways that can develop after repeated inflammation and infection.
Even when allergic inflammation is well controlled, bronchiectasis can still cause:
- Persistent cough
- Sputum production
- Breathlessness
- Fatigue
- Recurrent chest infections
In these situations, the biologic may still be helping while another aspect of the lung disease becomes more important.
Infection May Become More Important
Patients with bronchiectasis are more vulnerable to chest infections. Symptoms caused by infection can sometimes look very similar to an asthma or ABPA flare.
Signs suggesting infection may include:
- Increased sputum production
- Darker or thicker sputum
- Fever
- Feeling generally unwell
- More frequent need for antibiotics
Asthma and ABPA Can Change Over Time
Asthma is not a single disease. The pattern of inflammation in the airways may change over time.
Some patients who initially respond very well to anti-IgE treatment may later develop different patterns of airway inflammation, mucus production or airway remodelling.
This is one reason why specialists sometimes review whether a different biologic may be appropriate.
What Else Could Be Going On?
When symptoms worsen after several years of successful biologic treatment, specialists often look beyond asthma and ABPA alone.
Several different conditions can cause cough, breathlessness, sputum production, fatigue and recurrent chest infections.
Bronchiectasis Progression
Even if allergic inflammation is well controlled, bronchiectasis can continue to cause mucus retention, recurrent infections and worsening respiratory symptoms.
Bacterial Infection
Repeated chest infections can become a major cause of symptoms. Common bacteria include:
- Pseudomonas aeruginosa
- Haemophilus influenzae
- Staphylococcus aureus
- Moraxella catarrhalis
Mucus Plugging
Thick mucus can block airways, causing cough, breathlessness and reduced airflow.
Aspergillus Bronchitis
Some patients develop persistent airway infection with Aspergillus species. Symptoms may include chronic productive cough, increased sputum and recurrent respiratory symptoms.
Chronic Pulmonary Aspergillosis (CPA)
Although less common, some patients with previous lung damage may develop chronic pulmonary aspergillosis. Symptoms can include fatigue, weight loss, chronic cough and sometimes coughing up blood.
Nontuberculous Mycobacterial (NTM) Infection
Patients with bronchiectasis may be at increased risk of infection caused by environmental mycobacteria.
Changing Asthma Biology
The type of airway inflammation present when treatment begins may change over time.
The important point is that worsening symptoms do not automatically mean that omalizumab has stopped working.
Several different conditions may produce similar symptoms and require different treatments.
Possible Reasons for Worsening Symptoms
| Possible Cause | Typical Clues |
|---|---|
| ABPA flare | Increasing asthma symptoms, rising IgE, worsening inflammation |
| Bronchiectasis progression | More sputum, recurrent infections, increasing need for airway clearance |
| Bacterial infection | Change in sputum colour, fever, feeling unwell, antibiotics helping |
| Mucus plugging | Sudden worsening breathlessness, blocked airways |
| Aspergillus bronchitis | Persistent productive cough and sputum despite standard treatment |
| Chronic Pulmonary Aspergillosis (CPA) | Weight loss, fatigue, chronic symptoms, coughing up blood |
| NTM infection | Gradual worsening symptoms despite repeated treatment courses |
The Role of Bronchiectasis and Infection
For many patients with ABPA, the most useful question is not:
"Has omalizumab stopped working?"
but rather:
"What is causing my recent increase in symptoms and infections?"
If the main change is increasing antibiotic use, sputum production or recurrent chest infections, the focus may need to shift towards understanding what is happening within the airways.
This may include reviewing sputum cultures, airway clearance techniques, physiotherapy, exercise levels and bronchiectasis management plans.
Don't Forget the Basics
One of the challenges of successful biologic treatment is that patients often feel so much better that other aspects of their disease can gradually receive less attention.
This is completely understandable. When symptoms improve, it is natural to focus less on daily disease management.
However, biologics such as omalizumab do not cure asthma, bronchiectasis or ABPA. They help control specific parts of these conditions.
For example, omalizumab may reduce allergic inflammation and asthma exacerbations, but it does not reverse existing bronchiectasis, remove mucus from the airways or prevent every chest infection.
Think of your lung health as a garden. Omalizumab may be very effective at controlling one type of weed, but the garden still needs regular maintenance. If that maintenance stops, other problems can gradually take over.
Continuing to Manage Your Lung Health
- Take prescribed inhalers regularly.
- Continue airway clearance techniques if recommended.
- Stay physically active within your abilities.
- Monitor changes in sputum volume, colour or thickness.
- Attend routine specialist reviews.
- Keep vaccinations up to date.
- Follow asthma and bronchiectasis action plans where provided.
- Report increasing breathlessness, cough or infections promptly.
Biologics can be highly effective, but they work best as part of a broader management plan rather than replacing it.
The Bottom Line
If symptoms worsen after several years on omalizumab, it does not automatically mean the medication has stopped working.
In patients with asthma and ABPA, increasing antibiotics and steroid use may reflect changing asthma control, ABPA activity, bronchiectasis-related infection, mucus plugging or another lung condition.
Successful biologic treatment can sometimes make it easy to forget that asthma, bronchiectasis and ABPA still require ongoing management. Continuing inhalers, airway clearance, exercise, monitoring and regular review remains important even when symptoms have improved.
A careful specialist review can often identify what has changed and guide the most appropriate next steps.