
Wildfire smoke and aspergillosis: protecting your lungs when air quality falls
Wildfires in parts of the UK and Europe can produce smoke that travels considerable distances. Even when a fire is many miles away, fine particles carried in the air may temporarily reduce local air quality.
People with aspergillosis, asthma, bronchiectasis, COPD or another chronic lung condition may be more sensitive to wildfire smoke. Smoke can irritate the airways and cause coughing, wheezing, chest tightness, breathlessness, sore eyes or a sore throat. It can also aggravate an existing respiratory condition.
Check the air quality where you live. UK residents can use the official Defra UK Air website. International websites such as IQAir can also provide useful local maps, forecasts and measurements.
What should people with lung conditions do?
UK health advice recommends reducing exposure to smoke and air pollution, particularly if you develop symptoms.
- Reduce strenuous outdoor activity. Exercise causes you to breathe more deeply and may increase the amount of smoke particles reaching your lungs.
- Stay indoors when smoke is affecting your area and keep doors and windows closed while the outdoor air quality is poor.
- Ventilate when conditions improve. Open windows when the smoke has cleared and outdoor air quality is better, particularly if the building is becoming hot.
- Take your usual medication as prescribed. Do not alter antifungal treatment, inhalers, steroids or other medicines unless advised by your healthcare team.
- Keep your reliever inhaler with you if one has been prescribed.
- Follow your asthma, COPD, bronchiectasis or respiratory action plan if you have one.
- Avoid adding more particles indoors. During a smoke episode, avoid smoking, wood-burning stoves, candles and other activities that create smoke.
- Keep cool and hydrated. Wildfires often occur during hot weather, which can place additional strain on people with heart, lung, kidney or other long-term conditions.
Do masks help?
A well-fitting particulate respirator such as an FFP2 or FFP3 mask may reduce the amount of fine particulate matter inhaled while outdoors. Loose-fitting surgical or fabric masks provide much less protection against fine smoke particles.
However, some people with significant lung disease may find tight-fitting masks uncomfortable or may become more breathless while wearing one. A mask should not be used as a reason to remain outdoors in heavy smoke. Reducing exposure remains the priority.
Does wildfire smoke increase Aspergillus infection?
Wildfire smoke is primarily a mixture of gases and very small particles produced by burning vegetation and other materials. Its immediate health effect is irritation and inflammation of the lungs and airways.
Smoke exposure does not necessarily mean that Aspergillus is growing in the lungs or that aspergillosis is worsening. However, people whose lungs are already damaged or inflamed may notice increased coughing, wheezing, mucus production or breathlessness.
Symptoms caused by smoke can resemble a respiratory flare-up. Contact your healthcare team if symptoms are new, unusually severe, persist after the air quality has improved, or are not controlled by your normal treatment plan.
When should you seek medical help?
Contact your GP, respiratory team or NHS 111 if:
- you develop new or worsening breathlessness, wheezing or chest tightness;
- you need your reliever inhaler more often than usual;
- your symptoms are not responding to your agreed treatment plan;
- your symptoms persist after the smoke has cleared; or
- you are concerned about a change in your condition.
Call 999 for severe breathing difficulty. This includes rapidly worsening breathlessness, being unable to speak normally, becoming confused or drowsy, developing blue or grey lips or skin, or an asthma attack that is not improving after using your reliever inhaler as directed.
Understanding air-quality alerts
The UK Daily Air Quality Index runs from 1 to 10:
- Low, 1–3: most people can continue normal outdoor activity.
- Moderate, 4–6: people with lung or heart conditions who develop symptoms should reduce strenuous outdoor activity.
- High, 7–9: people with lung conditions should reduce strenuous outdoor exertion, particularly if symptomatic.
- Very high, 10: people with lung or heart conditions and older adults should avoid strenuous physical activity.
People vary considerably in their sensitivity. Some people with severe asthma, bronchiectasis or aspergillosis may experience symptoms even when the overall air-quality rating is described as low or moderate. Your symptoms and personal respiratory action plan remain important.
Useful sources
- Defra UK Air: current air-quality measurements and alerts
- UK government health advice for the Daily Air Quality Index
- IQAir international air-quality map
- NHS advice about asthma and asthma attacks
This information is intended as general guidance and does not replace advice from your own healthcare team.

Learning to Live with Chronic Illness: Is It Really Like Grieving?
“How do you accept having a chronic illness? Is it a grieving process?”
It is one of the most thoughtful questions anyone living with a long-term health condition can ask.
Whether you have aspergillosis, bronchiectasis, severe asthma, COPD or another chronic illness, many people describe life as having two chapters: before illness and after illness.
Most of us grow up assuming our health will simply be there in the background. We make plans, book holidays, think about retirement, imagine spending time with grandchildren, travelling or enjoying hobbies. We rarely question whether our bodies will allow us to do these things.
Then, sometimes quite suddenly, life changes.
Perhaps the diagnosis follows weeks of investigations. Perhaps it comes after years of unexplained symptoms, repeated infections or unsuccessful treatments. Whatever the route, many people describe the feeling that the future they expected has quietly disappeared.
The physical symptoms may be obvious.
The emotional changes are often much harder to see.
That is why so many people describe living with chronic illness as a form of grief.
Grieving for the life you expected
When we hear the word grief, we usually think about losing someone we love.
However, grief can follow many different kinds of loss. A chronic illness may bring several losses, not necessarily all at once, but gradually over time.
You may grieve:
- the health you once took for granted
- your confidence in your body
- your independence or spontaneity
- work or career opportunities
- financial security
- hobbies and activities that have become more difficult
- changes in relationships or family roles
- the future you had imagined.
Perhaps you can no longer walk as far as you once did. Perhaps you worry about booking a holiday because you do not know how you will feel when the time comes. Perhaps you miss being the person everyone relied upon.
You may also miss the freedom of doing something without first considering your symptoms, medication, energy levels or access to healthcare.
These are genuine losses, even when nobody else can see them.
It is therefore entirely understandable that they may be accompanied by sadness, frustration, anger or fear.
The hidden or “side” griefs
One patient described something that many people immediately recognised: the “side griefs”.
These are the numerous, seemingly small losses that accompany chronic illness. Individually, they may not appear life-changing. Together, they can gradually reshape everyday life.
Perhaps you stop gardening because your breathing or energy will not allow it.
Perhaps you can no longer play with your grandchildren in the same way.
Perhaps you avoid crowded places because you are concerned about infection.
Perhaps you have become the person who always has to ask, “How far is the walk?” or “Will there be somewhere to sit?”
Perhaps an invitation that once brought excitement now brings several calculations: How will I travel? Will I have enough energy? What happens if I become unwell? Can I cancel at short notice?
None of these changes may appear dramatic to other people. Together, however, they can change how you see yourself and the life you live.
“Shouldn’t I be over this by now?”
Many people feel guilty about continuing to struggle emotionally after their diagnosis.
Friends and relatives may say:
“At least it is being treated.”
“You look well.”
“Try to stay positive.”
These comments are usually intended to be reassuring. However, living with a chronic illness is not simply about receiving treatment and then carrying on as before. It frequently requires further practical and emotional adjustment.
Some days that adjustment feels manageable. Other days it feels exhausting.
There is no correct timetable for coming to terms with a life-changing diagnosis.
Is there really a grieving process?
You may have heard of the “five stages of grief”: denial, anger, bargaining, depression and acceptance.
These ideas have helped many people put words around difficult emotions, but real life is rarely so orderly. People do not necessarily move neatly from one stage to the next, and not everyone experiences all of them.
You might feel angry when you are first diagnosed and then optimistic when treatment begins. You may feel settled for several months, only to become frightened again before a scan or clinic appointment.
A flare-up, hospital admission or change in treatment may bring back feelings you thought you had already dealt with.
This does not mean that you are going backwards.
It means you are responding to a changing situation.
Research into psychological adjustment to chronic disease suggests that people differ greatly in how they respond and that adjustment can vary across the course of an illness. There is no single emotional pathway that everyone must follow.
The emotional rollercoaster
Many people imagine that accepting a diagnosis is something that happens once.
Patients often describe something very different.
Living with chronic illness can feel like an emotional rollercoaster.
Good clinic appointments may be followed by disappointing ones.
One blood test brings relief. The next raises new questions.
A scan may show improvement, only for a new symptom to appear.
A treatment begins to work, but later causes side effects or needs to be changed.
One day you almost forget that you are ill. The next day, getting dressed may feel like hard work.
Hope and disappointment.
Confidence and uncertainty.
Good days and bad days.
This continual movement can be exhausting. Just as you begin to feel that life is becoming predictable again, something changes.
Many people say that they are emotionally tired as well as physically tired.
Good days and bad days
Good and bad days can affect how you understand your illness.
On a good day, you may wonder whether you have been too cautious or whether things are finally returning to normal.
On a bad day, you may fear that your illness is getting worse or that the improvement was never real.
Both reactions are understandable, but one day rarely tells the whole story.
Over time, many people learn to look for patterns over weeks or months rather than judging their health by one particularly good or difficult day.
A bad day does not necessarily mean that your condition is deteriorating.
A good day does not mean that the illness has disappeared.
One of the hardest skills is learning to enjoy a good day without spending it worrying about the next bad one. Another is remembering during a difficult day that how you feel today may not be how you feel tomorrow.
You do not adapt once
Perhaps the biggest misconception about chronic illness is that acceptance is a single event.
In reality, most people do not adapt once.
They adapt hundreds of times.
You adapt to the diagnosis.
Then to the first treatment.
Then to side effects.
Then to improvement.
Then to a setback.
You adapt to hospital appointments, new symptoms, reassuring results and worrying results.
You adapt to holidays that have to be cancelled and holidays that go better than expected.
You adapt to asking for help when you were previously independent and to saying no when you would once have said yes.
Every change asks you to adjust again.
This does not mean that you have failed to accept your illness. It reflects the reality of living with a condition that can fluctuate and change over time.
Acceptance is dynamic
Perhaps we should stop thinking of acceptance as something we either achieve or fail to achieve.
Acceptance is dynamic.
It changes as your illness changes, as treatments change and as life itself changes around you.
Every new situation may require another adjustment.
Acceptance is not a finish line. It is an ongoing process of recognising where you are now, adjusting your expectations and protecting the things that remain important to you.
Acceptance does not mean giving up.
It does not mean liking what has happened, pretending everything is fine or abandoning hope for better treatment.
It means recognising the reality of today without spending all your energy fighting the fact that the illness exists.
Many people describe a gradual shift. Instead of repeatedly asking:
“Why has this happened to me?”
they begin to ask:
“Given where I am today, how can I live as well as possible?”
The first question is entirely understandable, but it may never have a satisfying answer. The second may create choices, even when those choices are limited.
Not every day has to be positive
People living with chronic illness are often encouraged to “stay positive”.
The intention is usually kind. Sometimes, however, it can feel like another burden.
The reality is that some days are simply difficult.
You do not have to find a positive lesson in every setback.
You do not have to feel grateful every day.
You do not have to pretend that losing something important does not hurt.
Sometimes the healthiest response is simply to acknowledge:
“Today is hard.”
Tomorrow may be different.
When illness affects the whole family
Chronic illness rarely affects only the person who has been diagnosed.
Partners, children, relatives, friends and carers may also live with uncertainty, disrupted plans, additional responsibilities and concerns about the future.
A partner may not know whether to encourage activity or suggest rest. A relative may struggle to understand why someone can manage an outing one day but has to cancel plans the next. A carer may be carrying practical responsibilities while also trying to manage their own emotions.
Because symptoms fluctuate, family members may sometimes misread what is happening.
On a good day, they may assume that the illness is improving permanently. On a bad day, they may wonder why everything has suddenly changed again.
The person who is ill may then feel disbelieved, pressured or guilty. The family member may feel rejected, confused or unappreciated.
Nobody necessarily intends to hurt anyone, but frustration on both sides can make an already difficult situation feel worse.
Patients may feel guilty about cancelling plans, needing help or placing additional demands on those around them. Carers may feel guilty for becoming tired, impatient or resentful.
These feelings do not mean that anyone cares less. They usually mean that everyone is trying to adapt to a situation they did not choose.
Open communication can help. It may be useful to explain that symptoms fluctuate, that a good day does not mean the illness has disappeared, and that a cancelled plan is not a rejection.
It is equally important for carers and relatives to be honest about their own limits and to have time, support and interests that do not revolve entirely around illness.
Sometimes the most useful conversation is not about solving the problem. It is simply acknowledging:
“This is difficult for both of us, and neither of us is to blame.”
Both the person living with illness and the people supporting them may have to adapt hundreds of times. Doing that together requires patience, honesty and permission for everyone involved to have difficult days.
Families and friends supporting someone with chronic pulmonary aspergillosis may also find our guide to CPA for family and friends helpful.
Living with uncertainty
One of the hardest parts of chronic illness is often uncertainty.
You may not know how well a treatment will work, whether symptoms will improve or how much energy you will have tomorrow.
This unpredictability can make planning difficult. It may also make you feel that you cannot entirely trust your body.
Some people respond by constantly watching for symptoms or imagining everything that might go wrong. This is understandable, particularly after frightening experiences, but remaining permanently on alert can itself become exhausting.
Acceptance does not remove uncertainty. It can, however, help you concentrate more of your attention on what is happening today rather than trying to solve every possible version of the future.
The NHS guide to coping with change and uncertainty offers practical suggestions for focusing on the short term, recognising what is working and finding a new rhythm.
What helps people adapt?
There is no single method that works for everybody. However, research and the experiences of people living with chronic illness suggest that several things can help.
Understanding your condition
Reliable information can reduce some of the fear created by uncertainty. Understanding your condition, treatment and warning signs can help you feel more prepared and involved in decisions about your care.
At the same time, it is possible to become overwhelmed by searching for information. It may help to use a small number of trusted sources and discuss important questions with your healthcare team.
Managing energy rather than fighting it
Fatigue is not simply ordinary tiredness. It can affect concentration, confidence, relationships and emotional wellbeing as well as physical activity.
Learning to pace activity, prioritise important tasks and allow time for recovery is not laziness or surrender. It is a practical response to limited energy.
Our guide to managing fatigue and energy in aspergillosis and allergic fungal lung disease explains pacing, the “boom-and-bust” cycle and ways to use limited energy more effectively.
Talking honestly
Family and friends may want to help but may not understand what you need. They may see you on a relatively good day and assume that your illness has improved.
It can help to explain that symptoms fluctuate and that cancelling a plan does not mean you no longer care about the people involved.
You do not have to tell everyone everything. However, being honest with a few trusted people can reduce the effort involved in constantly pretending to be well.
Connecting with people who understand
Support from other patients can provide something that even loving relatives and skilled healthcare professionals may not always be able to offer: recognition from someone who has experienced something similar.
People may exchange practical ideas, but sometimes the most important benefit is simply hearing:
“I understand. I have felt that too.”
Our aspergillosis support groups and meetings provide welcoming online spaces for patients, carers and supporters. You can also explore the wider aspergillosis community and support hub.
Making room for difficult emotions
Trying to suppress every frightening, angry or unhappy thought can require enormous effort.
Approaches such as mindfulness and Acceptance and Commitment Therapy, usually shortened to ACT, do not ask people to pretend that difficult feelings are unimportant. Instead, they aim to help people make room for those feelings while continuing to take actions connected with what matters to them.
The aim is not to eliminate all distress. It is to reduce the extent to which distress controls every decision.
Our article on managing the stress of living with chronic disease explores grounding, mindfulness, breathwork and other ways of responding to prolonged stress.
Setting goals that belong to your life now
Goals can restore a sense of direction and control, but they may need to change.
A goal does not have to be dramatic. It might be:
- taking a short walk
- meeting a friend
- returning to a hobby in a modified form
- attending an important family occasion
- preparing one meal
- asking for help before reaching exhaustion.
Changing a goal is not necessarily failure. Sometimes it is how we preserve the part of the goal that matters most.
You are more than your diagnosis
One danger of chronic illness is that it can gradually take over your identity.
Medical appointments, symptoms, prescriptions and test results may begin to dominate everyday conversation. You may find yourself thinking about your life mainly in terms of what your body can no longer do.
But you are not simply “an aspergillosis patient”.
You may also be a parent, partner, grandparent, friend, musician, gardener, engineer, teacher, artist or volunteer.
Illness may change how you fulfil those roles. It does not erase them.
It can help to ask:
“What matters to me, and is there another way I can still be part of it?”
You may no longer be able to host a large family gathering, but perhaps you can spend quieter time with one or two people. You may no longer manage a full day in the garden, but you may still be able to grow something in a container near the house.
Adaptation is not always about doing less. Often, it is about protecting what matters most.
Where people find strength
Although the journey is different for everyone, many people eventually discover something that helps them continue moving forward.
For some, it is family or friendship.
For others, it is faith.
Some find strength in nature, creativity, humour, community, personal values or helping other people.
One patient shared these words with us:
“I have to constantly remind myself that God is sovereign and in all things He is working for good to bring me to a greater understanding of who He is.”
Not everyone shares the same beliefs, but many people describe finding comfort in something that feels larger than the illness itself. That source of strength is deeply personal, and there is no single right answer.
Hope changes too
When people are first diagnosed, hope often means hoping for a cure or a complete return to their previous life.
Over time, hope may take on different forms.
Hope may mean:
- having more good days than bad ones
- finding a treatment with fewer side effects
- walking a little further than last month
- reducing the need for steroid treatment
- taking a holiday
- seeing grandchildren grow up
- feeling useful and connected
- discovering that life still contains pleasure and meaning.
This is not necessarily a smaller or weaker form of hope.
It is hope that has adapted to reality while continuing to look forward.
When additional help may be needed
Sadness, frustration, anger and fear are understandable responses to chronic illness. However, sometimes emotional distress becomes persistent or begins to affect every part of life.
Consider speaking to your GP or healthcare team if you are:
- feeling low or hopeless most of the time
- experiencing frequent panic or overwhelming anxiety
- withdrawing from everyone around you
- unable to sleep because of worry
- losing interest in nearly everything you previously valued
- finding that distress is making it difficult to manage medication, food or basic daily care.
Seeking psychological support does not mean that your physical symptoms are “all in your head”. Chronic physical illness places genuine demands on emotional wellbeing, and receiving help with those demands is part of caring for the whole person.
The NHS has practical guidance on looking after your mental health when living with physical illness. Its Every Mind Matters service also provides advice about stress, anxiety, low mood and sleep.
You are not alone
If you are finding it difficult to accept a chronic illness, you are in very good company.
Almost everyone living with a long-term condition experiences periods of sadness, frustration, fear or grief.
These feelings do not mean you are weak.
They do not mean you are failing.
They mean you are adapting to one of life’s greatest challenges.
Not once, but over and over again.
You may adapt hundreds of times during your journey:
To good news.
To bad news.
To better days.
To worse days.
To new medication.
To unexpected side effects.
To a reassuring scan.
To a worrying blood result.
To holidays that happen.
To holidays that have to be cancelled.
To the loss of something you valued.
To the discovery of something new that brings you joy.
Acceptance is not a finish line.
It is a lifelong process of adapting to change while holding on to the things that matter most.
Life may not be the one you planned.
But it can still be a life filled with love, purpose, hope and moments of genuine happiness.
Further support
Living with chronic illness can sometimes feel overwhelming, but you do not have to face it alone.
You may find it helpful to talk to:
- your GP
- your respiratory or specialist team
- a trusted friend or relative
- a counsellor, psychologist or NHS Talking Therapies service
- other people living with a similar condition.
For aspergillosis-specific support, visit our support groups and meetings page.
References and further reading
- Stanton AL, Revenson TA, Tennen H. Health psychology: psychological adjustment to chronic disease. Annual Review of Psychology. 2007;58:565–592. View on PubMed.
- Bonanno GA, Westphal M, Mancini AD. Resilience to loss and potential trauma. Annual Review of Clinical Psychology. 2011;7:511–535. View on PubMed.
- Graham CD, Gouick J, Krahé C, Gillanders D. A systematic review of the use of Acceptance and Commitment Therapy in chronic disease and long-term conditions. Clinical Psychology Review. 2016;46:46–58. View on PubMed.
- Herbert MS, Dochat C, Wooldridge JS, et al. Technology-supported Acceptance and Commitment Therapy for chronic health conditions: a systematic review and meta-analysis. Behaviour Research and Therapy. 2022;148:103995. View on PubMed.
This article provides general information and emotional support. It is not a substitute for individual medical or psychological advice. Please speak to your GP, specialist team or another qualified healthcare professional about your own circumstances.
Aspergillosis Research Update: ICU Infections, Immune Defences and Antifungal Treatment
Published: July 2026
Medical research into aspergillosis continues to advance rapidly, with new studies appearing almost every week. Some confirm what doctors already suspected, while others introduce new ideas about how the body fights fungal infections or how treatment might improve in the future.
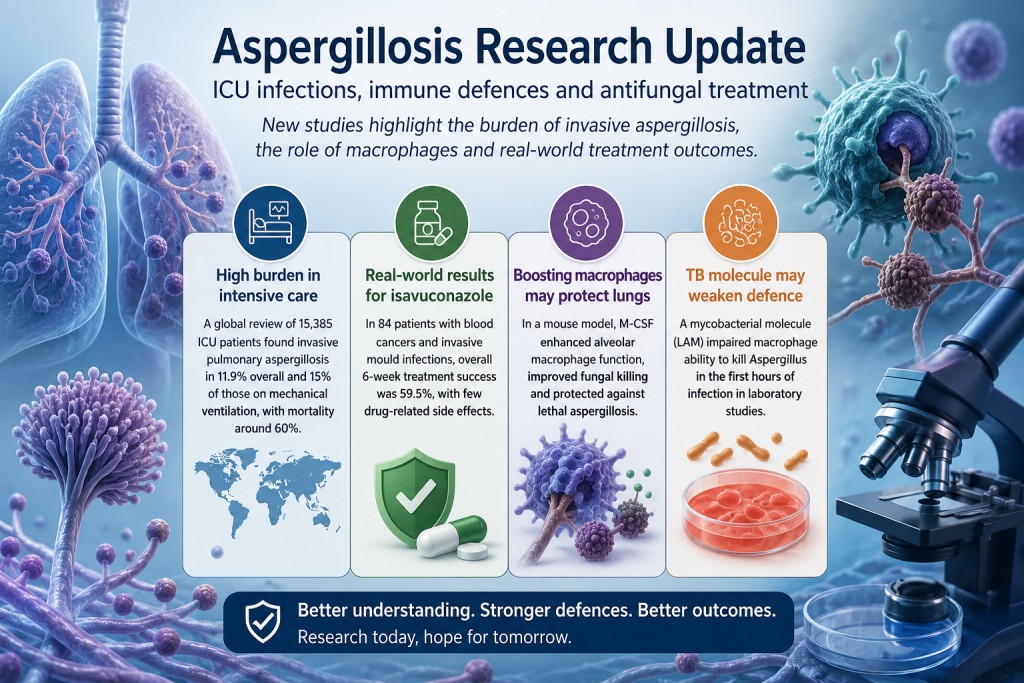
This week’s research includes a major international review of invasive aspergillosis in intensive care, encouraging real-world results for the antifungal drug isavuconazole, and two laboratory studies suggesting that specialised immune cells called macrophages may play an even greater role in protecting the lungs than previously appreciated.
None of these studies changes current treatment recommendations immediately. Together, however, they highlight an important direction in aspergillosis research: understanding not only how to kill the fungus, but also how to strengthen the body’s own immune defences.
A major international review confirms the burden of invasive aspergillosis in intensive care
A systematic review and meta-analysis combined results from 56 observational studies involving 15,385 intensive care patients. Among these patients, 2,381 cases of invasive pulmonary aspergillosis, or IPA, were identified.
The researchers estimated that IPA occurred in approximately 11.9% of the critically ill patients included in the studies. The estimated incidence increased to 15% among patients receiving mechanical ventilation.
Mortality among patients diagnosed with IPA was high:
- 59.6% overall mortality
- 61.9% mortality among mechanically ventilated patients
Factors associated with an increased risk of developing IPA included:
- immunosuppression;
- blood cancers and other malignancies;
- corticosteroid use before admission to intensive care;
- chronic lung, kidney, liver or heart disease;
- mechanical ventilation;
- vasopressor treatment;
- and renal replacement therapy.
What does this mean?
This study reinforces that invasive aspergillosis remains a serious complication in selected critically ill patients.
However, the results should not be interpreted as meaning that approximately one in eight people admitted to intensive care will develop aspergillosis. The authors state that the evidence predominantly reflects COVID-19-associated pulmonary aspergillosis, commonly known as CAPA.
Many of the identified risk factors, such as mechanical ventilation, vasopressor treatment and renal replacement therapy, are also signs that a patient is already extremely unwell. The study therefore identifies associations but cannot prove that these treatments independently cause aspergillosis.
The authors conclude that targeted screening and tailored antifungal strategies in high-risk patients deserve prospective evaluation. They do not claim that universal screening or preventive antifungal treatment has already been shown to improve survival.
Read the paper record on PubMed
Real-world evidence continues to support isavuconazole
Another study examined how well isavuconazole performs in routine clinical practice among people with blood cancers who develop serious invasive mould infections.
The retrospective study included 84 adults treated at two hospitals in China between 2022 and 2025:
- 62 had invasive aspergillosis;
- 14 had mucormycosis;
- 8 had mixed mould infections.
The main measure of success was assessed after six weeks. To count as successful treatment, the patient had to survive, show clinical or radiological improvement and avoid stopping treatment because of failure or toxicity.
The overall six-week treatment success rate was 59.5%. Among patients with aspergillosis, treatment success was higher, at 69.4%.
Only four patients experienced recorded drug-related adverse effects, and one stopped treatment because of vomiting.
What does this mean?
These findings are reassuring because they reflect routine clinical practice rather than the more controlled circumstances of a clinical trial.
The study found that patients receiving isavuconazole alone appeared to have better outcomes than those receiving combination antifungal treatment. However, this result must be interpreted cautiously.
Doctors commonly reserve combination therapy for patients who are more severely ill, have failed previous treatment, have mixed infections or are suspected of having resistant disease. The poorer outcomes in the combination-treatment group may therefore reflect the severity of the patients’ infections rather than harm caused by combining antifungal medicines.
This is known as confounding by indication. Because the patients were not randomly assigned to treatment, the study cannot establish that monotherapy is superior to combination treatment.
Overall, the study adds confidence that isavuconazole can be an effective and generally well-tolerated treatment for invasive aspergillosis in patients with haematological malignancies. It does not show that isavuconazole is better than other antifungal medicines, and it does not apply directly to chronic pulmonary aspergillosis, ABPA or Aspergillus bronchitis.
Read the paper record on PubMed
Could strengthening lung macrophages help prevent invasive aspergillosis?
Perhaps the most scientifically intriguing study this week did not test a new antifungal drug.
Instead, researchers investigated whether they could improve the ability of the lung’s own immune cells to eliminate Aspergillus fumigatus before infection became established.
The study focused on alveolar macrophages. These specialised immune cells live inside the air sacs of the lungs and are among the first cells to encounter inhaled Aspergillus spores.
Using a stem-cell transplant mouse model and an unusually low dose of Aspergillus spores intended to resemble everyday exposure, the researchers found that alveolar macrophages played a crucial role in protecting against invasive aspergillosis during the earliest stages of infection.
The researchers then tested whether macrophage function could be improved using macrophage colony-stimulating factor, or M-CSF.
M-CSF treatment:
- improved macrophage migration;
- enhanced phagolysosomal function;
- increased fungal killing;
- preserved lung tissue;
- reduced inflammatory cytokines;
- and protected mice against lethal invasive aspergillosis.
The researchers also tested primary human alveolar macrophages and found that M-CSF improved several of the same antifungal functions.
Importantly, the protective effect disappeared when alveolar macrophages were removed. This provides strong experimental evidence that the macrophages themselves were responsible for much of the benefit.
What does this mean?
This research suggests that tissue-resident macrophages may play an especially important role during the first hours after Aspergillus spores reach the lungs.
It also supports the wider idea of host-directed therapy: treatments designed to strengthen the patient’s immune response rather than attacking the fungus directly.
However, this study was carried out mainly in mice and has been published as a preprint. It has not yet completed formal peer review.
M-CSF is therefore not an established treatment for aspergillosis. Researchers would need to establish appropriate dosing, safety and effectiveness in people, particularly because stimulating immune activity after stem-cell transplantation could potentially affect inflammation, graft-versus-host disease and other immune processes.
Tuberculosis may affect immune defences as well as damaging the lungs
People who have previously had pulmonary tuberculosis are at increased risk of developing chronic pulmonary aspergillosis, or CPA.
The usual explanation is structural lung damage. Tuberculosis may leave behind cavities, scarring, bronchiectasis and damaged airways, creating an environment in which Aspergillus can persist.
A new laboratory study suggests that there may also be an immunological component.
The researchers studied a mycobacterial cell-wall molecule called lipoarabinomannan, or LAM. This molecule is known to interfere with some of the cellular pathways used by macrophages to respond to infection.
Bone-marrow-derived macrophages were exposed to two forms of LAM and then challenged with swollen Aspergillus fumigatus conidia.
Exposure to LAM:
- increased macrophage death;
- increased inflammatory cytokine release, particularly IL-1β;
- and reduced the ability of macrophages to kill Aspergillus conidia during the first six hours of infection.
The reduction in fungal killing was demonstrated using both colony-counting methods and time-lapse fluorescence microscopy.
What does this mean?
This study provides a plausible biological mechanism through which mycobacterial infection might interfere with early antifungal immune responses.
It does not, however, prove that this mechanism causes CPA after tuberculosis.
The experiments were conducted in laboratory-grown macrophages. They do not show that LAM remains present in the lungs for months or years after tuberculosis, nor that macrophages from people with previous tuberculosis behave in the same way.
The findings therefore do not replace the established structural explanation linking tuberculosis and CPA. Instead, they raise the possibility that lung damage and altered local immunity may work together.
Read the paper record on PubMed
A common theme emerges: macrophages matter
Although these studies examined different questions, two independent research groups reached complementary conclusions.
One study found that strengthening macrophage activity improved fungal killing and survival. The other found that disrupting macrophage activity reduced fungal killing.
Together, they support an emerging view that alveolar macrophages may be central to determining whether inhaled Aspergillus spores are cleared rapidly or allowed to develop into disease.
This does not reduce the importance of neutrophils, antifungal medicines or structural lung damage. Instead, it adds a more detailed understanding of what may happen during the earliest stages of fungal exposure.
Future advances in aspergillosis treatment may therefore involve both:
- better drugs that attack Aspergillus directly;
- and treatments that help the immune system respond more effectively.
What does this mean for people living with aspergillosis?
For most patients currently receiving treatment, these studies do not change day-to-day management.
Antifungal medicines remain the foundation of treatment for invasive and chronic Aspergillus infection. Patients should continue following the advice of their respiratory, infectious-diseases or specialist aspergillosis team.
These studies nevertheless provide encouraging evidence that aspergillosis research is progressing across several fronts:
- improving recognition of invasive aspergillosis in intensive care;
- evaluating how existing antifungal treatments perform in routine practice;
- understanding why some people are more vulnerable to Aspergillus than others;
- and exploring whether the immune system itself could become a future treatment target.
Progress is often gradual, and laboratory findings do not always lead to successful treatments. However, each study adds another piece to the puzzle and helps researchers move towards more effective and more personalised approaches to aspergillosis.
References
- Zhou Z, Luo B, Zhang X, et al. Incidence, mortality and risk factors of invasive pulmonary aspergillosis in critically ill patients during the COVID-19 era: a global systematic review and meta-analysis. Annals of Clinical Microbiology and Antimicrobials. Published 10 July 2026. PubMed. DOI.
- Zhang J, Xu M, Mao J, et al. Isavuconazole for invasive mold disease in patients with hematological malignancies: a multicenter real-world study from China on efficacy, safety, and competing risks. Antimicrobial Agents and Chemotherapy. Published 6 July 2026. PubMed. DOI.
- Sheta D, Mokhtari Z, Strobel M, et al. M-CSF-stimulated alveolar macrophages safeguard from invasive aspergillosis. bioRxiv. Preprint published 9 July 2026. DOI and preprint.
- Gonzales-Huerta LE, Williams TJ, Aljohani R, et al. Mycobacterial lipoarabinomannan negatively interferes with macrophage responses to Aspergillus fumigatus in vitro. PLOS ONE. 2026;21(7):e0351935. PubMed. DOI.
This article summarises newly published research for patients and non-specialist readers. It does not replace individual medical advice from a qualified healthcare professional.

How to Remove Mould from Your Washing Machine and Stop It Coming Back
Mould inside a washing machine is common, particularly in front-loading machines. It often develops in the rubber door seal, detergent drawer, filter and other areas where moisture and detergent residue collect.
For most people, a small amount of washing-machine mould is mainly an unpleasant cleaning problem. However, people living with aspergillosis, severe asthma, allergies or other long-term lung conditions may reasonably want to reduce avoidable mould exposure in the home.
The most effective approach is not only to remove visible mould, but also to keep the machine dry and clean enough to prevent it returning.
Key points
- Mould grows where moisture, detergent residue and dirt remain inside the machine.
- The rubber door seal and detergent drawer are the most common problem areas.
- Use gentle cleaning methods that avoid spraying mould spores or strong chemicals into the air.
- Never mix bleach with vinegar, acidic cleaners, ammonia or other cleaning products.
- Leaving the door and detergent drawer open between washes can greatly reduce recurrence.
Why does mould grow inside washing machines?
Modern washing machines often use less water and lower washing temperatures. This saves energy, but it can also allow detergent residue, fabric conditioner, skin oils, dirt and moisture to build up inside the machine.
Mould is more likely to develop when:
- the door is closed immediately after a wash;
- wet laundry is left inside the drum;
- mostly cool or eco washes are used;
- too much detergent or fabric conditioner is added;
- the rubber seal is not wiped or allowed to dry;
- the detergent drawer or filter is rarely cleaned;
- the machine is kept in a poorly ventilated room.
Where to check for mould
Mould may not always be immediately visible. Check the following areas carefully:
- Rubber door seal: pull back the folds and inspect underneath.
- Detergent drawer: remove it if possible and check the compartment behind it.
- Drum: look around the door opening and drainage holes.
- Filter: check the manufacturer’s instructions before opening it.
- Drainage area: persistent odours may indicate residue or stagnant water deeper inside the machine.
Before you start cleaning
Check the washing machine manufacturer’s instructions first. Different manufacturers recommend different cleaning products, temperatures and maintenance programmes.
To reduce exposure while cleaning:
- open a window or improve ventilation;
- wear household cleaning gloves;
- avoid leaning directly over mouldy areas;
- use damp disposable cloths rather than dry brushing;
- avoid scraping or scrubbing so vigorously that material is dispersed into the air;
- ask someone else to clean the machine if mould exposure usually worsens your breathing.
Some people with aspergillosis or severe respiratory disease may choose to wear a well-fitting FFP2 or FFP3 mask during mould cleaning. A mask does not replace ventilation or careful cleaning methods.
How to clean mould from the rubber door seal
- Switch off the washing machine.
- Gently pull back the folds of the rubber seal.
- Remove any trapped lint, hair, tissues or other debris.
- Wipe the area using a damp cloth and a cleaning product approved by the machine manufacturer.
- Pay particular attention to the lower part of the seal, where water often collects.
- Use a clean damp cloth to remove any remaining cleaning product.
- Dry the seal thoroughly.
Black staining may remain even after mould has been removed. Persistent staining does not always mean that mould is still actively growing, but damaged or deeply contaminated seals may need replacing.
How to clean the detergent drawer
- Remove the drawer according to the manufacturer’s instructions.
- Wash it with warm water and washing-up liquid.
- Use a small brush for narrow areas, taking care not to flick residue into the air.
- Wipe the compartment where the drawer sits.
- Rinse and dry the drawer before replacing it.
Using too much detergent or fabric conditioner can encourage residue to collect in this area. Follow the dosing instructions for your detergent and local water hardness.
Cleaning the filter
Many washing machines have a filter behind a small panel near the bottom of the machine. This may collect lint, hair, coins and other debris.
Before opening it:
- read the manufacturer’s instructions;
- switch off and unplug the machine;
- place towels or a shallow tray underneath, as water may escape;
- allow hot water to cool before opening the filter.
Clean the filter, remove debris and replace it securely. A blocked or dirty filter can contribute to poor drainage and unpleasant smells.
Run a maintenance wash
After cleaning the visible parts of the machine, run the manufacturer’s drum-clean or maintenance programme.
If the machine does not have a dedicated cleaning cycle, the manufacturer may recommend an empty hot wash. Use only a cleaning product that is suitable for your particular machine.
Do not assume that adding more cleaner will work better. Excessive detergent or cleaning product may leave additional residue behind.
Avoid mixing cleaning chemicals
Important safety warning
Never mix bleach with vinegar, limescale remover, toilet cleaner, ammonia or other household cleaning products.
Mixing bleach with acidic products can release chlorine gas, which can cause serious breathing difficulties and may require urgent medical attention.
Use one product at a time, follow the label instructions and rinse surfaces before using any different product.
How to stop washing-machine mould coming back
Keeping the machine dry between washes is often more effective than repeatedly carrying out deep cleaning.
- Remove laundry promptly when the cycle finishes.
- Leave the washing-machine door slightly open between washes.
- Leave the detergent drawer open so it can dry.
- Wipe moisture from the door seal, particularly from the lower folds.
- Use the correct amount of detergent.
- Reduce or avoid fabric conditioner if residue repeatedly builds up.
- Run the manufacturer’s maintenance cycle regularly.
- Clean the drawer, seal and filter routinely.
- Make sure the room is adequately ventilated.
How often should the machine be cleaned?
There is no single schedule suitable for every household. A machine used daily may need more frequent attention than one used only occasionally.
As a practical guide:
- wipe and check the door seal every week or two;
- clean the detergent drawer approximately once a month;
- run a maintenance wash according to the manufacturer’s advice;
- check the filter every few months, or sooner if drainage becomes slow or the machine smells.
Clean the machine sooner if you notice visible mould, slime, residue or a persistent musty smell.
When should the door seal be replaced?
Replacing the rubber door seal may be more effective than repeated cleaning if:
- the seal is cracked, torn or misshapen;
- mould is deeply embedded in the rubber;
- water repeatedly collects because the seal is damaged;
- the machine leaks;
- a persistent smell remains after thorough cleaning.
A competent appliance engineer may be able to replace the seal without replacing the whole washing machine.
When might the washing machine need professional attention?
Consider contacting the manufacturer or an appliance engineer if:
- the machine does not drain properly;
- stagnant water remains inside;
- the smell returns immediately after cleaning;
- mould appears to be growing behind inaccessible panels;
- the machine leaks;
- the seal or internal pipework needs replacing.
Is washing-machine mould dangerous for people with aspergillosis?
Finding mould in a washing machine does not necessarily mean that your home contains unusually high levels of airborne mould. Washing machines are naturally damp environments, and small amounts of mould are common.
However, people with aspergillosis or other significant respiratory conditions may wish to take reasonable precautions, particularly when disturbing visible mould.
Try to avoid:
- dry brushing;
- scraping large mouldy areas;
- using sprays that create a fine mist;
- mixing cleaning chemicals;
- remaining in a poorly ventilated room while strong products are being used.
If cleaning mould reliably causes coughing, wheezing, chest tightness or breathlessness, ask someone else to do the cleaning where possible.
When to seek medical advice
Seek medical advice if you develop a persistent worsening of respiratory symptoms after mould exposure, particularly if you have aspergillosis, severe asthma, bronchiectasis or another chronic lung condition.
Call 999 or seek urgent medical help if exposure to cleaning chemicals causes severe breathlessness, chest pain, confusion, collapse or difficulty speaking in full sentences.
Frequently asked questions
Can I use bleach in my washing machine?
Only use bleach if the washing-machine manufacturer states that it is safe for your model. Bleach can damage some rubber seals, metal parts and internal components.
Never mix bleach with vinegar or any other cleaning product.
Can I use vinegar?
Some manufacturers advise against regular vinegar use because concentrated acids may damage rubber seals or internal components. Check the instructions for your machine before using it.
Does a hot wash kill mould?
A hot maintenance wash may help reduce microorganisms and remove detergent residue, but it may not remove mould that is deeply embedded in a damaged rubber seal. Physical cleaning and drying are still important.
Should I replace the machine if there is mould in the seal?
Usually not. The seal can often be cleaned or replaced. Replacing the entire machine is generally only necessary if there is extensive inaccessible contamination, repeated drainage problems or the cost of repair is not economical.
Should I keep the door open all the time?
Leaving the door slightly open helps moisture evaporate. However, consider the safety of children and pets, who may climb into an open machine. Keep the laundry area secure where necessary.
Does washing at low temperatures cause mould?
Low-temperature washes can contribute to residue building up inside the machine, particularly if too much detergent or fabric conditioner is used. Regular maintenance cycles can help control this.
Related information
- Choosing a face mask for protection from dust and mould
- Getting help with damp and mould in rented housing
- Indoor air quality and aspergillosis
- Damp and mould in the home
Always follow the cleaning and maintenance instructions supplied by the manufacturer of your washing machine.
Why Can an Asthma Drug Help ABPA? Understanding Xolair (Omalizumab)
Originally published: 8 July 2026
Last reviewed: 8 July 2026
Many people diagnosed with Allergic Bronchopulmonary Aspergillosis (ABPA) are surprised when their specialist suggests Xolair (omalizumab).
"I thought Xolair was an asthma medication. How can it possibly help a fungal lung disease?"
It is a very reasonable question.
The answer is that ABPA is not simply an infection caused by Aspergillus. It is an allergic lung disease in which the immune system overreacts to the presence of Aspergillus in the airways.
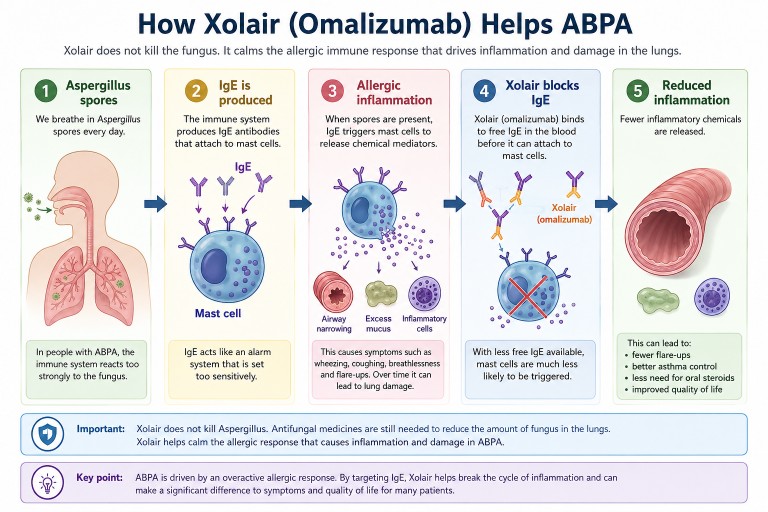
Xolair does not kill the fungus. Instead, it helps calm the allergic immune response that drives many of the symptoms of ABPA.
Key Points
- Xolair (omalizumab) is a biologic medicine originally developed for severe allergic asthma.
- Many people with ABPA also have severe allergic asthma.
- Omalizumab targets IgE, an antibody involved in allergic inflammation.
- In the UK, omalizumab is usually prescribed through NHS severe asthma pathways, not because ABPA itself is a licensed indication.
- Treating severe allergic asthma can also improve ABPA because the two conditions share important allergic immune pathways.
- Biosimilar versions of omalizumab are now becoming available, which may make biologic treatment more accessible for eligible patients.
Understanding ABPA
Everyone breathes in Aspergillus spores every day.
For most people, this causes no illness. In people with ABPA, however, the immune system reacts too strongly. Instead of ignoring the spores, it launches an exaggerated allergic response.
This can cause:
- airway inflammation
- wheezing
- coughing
- breathlessness
- excessive mucus production
- repeated flare-ups
- gradual lung damage if poorly controlled.
In many patients, the allergic response causes more problems than the fungus itself.
That is why doctors may treat both the amount of fungus in the airways and the immune system's overreaction to it.
What Does IgE Have To Do With ABPA?
One of the key parts of allergic disease is an antibody called Immunoglobulin E, usually shortened to IgE.
Think of IgE as part of the body's allergy alarm system.
In ABPA, the immune system produces IgE against Aspergillus. This can trigger immune cells to release chemicals that cause allergic inflammation. These chemicals narrow the airways, increase mucus production and attract other inflammatory cells, including eosinophils.
Doctors often measure total IgE because it is important in diagnosing and monitoring ABPA.
How Does Xolair Work?
Xolair (omalizumab) is a biologic medicine. Biologics are targeted treatments designed to block specific parts of the immune system.
Omalizumab attaches to free IgE antibodies before they can trigger the allergic cascade.
As a result:
- allergic inflammation may be reduced
- asthma symptoms may improve
- flare-ups may become less frequent
- some patients may be able to reduce oral steroid treatment
- quality of life may improve.
Xolair does not kill Aspergillus.
Instead, it reduces the body's excessive allergic response to the fungus.
Why Was I Offered An Asthma Drug?
This is one of the most common questions patients ask.
Although ABPA is a distinct condition, many people with ABPA also have severe allergic asthma. The two conditions share many of the same allergic immune pathways, particularly those involving IgE.
In the UK, omalizumab is not currently licensed specifically for ABPA.
Many patients receive omalizumab because they meet NHS eligibility criteria for severe allergic asthma. When the allergic asthma improves, the ABPA may also improve because both conditions are driven by overlapping allergic inflammation.
In other words, the treatment is not aimed at killing Aspergillus. It is aimed at reducing the allergic inflammation that contributes to both severe asthma and ABPA.
Why Can't Everyone With ABPA Have Xolair?
This is an important question.
In the NHS, access to omalizumab is usually based on nationally agreed eligibility criteria for licensed conditions such as severe allergic asthma. A diagnosis of ABPA alone does not usually make someone eligible for omalizumab treatment.
This does not mean omalizumab cannot help some people with ABPA. It means that NHS prescribing is guided by licensing, NICE recommendations, commissioning arrangements and clinical judgement.
Your respiratory specialist will consider your asthma severity, ABPA history, IgE levels, previous treatments, steroid exposure, flare-up frequency and overall health when deciding whether a biologic medicine may be appropriate.
Why Aren't Antifungal Drugs Enough?
Antifungal medicines such as itraconazole or voriconazole reduce the amount of Aspergillus growing in the airways.
However, reducing the fungus does not always completely switch off the allergic immune response.
Different treatments target different parts of the disease:
| Treatment | Main purpose |
|---|---|
| Antifungal medicines | Reduce the amount of Aspergillus |
| Corticosteroids | Reduce widespread inflammation |
| Biologics such as omalizumab | Target specific allergic pathways |
| Airway clearance | Help remove mucus from the lungs |
These treatments often work together rather than replacing one another.
Why Have Steroids Been Used For So Long?
For many years, oral corticosteroids such as prednisolone have been a main treatment for ABPA.
Steroids are often effective at controlling inflammation quickly, but prolonged or repeated courses can cause significant side effects, including:
- weight gain
- diabetes
- osteoporosis
- cataracts
- mood changes
- increased infection risk
- adrenal suppression or adrenal insufficiency.
One reason biologics are important is that they may help some suitable patients reduce their need for long-term oral steroids under specialist supervision.
Does Xolair Help Everyone?
No.
Some patients experience major improvements. Others notice more gradual changes. A small number may gain little benefit and may be better suited to a different biologic medicine.
Published studies and specialist-centre experience suggest that some patients with ABPA treated with omalizumab may experience:
- fewer exacerbations
- better asthma control
- reduced oral steroid requirements
- improved quality of life.
Because ABPA is relatively uncommon, much of the evidence comes from case series, observational studies, smaller trials and systematic reviews rather than the very large trials often performed for common diseases.
Why Isn't Xolair Licensed Specifically For ABPA?
This can be confusing for patients.
Being "not licensed for ABPA" does not necessarily mean there is no evidence that omalizumab can help. It means that the medicine has not gone through the formal licensing process for ABPA as a specific indication.
Licensing a medicine for a new condition usually requires large, expensive clinical trials. ABPA is a relatively uncommon disease, which makes such studies difficult to organise and fund.
There is also less commercial incentive now that omalizumab biosimilars are becoming available. No single manufacturer may have a strong reason to fund large registration trials for an additional ABPA indication.
As a result, the scientific evidence and clinical experience have grown faster than the formal licensing process.
Why Is Omalizumab Back In The News?
Omalizumab itself is not new. It has been used for severe allergic asthma for more than twenty years.
What is new is the increasing availability of biosimilar omalizumab.
Biosimilars are highly similar versions of an existing biologic medicine. They must show comparable quality, safety and effectiveness before approval.
This matters because biologic medicines are expensive. Increased competition from biosimilars is expected to reduce costs over time.
Lower costs may improve access for patients who meet NHS eligibility criteria and may also increase research interest in biologic treatment for conditions such as ABPA.
It is important not to overpromise: biosimilars do not automatically mean that everyone with ABPA will be offered omalizumab. NHS access will still depend on eligibility criteria, clinical assessment and local pathways.
Are There Other Biologics?
Yes.
Omalizumab was the first biologic widely used in allergic asthma and has been used in selected patients with ABPA. Newer biologics target different parts of the allergic inflammatory pathway.
Depending on an individual's disease pattern, specialists may consider medicines such as:
- mepolizumab
- benralizumab
- dupilumab
- tezepelumab.
Research is continuing to determine which patients are most likely to benefit from each biologic.
Questions You May Wish To Ask Your Specialist
- Why do you think omalizumab is appropriate for me?
- Am I being considered for this because of severe allergic asthma, ABPA, or both?
- How long before we know whether it is working?
- Will I still need antifungal treatment?
- Could this help reduce my oral steroid dose?
- What side effects should I watch for?
- Would another biologic be more suitable for my type of inflammation?
The Bottom Line
Xolair (omalizumab) was originally developed for severe allergic asthma, but it can also help some people with ABPA because ABPA is strongly driven by allergic immune inflammation.
In the NHS, omalizumab is usually prescribed through severe asthma pathways rather than because ABPA itself is a licensed indication.
It is not an antifungal drug and it is not a cure for ABPA. Instead, it is part of a modern treatment approach that may include antifungal medicines, airway clearance, corticosteroids, monitoring and biologic therapy in selected patients.
With biosimilar omalizumab becoming available and newer biologics continuing to emerge, treatment options for severe allergic lung disease are changing. For people living with ABPA, this is an important and rapidly developing area of care.
Related Articles
- Understanding Biologic Treatments for Aspergillosis
- ABPA: A Complete Patient Guide
- Understanding Steroids, Cortisol, ACTH and Adrenal Suppression
- Can Biologics Reduce the Need for Steroids?

Vaccinations for People Living with Aspergillosis

First published: [add original date]
Last reviewed: July 2026
Vaccinations are an important part of staying well when you live with aspergillosis or another long-term lung condition. They cannot prevent aspergillosis itself, but they can reduce the risk of infections that may make breathing symptoms worse, trigger flare-ups, or lead to hospital admission.
International readers: This article explains why vaccination matters for people living with aspergillosis. Vaccine recommendations, availability and eligibility vary between countries. Where healthcare-system information is included, it refers to the UK unless otherwise stated. Always follow advice from your own healthcare team.
Key points
- Vaccines do not prevent aspergillosis, but they can reduce the risk of serious infections that may worsen lung disease.
- People with aspergillosis often also have asthma, bronchiectasis, COPD or immune system problems, which can make infections more serious.
- Flu, COVID-19, pneumococcal, RSV and shingles vaccines may be relevant, depending on your age, health conditions and local guidance.
- Some people need additional vaccines or vaccine-response testing as part of specialist immunology care.
- If you take long-term steroids, biologics or other immune-suppressing medicines, ask which vaccines are suitable for you.
Why vaccination matters if you have aspergillosis
Many people living with aspergillosis already have lungs that are more vulnerable than usual. This may be because of asthma, bronchiectasis, COPD, previous infection, scarring, mucus plugging, cavities in the lung, or reduced lung function.
For this reason, an infection that is mild for one person can sometimes cause a much bigger setback for someone with aspergillosis. A respiratory infection may lead to increased breathlessness, more coughing, thicker sputum, a flare-up of asthma or COPD, or a chest infection that takes weeks to recover from.
Vaccination is one way to reduce this risk. It does not replace usual aspergillosis treatment, airway clearance, antifungal medication, inhalers or other care, but it can be an important part of protecting your lungs.
Which vaccines are most important?
The vaccines that matter most will depend on your age, diagnosis, immune system, medications, previous vaccine history and the country where you live. The vaccines below are commonly discussed for people with long-term lung disease or increased infection risk.
Influenza (flu) vaccine
For many people living with aspergillosis, the annual flu vaccine is one of the most important ways to reduce the risk of a serious winter chest infection.
Flu is not just a heavy cold. It can cause fever, severe tiredness, muscle aches and worsening breathing symptoms. In people with asthma, bronchiectasis, COPD or other lung disease, flu may trigger a flare-up or lead to pneumonia.
Because flu viruses change over time, the vaccine is updated regularly and is usually offered each year before the main flu season.
COVID-19 vaccine
COVID-19 can still cause serious illness in people who are older, immunosuppressed or living with chronic lung disease. Some people with aspergillosis may therefore be offered seasonal COVID-19 vaccination or booster doses.
Eligibility changes over time and differs between countries. If you are unsure whether you should receive a COVID-19 booster, ask your GP, pharmacist, respiratory specialist or local healthcare team.
Pneumococcal vaccine
Pneumococcal disease is caused by bacteria that can lead to pneumonia and, less commonly, serious infections such as bloodstream infection or meningitis.
This vaccine is particularly relevant for many people with chronic respiratory disease. People with aspergillosis may also have bronchiectasis, COPD, asthma, scarring or cavities in the lung, all of which can make bacterial chest infections more difficult to recover from.
If you are not sure whether you have had a pneumococcal vaccine, or whether your record is up to date, ask your GP surgery or specialist team.
RSV vaccine
Respiratory syncytial virus, usually called RSV, is a common respiratory virus. In many people it causes cold-like symptoms, but in older adults and people with lung disease it can cause more serious lower respiratory tract infection.
RSV vaccination is a newer area of adult vaccination. Some countries now recommend RSV vaccination for older adults or people at increased risk of severe respiratory illness.
If you are older or have chronic lung disease, it is worth asking whether RSV vaccination is recommended for you.
Shingles vaccine
Shingles is caused by reactivation of the chickenpox virus. It can cause a painful rash and may lead to long-lasting nerve pain.
The shingles vaccine reduces the risk of shingles and its complications. It may be particularly relevant for older adults and some people with weakened immune systems.
Additional vaccines for some people
Some people with aspergillosis also have other medical conditions that affect the immune system or increase their risk of certain infections. In these situations, your specialist may recommend additional vaccines as part of your care.
For example, some people with immune deficiencies, those without a functioning spleen, or people who have received a stem cell transplant may be advised to receive vaccines such as Haemophilus influenzae type b (Hib) or meningococcal vaccines. These vaccines are not routinely recommended for everyone with aspergillosis, but they may be appropriate for certain individuals.
If you have recurrent infections, your respiratory specialist or immunologist may also investigate how well your immune system responds to vaccines. In some cases, measuring antibody responses to vaccines such as the pneumococcal vaccine forms part of an assessment for possible antibody deficiency.
Travel vaccines may also be needed if you are visiting countries where certain infections are more common. If you are planning travel, ask for advice well in advance, especially if you are immunosuppressed.
Vaccines and steroids, biologics or immune-suppressing treatment
Some people with aspergillosis take medicines that affect the immune system, including:
- oral steroids such as prednisolone or methylprednisolone
- long-term or repeated courses of steroids
- biologic medicines for severe asthma or ABPA
- immune-suppressing medicines for other conditions
- chemotherapy or transplant-related medicines
Most routine adult vaccines are not live vaccines and are generally safe for people with chronic lung disease. However, live vaccines may not be suitable for people who are significantly immunosuppressed.
Important: Do not stop steroids, antifungal treatment or biologic medicines just to have a vaccine unless your own doctor tells you to. If you are immunosuppressed, ask your GP, pharmacist or specialist team which vaccines are suitable and when they should be given.
UK NHS information
In the UK, vaccination eligibility is based on age, medical conditions, pregnancy, occupation and immune status. It can also change between seasonal campaigns.
People with chronic respiratory disease are commonly eligible for seasonal flu vaccination and may be eligible for other vaccines depending on their age, diagnosis and treatment. This may include COVID-19 boosters, pneumococcal vaccination, RSV vaccination or shingles vaccination.
Ask your GP surgery, pharmacist or specialist respiratory team whether your vaccination record is up to date. This is especially important if you have:
- bronchiectasis, COPD, severe asthma or another long-term lung condition
- chronic pulmonary aspergillosis (CPA)
- allergic bronchopulmonary aspergillosis (ABPA)
- recurrent chest infections
- long-term steroid treatment
- other immune-suppressing treatment
- a known or suspected immune deficiency
Can vaccines make aspergillosis worse?
Vaccines do not cause aspergillosis. They do not contain Aspergillus and cannot give you a fungal infection.
Some people feel tired, achy or feverish for a short time after vaccination. This is usually a normal immune response and settles within a few days.
If you develop worsening breathlessness, chest pain, coughing blood, oxygen levels lower than usual, or symptoms that feel very different from your usual pattern, seek medical advice.
Should family members be vaccinated?
Vaccination is not only about protecting the individual. If you live with someone who is clinically vulnerable, keeping household vaccinations up to date can reduce the chance of bringing infections into the home.
This may be especially important for people who are immunosuppressed, older, or living with severe lung disease.
Questions to ask your healthcare team
At your next GP, pharmacist or specialist appointment, consider asking:
- Am I eligible for the annual flu vaccine?
- Am I eligible for a COVID-19 booster this season?
- Have I had the correct pneumococcal vaccine?
- Am I eligible for the RSV vaccine?
- Am I eligible for the shingles vaccine?
- Do any of my medicines affect which vaccines I can have?
- Do I need any additional vaccines because of immune problems or recurrent infections?
- Should my antibody response to any vaccine be checked?
- Are any vaccines recommended before starting a new immune-suppressing treatment?
Frequently asked questions
Can I have vaccines while taking antifungal medication?
In most cases, antifungal medicines such as itraconazole, voriconazole, posaconazole or isavuconazole do not prevent vaccination. If you are unsure, ask your pharmacist, GP or specialist team.
Can I have more than one vaccine at the same appointment?
Some vaccines can be given at the same appointment, but this depends on the vaccine, your health and local guidance. Your GP surgery or pharmacist can advise.
Should I delay vaccination if I am unwell?
If you have a high temperature or are acutely unwell, you may be advised to wait until you have recovered. Mild cold symptoms do not always mean vaccination must be delayed, but check with the vaccinator if you are unsure.
What if I had a reaction to a vaccine before?
Tell the vaccinator before receiving any vaccine. Serious allergic reactions are rare, but your history should be checked carefully.
Can vaccines give me aspergillosis?
No. Vaccines do not contain Aspergillus and cannot give you aspergillosis.
When to seek medical advice urgently
Seek urgent medical help if you have:
- severe or rapidly worsening breathlessness
- chest pain
- blue lips or confusion
- coughing up blood
- oxygen levels lower than usual, if you monitor them
- signs of a severe allergic reaction after vaccination, such as swelling of the face or throat, wheezing, collapse or a widespread rash
Useful links
- NHS: Flu vaccine
- NHS: COVID-19 vaccine
- NHS: RSV vaccine
- NHS: Shingles vaccine
- UKHSA: Immunisation against infectious disease — The Green Book
- UKHSA: Pneumococcal vaccination programme
- CDC: Haemophilus influenzae type b vaccine safety
Related information
You may also find these guides helpful:
- What is Aspergillosis?
- Bronchiectasis and Aspergillosis
- Preventing Chest Infections
- Corticosteroids and Aspergillosis
- Biologic Treatments and Aspergillosis
- Travel with Aspergillosis
```
Summary
Vaccination is one of the simplest ways to reduce the risk of serious respiratory infection. For people living with aspergillosis, bronchiectasis, COPD, severe asthma or immune suppression, it is worth checking regularly that your vaccination record is up to date.
The medical reasons for vaccination are relevant internationally, but vaccine eligibility and availability vary between countries. Ask your GP, pharmacist, respiratory specialist or local healthcare team which vaccines are recommended for you.
Preparing for a Disability Assessment: A Practical Guide for People Living with Aspergillosis in UK
Originally published: August 2018
Last reviewed: July 2026
If you have been invited to attend a disability assessment, it is natural to feel anxious. Many people worry about saying the wrong thing, forgetting important information or not being believed.
The purpose of the assessment is not simply to confirm your diagnosis. Instead, it aims to understand how your health condition affects your daily life, including your ability to carry out everyday activities safely, reliably and repeatedly.
For people living with aspergillosis, symptoms such as breathlessness, fatigue, chronic cough, medication side effects and frequent infections can all have a significant impact on daily life, even if they are not always obvious to other people.
This guide explains how to prepare for your assessment and how to describe your symptoms clearly and honestly.
What is a disability assessment?
Several UK benefits and support schemes may involve an assessment of how your condition affects your daily life. These include:
- Personal Independence Payment (PIP)
- Adult Disability Payment (Scotland)
- Employment and Support Allowance (ESA)
- Universal Credit health assessments
The assessment is usually carried out by an independent healthcare professional working on behalf of the Department for Work and Pensions (DWP) or the relevant national authority.
The assessor is interested less in the name of your condition than in understanding how it affects your ability to manage everyday tasks.
Before your assessment
Good preparation can make the assessment less stressful and help ensure you provide an accurate picture of how your condition affects you.
You may find it helpful to gather:
- recent clinic letters
- hospital discharge summaries
- lung function results, where available
- CT scan reports if relevant
- your current medication list
- details of inhalers, nebulisers or oxygen therapy
- letters from your GP or specialist nurse
Having these documents available can help you answer questions confidently and provide supporting evidence if requested.
Keep a symptom diary
Many people underestimate how much their condition affects them because they gradually adapt to living with it.
Keeping a diary for one or two weeks before your assessment can help you remember important details.
Record things such as:
- how far you can walk before stopping
- how often you become breathless
- episodes of coughing or coughing up blood
- levels of fatigue
- sleep disturbance
- days when you cannot leave the house
- help you receive from family or friends
This provides real-life examples that are often easier to explain during the assessment.
Describe your worst days as well as your better days
Many long-term lung conditions fluctuate. Some days may be manageable, while others are much more difficult.
It is important to explain:
- how often bad days occur
- how long they last
- what you cannot do during these periods
If your condition varies, explain what happens on both good and bad days rather than describing only how you feel on the day of the assessment.
Explain how your symptoms affect everyday life
Assessors are interested in the practical impact of your condition.
Rather than simply saying:
"I get breathless."
Explain what that means in daily life.
"I have to stop halfway up the stairs to catch my breath."
Instead of saying:
"I'm tired all the time."
You might explain:
"After having a shower I usually need to rest for an hour before I can prepare breakfast."
These practical examples help assessors understand the real impact of your condition.
Remember the symptoms people cannot see
Not all symptoms are visible.
People living with aspergillosis often experience:
- severe fatigue
- brain fog
- poor concentration
- chronic cough
- disturbed sleep
- medication side effects
- anxiety about breathlessness or haemoptysis
- recurrent infections
These symptoms can significantly affect daily living, even when you appear well during the assessment.
Be honest about the help you need
Many people naturally try to remain independent and may overlook the assistance they receive from others.
Think about whether family members or friends help you with:
- shopping
- housework
- gardening
- transport
- preparing meals
- managing medication
- heavy lifting
Needing help occasionally is still important to mention.
Medication side effects matter too
Your symptoms are only part of the picture.
Treatments for aspergillosis and associated conditions may also affect daily life.
Examples include:
- fatigue
- nausea
- light sensitivity
- tremor
- dizziness
- sleep disturbance
- frequent blood tests and hospital appointments
Explain how these affect your ability to work, travel or carry out everyday activities.
During the assessment
Try not to rush your answers.
If you do not understand a question, ask for it to be repeated or explained.
Answer honestly. Avoid both minimising and exaggerating your symptoms.
If you become upset or need to pause because of coughing or breathlessness, take your time. Assessors understand that some conditions make conversations difficult.
After the assessment
You may wish to request a copy of the assessment report once it has been completed.
If you disagree with the decision, you usually have the right to ask for a mandatory reconsideration and, if necessary, to appeal.
Many successful claims are awarded following reconsideration or appeal, so do not assume the first decision is always final.
Getting support
You do not have to manage the process alone.
Help may be available from:
- Citizens Advice
- local welfare rights advisers
- disability charities
- hospital benefits advisers where available
- your GP or specialist team, who may be able to provide supporting medical evidence
Key points to remember
- Prepare before your assessment.
- Use real-life examples rather than general statements.
- Describe both good days and bad days.
- Include fatigue, medication side effects and invisible symptoms.
- Be honest about the help you need.
- If you disagree with the decision, remember that you may be able to request a review or appeal.
Further information
You may also find these articles helpful:
- Disability Verification and Support for People with Aspergillosis in the UK
- Living with Aspergillosis
- Managing Fatigue
- Understanding Bronchiectasis
References
- Department for Work and Pensions. Personal Independence Payment Assessment Guide.
PIP Assessment Guide for Assessment Providers – GOV.UK
- Department for Work and Pensions. Work Capability Assessment Guidance.
Employment and Support Allowance: Work Capability Assessment – GOV.UK
- Citizens Advice. Benefits and disability assessment guidance.
Benefits guidance – Citizens Advice
- NHS. Living with long-term respiratory conditions.
Living with COPD – NHS

Choosing the Right Face Mask for Aspergillosis | FFP2, FFP3 & Mould Protection
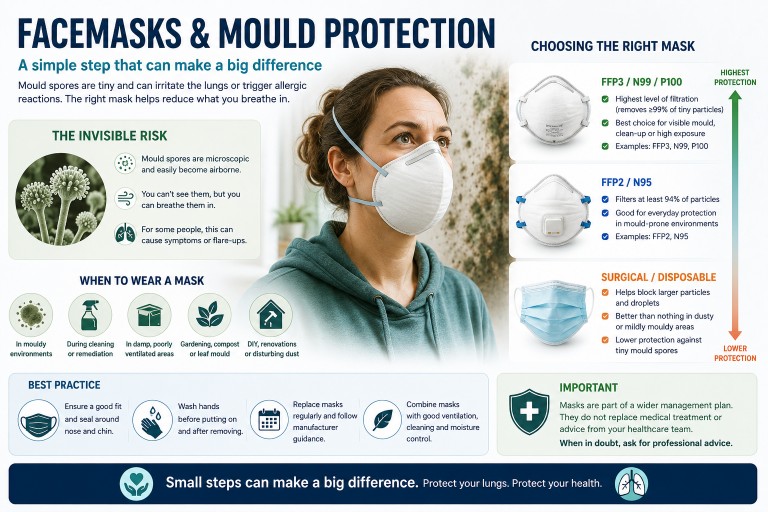
Originally published: Aug 2018
Last reviewed: July 2026
Key points
- Wearing a well-fitting mask can reduce exposure to Aspergillus spores during higher-risk activities.
- FFP2 and FFP3 respirators provide much better protection than cloth face coverings or standard surgical masks.
- The fit of the mask is just as important as the type of mask.
- Masks are most useful for short periods of increased exposure, such as gardening, handling compost or dusty DIY.
- A face mask is only one part of reducing exposure. Ventilation, avoiding unnecessary dust and changing clothes after high-risk activities can also help.
Why might people with aspergillosis wear a face mask?
Aspergillus moulds are common in the environment. Their microscopic spores are present in outdoor and indoor air every day, and for most people they cause no problems.
However, for people living with aspergillosis, severe asthma, bronchiectasis, chronic lung disease or weakened immune systems, breathing in large numbers of fungal spores may increase symptoms or, in some situations, increase the risk of infection.
It is impossible to avoid Aspergillus completely, but reducing exposure during activities that generate large amounts of dust or disturb mouldy material may be helpful.
When is wearing a mask most useful?
You may wish to wear a well-fitting respirator during activities such as:
- gardening, particularly digging or turning soil
- opening bags of compost or potting mix
- leaf clearing
- handling mulch, bark or wood chippings
- cleaning mouldy areas, where appropriate and safe
- DIY projects that create dust
- sweeping sheds, garages or lofts
- visiting farms, stables or grain stores
- construction or demolition work
- working in dusty environments
For some people, avoiding these activities altogether is the safest option. If they cannot be avoided, appropriate respiratory protection may help reduce exposure.
Which type of mask should I choose?
Not all masks provide the same level of protection.
| Mask type | Protection against fungal spores | Recommended? |
|---|---|---|
| Cloth face covering | Low | No |
| Standard surgical mask | Limited | Better than nothing, but not designed for airborne spores |
| FFP2 respirator | Good | Suitable for most situations |
| FFP3 respirator | Excellent | Best disposable option |
| Reusable respirator with P3 filters | Excellent | Useful for frequent or higher-exposure activities |
An FFP2 respirator filters at least 94% of airborne particles when properly fitted.
An FFP3 respirator filters at least 99% of airborne particles and offers the highest level of protection available in disposable masks.
For people who regularly garden or work in dusty environments, a reusable respirator fitted with certified P3 filters may be more comfortable and economical over time.
Fit is just as important as the mask itself
Even the best respirator works poorly if air leaks around the edges.
To improve protection:
- choose the correct size where available
- adjust the nose clip carefully
- tighten the straps so the mask seals comfortably
- ensure the mask covers both your nose and mouth
- check for gaps around the cheeks and chin
- replace disposable masks if they become damp, damaged or difficult to breathe through
Facial hair can prevent a tight seal, reducing the effectiveness of close-fitting respirators.
Valved and non-valved masks
Some respirators have an exhalation valve. Patients often report that these masks feel more comfortable, are less warm and humid, and are less likely to steam up glasses.
A valved FFP2 or FFP3 respirator can help protect the wearer from breathing in dust and fungal spores, provided it fits well. However, the valve allows exhaled air to leave the mask more easily, so it does not filter your breath outwards in the same way as a non-valved mask.
This means valved masks may be useful for gardening, DIY or other mould-exposure activities, but may not be appropriate in healthcare settings or situations where you are trying to reduce the spread of respiratory infections to other people.
Some people also find FFP3 masks harder to breathe through than FFP2 masks because they provide higher filtration. If FFP3 feels too difficult to tolerate, a well-fitting FFP2 respirator may be a more practical option for short, lower-risk activities.
Disposable or reusable?
Disposable FFP2 or FFP3 masks
Advantages:
- lightweight
- convenient
- no maintenance
- widely available
Disadvantages:
- ongoing replacement cost
- more waste
- may not fit every face shape equally well
Reusable respirators
Advantages:
- often provide a better seal
- replaceable filters
- lower long-term cost if used regularly
- less waste
Disadvantages:
- higher initial cost
- require cleaning and maintenance
- bulkier than disposable masks
If you only occasionally garden or carry out DIY, disposable FFP2 or FFP3 masks are usually sufficient. If you need respiratory protection frequently, a reusable respirator may be worth considering.
Are masks uncomfortable?
Many people find respirators take a little time to get used to.
You may notice:
- slightly warmer air inside the mask
- increased humidity
- pressure around the nose
- difficulty wearing glasses without fogging
Taking regular breaks in a safe environment and ensuring a good fit often improves comfort.
Can I wear a mask if I have asthma or bronchiectasis?
Many people with asthma or bronchiectasis can safely wear FFP2 or FFP3 respirators for short periods.
However, masks may feel uncomfortable if you are already very breathless. If wearing a respirator causes significant breathlessness, dizziness or distress, stop the activity, remove the mask in a safe place, and discuss suitable options with your healthcare team.
Other ways to reduce exposure
A mask is only one part of reducing mould exposure.
You may also wish to:
- ask someone else to turn compost or carry out particularly dusty gardening jobs
- wet down dusty materials before moving them, where appropriate
- keep windows closed if neighbours are disturbing large amounts of compost, soil or building dust
- remove outdoor clothing after gardening
- wash your hands after handling soil or compost
- shower and wash your hair after heavy exposure if practical
No mask can eliminate exposure completely, but combining several simple measures can reduce the amount of dust and fungal spores you breathe in.
Where can I buy suitable masks?
Certified FFP2 and FFP3 respirators are widely available from:
- major pharmacies
- builders' merchants
- DIY retailers
- industrial safety equipment suppliers
- reputable online PPE suppliers
When buying a respirator, look for products that meet recognised UK or European standards and carry appropriate certification markings. Avoid products that make unrealistic claims or do not clearly state their filtration standard.
Frequently asked questions
Is a cloth face covering enough?
No. Cloth face coverings are not designed to filter the tiny airborne particles that include fungal spores.
Is FFP3 better than FFP2?
Yes. FFP3 provides a higher level of filtration, although a well-fitting FFP2 respirator offers good protection for many situations.
Can I reuse disposable masks?
Disposable respirators are designed for limited use. Replace them if they become damp, damaged, dirty or difficult to breathe through. Always follow the manufacturer’s instructions.
Should I wear eye protection?
Most people do not need goggles for routine gardening. However, eye protection may be sensible if working in very dusty environments or using power tools.
When should I seek medical advice?
Contact your healthcare team if:
- your respiratory symptoms worsen after heavy mould exposure
- you develop increasing breathlessness, fever or persistent cough
- you notice coughing up blood
- your asthma becomes more difficult to control
- you are unsure whether your work or hobbies are exposing you to excessive mould
Further information
- NHS: Aspergillosis
- Health and Safety Executive: Respiratory Protective Equipment
- Health and Safety Executive: Face fit testing basics
- UKHSA: Damp and mould health risks

Understanding Antibiotics: A Guide for People Living with Aspergillosis and Bronchiectasis
Antibiotics are among the most important medicines used to treat bacterial infections, yet many people living with aspergillosis and bronchiectasis receive repeated courses without ever having their purpose fully explained. This guide explains why antibiotics are prescribed, how doctors choose them, why resistance matters, what side effects and interactions to watch for, and how future treatments may become faster and more precise.
Key points
- Antibiotics treat bacterial infections. They do not treat Aspergillus, which is a fungus.
- Many people with aspergillosis also have bronchiectasis, asthma, COPD or damaged airways, making bacterial infections more likely.
- The “strongest” antibiotic is not always the best choice. Doctors usually aim to use the antibiotic that is most likely to work while causing the least unnecessary harm.
- Sputum samples help identify which bacteria are present and which antibiotics are likely to work.
- Antibiotic resistance develops in bacteria, not in people.
- Side effects, allergies, kidney and liver function, and drug interactions all influence antibiotic choice.
- People taking antifungal medicines should always tell their doctor or pharmacist before starting antibiotics.
- The future of infection treatment is likely to involve faster diagnostics, more targeted antibiotics, sequencing, AI, vaccines and other precision approaches.
1. Why this guide?
Many people living with aspergillosis are prescribed antibiotics at some point. Some receive occasional short courses, while others need antibiotics repeatedly because they also have bronchiectasis, COPD, asthma, recurrent chest infections or other lung conditions.
Many patients tell us that they have taken antibiotics for years but have never had the opportunity to understand why different antibiotics are chosen, why some are changed, why others are avoided, or how these decisions are made. This guide aims to answer those questions.
Antibiotics can be very important medicines. They can treat bacterial infections, prevent serious complications and help people recover from a worsening chest condition. However, they can also cause side effects, interact with other medicines, disturb the microbiome and contribute to antibiotic resistance if they are used when they are not needed.
Key message
Antibiotics treat bacterial infections. They do not treat Aspergillus itself. Aspergillosis is caused by a fungus and requires antifungal treatment when active treatment is needed.
The aim of this guide is not to help people choose antibiotics for themselves. Antibiotics should always be prescribed by a qualified healthcare professional who understands your medical history, test results, allergies, current medicines and local prescribing guidance.
Instead, this guide aims to help you have better conversations with your healthcare team. Understanding why decisions are made can make treatment feel less confusing and help you share information that may be important, such as previous sputum results, antibiotics that have helped before, side effects you have experienced, or medicines that might interact.
If you are unwell, coughing up blood, becoming more breathless, developing chest pain, confused, drowsy, feverish or rapidly deteriorating, seek urgent medical advice. This guide is for general education and should not replace individual medical care.
2. Why do people with aspergillosis need antibiotics?
One of the most common questions people ask is:
“If aspergillosis is caused by a fungus, why am I taking antibiotics?”
The answer is that many people living with aspergillosis also develop bacterial chest infections. These infections require antibiotics because antibiotics treat bacteria, not fungi.
Although aspergillosis itself is caused by the Aspergillus fungus, it often occurs alongside other lung conditions that make bacterial infections more likely. This means it is not unusual for someone to receive antifungal medication at one time and antibiotics at another, or occasionally both at the same time.
Bacteria, fungi and viruses: what is the difference?
| Type of germ | Examples | Usual treatment approach |
|---|---|---|
| Bacteria | Many chest infections, Haemophilus influenzae, Pseudomonas aeruginosa, Streptococcus pneumoniae | Antibiotics |
| Fungi | Aspergillus, Candida | Antifungal medicines |
| Viruses | Influenza, COVID-19, RSV and many common colds | Usually supportive care, with antiviral medicines for some infections |
This distinction is important because antibiotics do not kill fungi or viruses. Taking an antibiotic will not treat aspergillosis itself.
Why are bacterial infections more common in some people with aspergillosis?
Many people with aspergillosis also have underlying lung conditions that make it easier for bacteria to grow.
Bronchiectasis is a common example. It causes widening and damage to the airways, making it harder for the lungs to clear mucus effectively. When mucus remains in the lungs, bacteria have more opportunity to multiply and cause infection.
Other conditions, such as severe asthma or COPD, can also affect the lungs’ natural defence mechanisms. Previous lung damage, surgery or repeated infections may further increase the risk.
Some medicines used to control inflammation, including corticosteroids, can also reduce the body’s ability to fight infection, although they are often essential parts of treatment.
Can more than one problem happen at the same time?
Yes. This is one reason chest symptoms can be difficult to diagnose and treat.
A person may have:
- aspergillosis that is stable, but a new bacterial chest infection;
- worsening aspergillosis without any bacteria being involved;
- a viral infection that triggers worsening respiratory symptoms;
- or a combination of bacterial, fungal and viral problems occurring together.
Because many of these illnesses produce similar symptoms, including cough, increased sputum, breathlessness and tiredness, your healthcare team may need sputum samples, blood tests or scans to determine what is happening.
Not every flare-up needs antibiotics
When symptoms worsen, it is natural to think that antibiotics are needed. However, this is not always the case.
Breathlessness, increased cough or fatigue may be caused by a bacterial infection, but they may also be caused by a viral infection, a flare-up of aspergillosis, airway inflammation, asthma, allergy or another medical condition.
Choosing the right treatment begins with understanding what is causing the symptoms, rather than simply treating the symptoms themselves.
3. How do doctors decide which antibiotic to prescribe?
Many people are surprised by how much thought goes into choosing an antibiotic. Although several antibiotics may be able to treat the same infection, the best choice depends on much more than simply identifying the bacteria.
Your healthcare professional has to balance a number of factors to select an antibiotic that is both effective and safe for you.
What information does your doctor consider?
Before prescribing an antibiotic, your healthcare team may consider:
- your symptoms and how severe they are;
- whether the infection is likely to be bacterial, viral or fungal;
- your underlying lung conditions, such as bronchiectasis, asthma or COPD;
- previous sputum culture results;
- which bacteria have caused infections in the past;
- which antibiotics have worked well previously;
- which antibiotics have not helped, or have caused side effects;
- any antibiotic allergies;
- your kidney and liver function;
- other medicines you are taking that could interact;
- local antibiotic resistance patterns;
- whether treatment is needed at home or in hospital.
Sometimes doctors have to make their best judgement
Ideally, doctors would know exactly which bacterium is causing an infection before treatment begins. Unfortunately, laboratory cultures usually take at least a day or two, and sometimes longer.
If someone is becoming unwell, waiting several days may not be safe.
Instead, doctors often begin empirical treatment. This means prescribing the antibiotic that is most likely to work based on your symptoms, the bacteria that commonly cause similar infections, your previous microbiology results and local knowledge of antibiotic resistance.
Once sputum culture or other laboratory results become available, treatment can be reviewed. Sometimes the original antibiotic is continued because it is working well. At other times it may be changed to one that is more specifically targeted to the bacteria that have been identified.
Did you know?
Many people start antibiotic treatment before laboratory results are available. This is common medical practice and helps ensure that serious infections are treated promptly while additional information is being collected.
Why don’t two patients receive the same antibiotic?
Two people with similar symptoms may receive different antibiotics.
For example, one person may have previously grown Pseudomonas aeruginosa in their sputum, while another has repeatedly grown Haemophilus influenzae. One may have a penicillin allergy, another may have reduced kidney function, while a third may be taking medicines that interact with certain antibiotics.
The most appropriate antibiotic is therefore highly individual.
Previous infections matter
Your previous microbiology results are often one of the most valuable pieces of information available.
If you have had repeated infections with the same bacterium, your healthcare team may already know which antibiotics usually work well, which have failed previously, whether resistance has developed, and whether your bacteria have become more difficult to treat over time.
This is one reason why specialist clinics often ask about previous sputum results when reviewing your treatment.
4. Broad-spectrum and narrow-spectrum antibiotics
One of the most common misunderstandings about antibiotics is that some are “strong” while others are “weak”. In reality, doctors usually think in terms of broad-spectrum and narrow-spectrum antibiotics rather than strength.
The aim is not to prescribe the most powerful antibiotic available. Instead, it is to choose the antibiotic that is most likely to treat your infection while causing the least unnecessary harm.
What does “broad-spectrum” mean?
Broad-spectrum antibiotics are active against a wide range of different bacteria.
They are particularly useful when the exact bacterium is not yet known, several different bacteria could be responsible, or the infection is serious and treatment cannot safely wait for laboratory results.
Because they affect many different bacteria, broad-spectrum antibiotics may also disturb the body’s normal bacteria more than a narrower-spectrum antibiotic.
What does “narrow-spectrum” mean?
Narrow-spectrum antibiotics are designed to treat a smaller range of bacteria.
Once laboratory tests identify the bacterium causing an infection, doctors often prefer to use a narrow-spectrum antibiotic whenever possible.
This approach helps to treat the infection effectively, reduce unnecessary exposure to antibiotics, protect the body’s normal bacteria and slow the development of antibiotic resistance.
Think of it like gardening
A broad-spectrum antibiotic is a little like using a weedkiller that kills almost every plant in a flower bed. It may solve the immediate problem, but it can also affect plants you wanted to keep.
A narrow-spectrum antibiotic is more like carefully removing only the weed causing the problem. It is a more targeted approach that leaves the surrounding plants largely undisturbed.
Examples of antibiotics commonly used for chest infections
There are many different antibiotics available, and the choice depends on the type of infection, the bacteria involved, previous sputum culture results, allergies, side effects, other medicines you are taking and local prescribing guidance.
The examples below illustrate some antibiotics that people with chronic lung conditions may encounter. They are included to help explain how doctors think about antibiotic selection, not to suggest that one antibiotic is better than another.
| Antibiotic | Common respiratory uses | Spectrum* | Things patients should know |
|---|---|---|---|
| Amoxicillin | Common bacterial chest infections | Relatively narrow | Often an excellent first-choice antibiotic when the likely bacteria are susceptible. |
| Co-amoxiclav | A wider range of respiratory infections | Broad | Covers more bacteria than amoxicillin alone but may cause more digestive side effects in some people. |
| Doxycycline | Many respiratory infections, particularly when penicillin is unsuitable | Broad | Can cause photosensitivity, making skin more sensitive to sunlight. |
| Azithromycin | Long-term prevention of exacerbations in selected people with bronchiectasis | Relatively narrow | Often prescribed for its anti-inflammatory effects as well as its antibacterial activity. It is not suitable for everyone and requires careful monitoring. |
| Ciprofloxacin | Often used when bacteria such as Pseudomonas aeruginosa are present and susceptible | Broad | Usually reserved for specific situations because of concerns about resistance and potentially important side effects. |
*Spectrum is a simplified description. Some antibiotics do not fit neatly into “broad” or “narrow” categories, and the best antibiotic depends on the individual patient and the bacteria causing the infection.
Did you know?
There are many licensed antibiotics, but only a relatively small number are used routinely for most community chest infections. Others are reserved for specific bacteria, resistant infections or hospital use. Protecting these specialist antibiotics is an important part of antimicrobial stewardship.
Why not always prescribe the broadest antibiotic?
It might seem logical to use the antibiotic that kills the greatest number of bacteria, but this is not usually the best approach.
Using unnecessarily broad antibiotics can increase the risk of antibiotic resistance, cause more side effects, disturb the normal bacteria living in the gut and elsewhere in the body, increase the risk of infections such as Clostridioides difficile (C. difficile), and reduce future treatment options if resistant bacteria develop.
For these reasons, doctors aim to use the narrowest effective antibiotic whenever it is safe to do so.
Remember
Doctors do not usually ask, “Which is the strongest antibiotic?” Instead they ask, “Which antibiotic is most likely to treat this infection safely and effectively while causing the least unnecessary harm?”
Can treatment change once test results are available?
Yes. It is quite common for doctors to begin treatment with a broader-spectrum antibiotic while waiting for sputum culture results. Once the laboratory identifies the bacterium and reports which antibiotics are likely to work, treatment may be changed to a more targeted medicine.
This process is known as stepping down or de-escalating antibiotic treatment. It is an important part of good antimicrobial stewardship and helps preserve antibiotics for the future.
5. Why have I been prescribed an antibiotic that didn’t seem to work before?
Many people living with bronchiectasis or aspergillosis have experienced repeated chest infections over many years. It is not unusual to be prescribed the same antibiotic more than once.
This can be frustrating, especially if you remember taking that antibiotic previously and feeling that it made little difference.
“I’ve had this antibiotic before. It never works.”
Although this is an understandable reaction, the situation is often more complicated than it first appears.
The infection may not be the same
Not every chest infection is caused by the same bacterium.
One episode may be caused by one type of bacteria, while the next may involve a completely different organism. Sometimes symptoms are caused by a viral infection, worsening aspergillosis, inflammation or another lung condition rather than bacteria at all.
An antibiotic that was appropriate for one illness may therefore be less suitable for another, or the other way around.
The previous illness may not have been bacterial
Antibiotics only work against bacteria.
If your previous symptoms were caused by a virus, a flare-up of aspergillosis, airway inflammation or another non-bacterial cause, then no antibiotic would have been expected to help very much, regardless of which one was prescribed.
This does not necessarily mean the antibiotic itself was ineffective.
Your doctor may have different information this time
Each consultation is slightly different.
Your doctor may now know which bacteria have previously grown in your sputum, which antibiotics those bacteria were sensitive to, whether resistance has developed, whether you have new medical conditions, or whether your current medicines have changed.
Even if the same antibiotic is prescribed, the decision may be based on new information.
A new doctor may not know your previous experience
If you are seen by an out-of-hours service, an emergency department or a clinician who does not usually look after you, they may not immediately have access to your full treatment history.
They may know that you have a chest infection but not which antibiotics have helped, failed or caused side effects in the past.
Helping your healthcare team
Instead of simply saying, “That antibiotic never works,” it is often more helpful to explain when you last received it, whether you completed the course, whether your symptoms improved at all, whether another antibiotic was eventually needed, whether a sputum sample identified a particular bacterium, and whether you experienced any important side effects.
Sometimes the antibiotic really was not the right one
Doctors are not always able to identify the exact cause of an infection before treatment begins.
Initial antibiotic treatment is often based on experience and the bacteria most likely to be responsible. Occasionally, laboratory results later show that a different antibiotic would be more appropriate.
Changing antibiotics after sputum culture results become available is common and should not be seen as a failure. Instead, it reflects the fact that treatment is being refined as more information becomes available.
Good communication improves future treatment
If you experience repeated chest infections, keeping a simple record of your treatment history can be extremely helpful.
You may wish to note the date of each infection, whether a sputum sample was taken, which bacteria were identified, which antibiotic was prescribed, whether it appeared to help, and any significant side effects.
Many patients find that this information becomes particularly valuable during hospital admissions, emergency appointments or consultations with new healthcare professionals.
6. Why are sputum samples so important?
If you live with bronchiectasis or aspergillosis, your healthcare team may ask you to provide a sputum sample whenever your symptoms worsen.
This can feel inconvenient, particularly if you are coughing more or feel unwell. However, a good sputum sample is often one of the most valuable tools available for identifying the cause of a chest infection and selecting the most appropriate treatment.
What is a sputum sample?
Sputum is the mucus that is coughed up from deep within the lungs. It is different from saliva, which is produced in the mouth.
Because sputum comes from the lower airways, it can contain bacteria, fungi and other organisms that are living in or causing infection within the lungs.
Key message
A sputum sample helps your healthcare team identify what is causing an infection rather than relying only on an educated guess.
What happens to my sample?
Once your sputum reaches the microbiology laboratory, several different tests may be performed depending on your symptoms and medical history.
These may include looking for bacteria that commonly cause chest infections, identifying fungi such as Aspergillus where appropriate, testing which antibiotics are most likely to work against any bacteria that are found, and, in some situations, carrying out specialised molecular tests.
Not every sample receives every test. The investigations performed depend on the clinical information provided by your healthcare team.
What is a culture?
One of the most common laboratory tests is called a culture.
During a culture, the laboratory attempts to grow bacteria or fungi from your sputum under carefully controlled conditions. If organisms grow, they can often be identified and tested against different antibiotics to determine which treatments are most likely to be effective.
This process takes time, which is why laboratory results are usually not available immediately.
What is antibiotic susceptibility testing?
Finding a bacterium is only part of the story.
The laboratory also wants to know which antibiotics are likely to stop it growing.
This process, known as antibiotic susceptibility testing, helps doctors move from an educated guess to a more targeted treatment plan.
Sometimes the results confirm that the antibiotic already prescribed is appropriate. At other times they suggest that a different antibiotic may work better.
Why should I provide a sputum sample before starting antibiotics?
Whenever possible, it is usually best to collect a sputum sample before starting antibiotics.
Once antibiotics have begun to kill bacteria, it can become more difficult for the laboratory to identify exactly which organisms were present.
This does not mean a sample taken later has no value, but early samples often provide the clearest picture.
What if no bacteria are found?
A negative culture does not always mean that nothing is wrong.
There are several possible reasons. The infection may have been caused by a virus, you may already have started antibiotics, the bacteria may be difficult to grow in the laboratory, or your symptoms may be due to worsening aspergillosis or inflammation rather than a bacterial infection.
Your doctor will interpret the laboratory results alongside your symptoms, examination and any imaging studies.
Can my sputum change over time?
Yes. The bacteria living in the lungs can change over months or years. Some may disappear, while others become more common. Occasionally bacteria develop resistance to antibiotics that previously worked well.
For this reason, previous sputum results remain useful, but they do not always predict what is causing your current infection.
Did you know?
A sputum sample does more than identify bacteria. It can also help your healthcare team avoid unnecessary antibiotics, detect resistant organisms, monitor long-term changes and, in some patients, identify fungi or other less common causes of infection.
The future of laboratory testing
Traditional cultures remain extremely important, but laboratory diagnosis is continuing to evolve.
Researchers are developing faster molecular tests that may identify bacteria, fungi and antibiotic resistance genes within hours rather than days. These new technologies are expected to play an increasingly important role in helping doctors prescribe the right antibiotic as quickly as possible.
7. Why don’t doctors always prescribe antibiotics?
Many people expect antibiotics whenever a chest condition worsens. If you have previously benefited from antibiotics, it can be frustrating when a doctor decides that they are not needed this time.
However, not every increase in cough, sputum or breathlessness is caused by a bacterial infection. Prescribing antibiotics when they are unlikely to help exposes you to possible side effects without treating the underlying problem.
Not every flare-up is a bacterial infection
Many different problems can produce similar symptoms.
Increased cough, tiredness or breathlessness may be caused by a bacterial chest infection, a viral infection such as influenza or COVID-19, a flare-up of aspergillosis, increased airway inflammation, poor mucus clearance, an asthma or COPD exacerbation, heart problems or another medical condition.
Key message
Antibiotics only work against bacteria. If your symptoms are caused by something else, an antibiotic is unlikely to help and may expose you to unnecessary risks.
Doctors weigh up the benefits and risks
Every prescription involves balancing potential benefits against possible harms.
Before recommending an antibiotic, your healthcare professional will consider how likely a bacterial infection is, how unwell you are, whether waiting for further information is safe, whether another condition could explain the symptoms, what side effects or drug interactions might occur, and whether you have received several recent courses of antibiotics.
Sometimes the safest decision is to monitor symptoms closely, arrange investigations or review you again rather than prescribing antibiotics immediately.
Antibiotics are not risk-free
Although antibiotics save countless lives, they can also cause unwanted effects.
Depending on the medicine, these may include stomach upset or diarrhoea, allergic reactions, photosensitivity, interactions with other medicines, disturbance of the normal gut microbiome, and encouraging antibiotic-resistant bacteria.
What is a delayed prescription?
Occasionally your doctor may recommend a delayed or “back-up” antibiotic prescription.
This means you are asked to wait for a short period before starting treatment, or only begin the antibiotic if your symptoms worsen or fail to improve.
Delayed prescribing can reduce unnecessary antibiotic use while still ensuring treatment is available if it becomes needed. It is not appropriate for every patient or every infection, but it is one of several approaches doctors may use.
People with chronic lung disease may need a different approach
For people with bronchiectasis or aspergillosis, treatment decisions are often more individual than they are for otherwise healthy adults.
Your respiratory specialist may recommend that you provide a sputum sample at the start of a flare-up, contact your specialist team promptly, keep “rescue antibiotics” at home if this forms part of your agreed care plan, or attend hospital if your symptoms are severe.
Always follow the management plan agreed with your healthcare team, as this will take account of your own medical history and previous infections.
Remember
Choosing not to prescribe antibiotics is an active medical decision, not simply the absence of treatment. Your healthcare professional may recommend monitoring, investigations or a different treatment because they believe this is the safest and most appropriate approach.
Knowing when to seek urgent medical advice
Although not every flare-up requires antibiotics, some symptoms should never be ignored.
Seek urgent medical advice if you develop significant or increasing breathlessness, persistent high fever or rigors, confusion or increasing drowsiness, new chest pain, large amounts of blood when coughing, or rapidly worsening symptoms.
If you are unsure, contact your healthcare team or seek urgent medical assessment.
8. Side effects: what should I watch for?
Like all medicines, antibiotics can cause side effects. Fortunately, most people complete a course without experiencing any serious problems. Many side effects are mild, temporary and disappear once treatment has finished.
However, every antibiotic has its own pattern of possible side effects, which is one reason your healthcare professional carefully considers which medicine is most appropriate for you.
Key message
Most side effects are mild and manageable, but it is important to know which symptoms are expected, which should be reported to your healthcare team, and which require urgent medical attention.
Common side effects
The most frequently reported side effects include nausea, stomach discomfort, diarrhoea, loss of appetite, metallic or altered taste, and thrush affecting the mouth or vagina.
These symptoms are usually temporary and improve after the antibiotic has been completed.
Photosensitivity: when sunlight becomes a problem
Some antibiotics, including doxycycline, can make your skin much more sensitive to sunlight and ultraviolet light. This is known as photosensitivity.
People affected may develop severe sunburn much more quickly than usual, even after relatively short periods outdoors.
This is not only relevant on holiday or during hot weather. Some people may burn more easily while gardening, walking the dog, sitting near strong sunlight, driving, or spending time outdoors on a bright day.
While taking medicines that cause photosensitivity it is sensible to avoid prolonged exposure to strong sunlight, wear protective clothing and a wide-brimmed hat if outdoors, use a broad-spectrum sunscreen with a high SPF, and avoid sunbeds.
If you develop an unusually severe skin reaction after sun exposure, contact your healthcare professional.
Allergic reactions
Some people are allergic to particular antibiotics, especially those in the penicillin family.
Symptoms may include a widespread itchy rash, swelling of the lips, tongue or face, difficulty breathing, wheezing, collapse or feeling faint.
Severe allergic reactions, also known as anaphylaxis, are medical emergencies and require immediate emergency treatment.
Looking after your gut
Antibiotics do not distinguish between harmful bacteria causing an infection and many of the helpful bacteria that naturally live in the gut.
As a result, some people develop diarrhoea or other digestive symptoms during treatment.
Most people recover naturally after finishing their antibiotics as their normal gut bacteria gradually re-establish themselves.
Other important side effects
Although less common, some antibiotics have specific side effects that your healthcare professional may discuss with you.
Examples include tendon inflammation or rupture with some fluoroquinolone antibiotics, hearing or balance problems with certain intravenous antibiotics, effects on kidney function, effects on liver function, and changes in heart rhythm with some medicines.
These problems are uncommon, but they illustrate why different antibiotics are chosen carefully for different patients.
Why does my doctor ask about previous side effects?
If you have experienced troublesome side effects before, it is important to tell your healthcare professional.
For example, if you previously developed severe diarrhoea, a significant skin reaction or marked photosensitivity while taking a particular antibiotic, your doctor may choose a different treatment if a suitable alternative is available.
Keeping a personal record of important side effects can be extremely helpful, particularly if you receive care from several different healthcare providers.
When should I seek medical advice?
Contact your healthcare team promptly if you develop persistent or severe diarrhoea, a widespread rash, yellowing of the skin or eyes, new hearing problems, severe dizziness, pain or swelling in a tendon, or any side effect that concerns you.
Seek emergency medical help immediately if you develop swelling of the face or throat, severe difficulty breathing or symptoms of anaphylaxis.
9. Drug interactions: why does my doctor need to know about every medicine I take?
People living with aspergillosis often take several medicines at the same time. These may include antifungal medicines, inhalers, corticosteroids, treatments for asthma or bronchiectasis, blood pressure tablets, blood thinners and medicines for other long-term conditions.
When a new antibiotic is prescribed, your healthcare professional will usually check whether it could interact with any of your existing medicines.
Most interactions can be avoided simply by choosing a different antibiotic or by monitoring treatment more closely.
Key message
Always tell your doctor, nurse or pharmacist about every medicine you take, including inhalers, over-the-counter medicines, vitamins, herbal remedies and dietary supplements.
What is a drug interaction?
A drug interaction occurs when one medicine changes the way another medicine works.
An interaction may make one medicine less effective, increase the chance of side effects, increase or decrease the amount of a medicine in the bloodstream, or require additional monitoring during treatment.
Not every combination causes problems, but checking for interactions is an important part of safe prescribing.
Why is this particularly important in aspergillosis?
Many people with aspergillosis receive antifungal medicines such as itraconazole, voriconazole, posaconazole or isavuconazole.
These medicines can be highly effective, but they are also well known for interacting with a wide range of other drugs.
Before prescribing an antibiotic, your healthcare professional may therefore review your current medicines to make sure the combination is appropriate.
Other medicines that may interact
Depending on the antibiotic being prescribed, your healthcare professional may also consider interactions with corticosteroids, blood-thinning medicines, heart rhythm medicines, diabetes treatments, anti-epileptic medicines, some cholesterol-lowering medicines, certain antidepressants and biological therapies used for severe asthma.
This does not mean these medicines cannot be used together. In many cases they can, but careful selection and monitoring are important.
Timing can also matter
Some medicines can reduce how well an antibiotic is absorbed.
For example, certain antibiotics should not be taken at exactly the same time as calcium supplements, iron tablets, magnesium-containing indigestion remedies or zinc supplements.
Your pharmacist or healthcare professional will advise you if medicines need to be separated by a few hours.
Don’t forget non-prescription medicines
Many people assume that only prescription medicines matter.
However, over-the-counter medicines, herbal preparations and food supplements can also interact with prescription medicines.
Always mention anything you are taking, even if you bought it yourself or only use it occasionally.
Did you know?
Community pharmacists routinely check for many potential drug interactions before dispensing medicines. They are an excellent source of advice if you are unsure whether medicines can safely be taken together.
Keeping an accurate medicines list
If you have a chronic lung condition, one of the most useful things you can do is keep an up-to-date medicines list.
This should include prescription medicines, inhalers, antifungal medicines, regular antibiotics, rescue medicines, vitamins and supplements, and any known drug allergies or important side effects.
Having this information available can be particularly helpful if you are admitted to hospital, attend an emergency department or see a healthcare professional who is unfamiliar with your medical history.
Further information
Aspergillosis.org has detailed guides covering antifungal medicines and their interactions. If you take an antifungal medicine, these resources provide more detailed information about specific drug combinations and precautions.
10. Antibiotics and the microbiome
Over the past decade, scientists have become increasingly interested in the microbiome: the enormous community of bacteria, fungi and other microorganisms that naturally live in and on our bodies.
Most of these organisms are harmless and many play an important role in maintaining health. They help digest food, produce vitamins, support the immune system and compete with potentially harmful microbes.
Antibiotics are designed to kill disease-causing bacteria, but they can also affect many helpful bacteria at the same time.
Key message
Antibiotics save lives and remain one of the greatest advances in modern medicine. However, researchers are learning that they may also temporarily alter the body’s normal microbiome. Understanding these changes is helping doctors use antibiotics more wisely.
What is the microbiome?
Your body is home to trillions of microorganisms. These communities are found in many places, including the gut, mouth, skin, nose and lungs.
Together they form your microbiome. Although invisible, these microorganisms are an important part of normal human biology.
How do antibiotics affect the microbiome?
Because antibiotics cannot always distinguish between harmful and helpful bacteria, they may reduce the numbers of beneficial bacteria as well as those causing an infection.
This helps explain why some people experience diarrhoea, changes in bowel habit, thrush or digestive discomfort during or shortly after antibiotic treatment.
For most people, the microbiome gradually recovers after treatment has finished, although recovery may take time and varies between individuals.
Why are researchers so interested?
Scientists are now investigating whether the microbiome influences many aspects of health, including immunity, inflammation and susceptibility to infection.
This is an exciting area of research, but many questions remain unanswered.
Researchers are still working to understand which changes are temporary, which are important for long-term health, how repeated antibiotic courses affect the microbiome, and whether it is possible to protect beneficial bacteria while still treating infection effectively.
The microbiome has become an area of intense research, but scientists are still learning which changes are important and how they influence long-term health.
What about people with chronic lung disease?
People living with bronchiectasis and aspergillosis may receive repeated courses of antibiotics over many years.
Researchers are therefore particularly interested in understanding how long-term antibiotic treatment influences both the gut microbiome and the community of microorganisms living within the airways, sometimes called the lung microbiome.
This research may help explain why some people experience repeated infections while others remain relatively stable, although many questions have yet to be answered.
Should I take probiotics?
This is one of the questions patients ask most often.
Some studies suggest that certain probiotics may reduce the risk of antibiotic-associated diarrhoea in some people. However, not every probiotic is the same, and research is continuing to determine which products are beneficial, who is most likely to benefit, and when they should be used.
For most people, eating a balanced diet that supports general health is more important than taking a particular probiotic supplement.
If you have a weakened immune system or are receiving specialist treatment, speak to your healthcare team before taking probiotic products, as they may not be suitable for everyone.
Be cautious of marketing claims
Many products are marketed as “microbiome boosters”, “gut health” supplements or “immune support” products. Some may be harmless, but the quality of evidence varies. Be especially cautious about products that claim to prevent infection, replace medical treatment or “repair” the microbiome quickly.
The future
As our understanding of the microbiome grows, it is likely to influence how antibiotics are developed and prescribed.
Future treatments may become increasingly personalised, helping doctors choose therapies that not only treat infection effectively but also preserve the beneficial microorganisms that contribute to long-term health.
11. Antibiotic resistance: why does it matter?
Antibiotic resistance has become one of the greatest challenges facing modern medicine. Around the world, doctors are seeing increasing numbers of bacteria that have become difficult, or sometimes impossible, to treat using antibiotics that once worked well.
This does not mean antibiotics are no longer effective. Most bacterial infections can still be treated successfully. However, preserving these medicines for the future requires careful use by healthcare professionals, patients, researchers and governments alike.
Key message
People do not become resistant to antibiotics. Bacteria do. Antibiotic resistance develops when bacteria change over time, making some antibiotics less effective against them.
How does antibiotic resistance develop?
Bacteria multiply very quickly.
Occasionally, random genetic changes occur that help some bacteria survive exposure to a particular antibiotic. When antibiotics are used, these resistant bacteria may survive while more susceptible bacteria are killed.
The resistant bacteria can then continue to multiply and, in some cases, spread to other people.
This is a natural process driven by evolution, but the more antibiotics are used, the greater the opportunity for resistant bacteria to be selected.
Why does this matter to me?
If you have a chronic lung condition, antibiotics may be an important part of your treatment throughout your life.
Preserving effective antibiotics is therefore not just a global issue. It is also a personal one.
If bacteria become resistant to commonly used antibiotics, treatment options may become more limited, and future infections may be more difficult to manage.
What is antimicrobial stewardship?
You may hear healthcare professionals talk about antimicrobial stewardship.
This means using antibiotics, antifungals and other antimicrobial medicines carefully and responsibly so that they remain effective for as long as possible.
Antimicrobial stewardship is about giving every patient the treatment they need, not denying treatment to reduce costs.
Good antimicrobial stewardship aims to treat infections promptly and effectively, avoid antibiotics when they are unlikely to help, choose the most appropriate antibiotic, use the correct dose and duration, change to a more targeted antibiotic when laboratory results become available, and reduce the development of antibiotic resistance.
Did you know?
Many hospitals have specialist antimicrobial stewardship teams made up of doctors, pharmacists, microbiologists and infection specialists who work together to ensure antibiotics are used as safely and effectively as possible.
Can patients help?
Absolutely.
You can support good antibiotic stewardship by taking antibiotics exactly as prescribed, providing sputum samples before starting treatment whenever possible, not sharing antibiotics with other people, not keeping leftover antibiotics for future illnesses unless specifically advised as part of your agreed care plan, telling your healthcare team if treatment is not working or if you develop side effects, and keeping an accurate record of previous infections and treatments.
These simple steps help your healthcare team make the best possible treatment decisions.
Are new antibiotics being developed?
Yes, but developing new antibiotics is difficult, expensive and time-consuming.
Unlike many other medicines, antibiotics are usually taken for only a short period, making them less commercially attractive to develop. At the same time, bacteria continually evolve, meaning new medicines may eventually encounter resistance as well.
This is one reason why preserving the antibiotics we already have remains so important.
Resistance is only part of the solution
Modern medicine is increasingly looking beyond simply developing stronger antibiotics.
Researchers are also working on faster diagnostic tests, rapid identification of resistance genes, vaccines that prevent bacterial infections, new ways of targeting bacteria more precisely, and treatments that reduce the need for antibiotics altogether.
The goal is not only to develop new medicines but also to ensure that every patient receives the right antibiotic, at the right time, for the right infection.
12. The future of treating infections
Antibiotics have transformed medicine over the past 80 years, saving millions of lives and making many modern medical treatments possible. Although antibiotic resistance presents a significant challenge, there are many reasons to be optimistic about the future.
Researchers around the world are developing new antibiotics, faster diagnostic tests and entirely new ways of preventing and treating infections. The aim is not simply to find “stronger” antibiotics, but to ensure that every patient receives the right treatment at the right time.
Key message
The future of infection treatment is becoming more precise, personalised and evidence-based. Better diagnostics may be just as important as new antibiotics in improving patient care.
Faster diagnosis
One of the biggest changes is likely to be how quickly infections can be identified.
Traditional laboratory cultures remain extremely important, but they can take several days to provide complete results.
New molecular techniques, including PCR and genetic sequencing, are increasingly able to identify bacteria, fungi and important resistance genes much more quickly. In the future, doctors may be able to select the most appropriate treatment within hours rather than days.
This is particularly exciting for people with chronic lung disease, where identifying the cause of an infection quickly may help avoid unnecessary antibiotics and improve outcomes.
New antibiotics
Although developing new antibiotics is scientifically challenging, research continues around the world.
Many newer antibiotics are being designed to treat bacteria that have become resistant to older medicines, particularly those responsible for serious hospital-acquired infections.
However, researchers recognise that simply developing new antibiotics is not enough. Every new antibiotic must also be protected through careful prescribing so that it remains effective for as long as possible.
Precision medicine
Instead of treating every patient in the same way, doctors increasingly aim to tailor treatment to the individual.
Future decisions may take account of the exact bacteria causing the infection, their resistance profile, your previous microbiology results, your underlying lung disease, your medicines and possible drug interactions, and even your own microbiome.
This personalised approach aims to improve treatment while reducing unnecessary antibiotic exposure.
Artificial intelligence
Artificial intelligence may assist researchers and healthcare professionals in several areas of infection management.
Potential future applications include interpreting laboratory results more rapidly, predicting antibiotic resistance, helping clinicians select the most appropriate treatment, and identifying patients at greatest risk of severe infection.
AI is expected to support, not replace, the judgement of experienced healthcare professionals.
Bacteriophage therapy
One of the most fascinating areas of research involves bacteriophages, often shortened to phages.
These are naturally occurring viruses that infect bacteria rather than people.
Scientists are investigating whether carefully selected phages could be used to treat some infections that no longer respond well to conventional antibiotics. Although phage therapy is not yet routine clinical practice, it offers exciting possibilities for the future.
Vaccines and prevention
Perhaps the best way to reduce antibiotic use is to prevent infections from occurring in the first place.
Vaccination programmes, improved infection prevention, better management of chronic lung disease and healthier lifestyles all contribute to reducing the need for antibiotics.
For people living with aspergillosis, measures such as airway clearance, prompt investigation of new symptoms and regular follow-up with their healthcare team may also help reduce the impact of recurrent infections.
Protecting the microbiome
Researchers are also exploring ways of treating infections while causing less disruption to the body’s normal bacteria.
Future antibiotics may become much more selective, targeting harmful bacteria while preserving beneficial microorganisms that support normal health.
This could reduce side effects and help maintain a healthier microbiome during treatment.
Looking to the future
Although headlines often focus on antibiotic resistance, the wider picture is encouraging. Advances in diagnostics, genomics, microbiology, infection prevention and new antimicrobial therapies are changing the way infections are managed. For people living with aspergillosis and bronchiectasis, these developments offer real hope that future treatment will become faster, more targeted and increasingly personalised.
13. Five practical things patients can do
Understanding antibiotics does not mean choosing treatment for yourself. It means being better prepared to work with your healthcare team.
- Provide sputum samples early when your healthcare team asks for them, ideally before starting antibiotics if this is safe and practical.
- Keep a record of previous antibiotics, sputum results, side effects and which treatments seemed to help.
- Tell your doctor and pharmacist about all medicines, including antifungals, inhalers, over-the-counter medicines and supplements.
- Take antibiotics exactly as prescribed and ask for advice if you are unsure what to do.
- Seek medical advice promptly if symptoms worsen, side effects are severe, or you develop warning signs such as increasing breathlessness, chest pain, confusion or coughing up significant amounts of blood.
A final thought
Antibiotics remain one of the greatest achievements in modern medicine. They have saved countless lives and continue to play a vital role in treating bacterial infections.
For people living with aspergillosis and bronchiectasis, antibiotics may be an important part of care, but they need to be used thoughtfully. The best antibiotic is not always the broadest or newest medicine. It is the one that is most likely to treat the infection safely, effectively and with the least unnecessary harm.
Understanding how antibiotics are chosen, why they are used carefully and how research is shaping the future can help patients become informed partners in their own care. By working together, patients and healthcare professionals can help ensure that these remarkable medicines remain effective for future generations.
Internal Links
Consider linking to:
- Antifungal medicines
- Bronchiectasis Knowledge Hub
- Sputum sampling
- Understanding sputum cultures
- Antimicrobial stewardship
- Drug interactions
- Photosensitivity with antibiotics
- Living with bronchiectasis
- Pseudomonas infections
- When to seek urgent medical advice
External References
Useful authoritative resources include:
- NHS guidance on antibiotics
- UK Health Security Agency information on antimicrobial resistance
- National Institute for Health and Care Excellence antimicrobial prescribing guidance
- World Health Organization resources on antimicrobial resistance
Weekly Aspergillosis Research Update: COPD IPA Criteria, CPA Serology, ICU Galactomannan and Environmental Prevention
Week ending 6 July 2026
Overall summary
This week’s strongest theme is improved recognition and interpretation of Aspergillus disease in high-risk respiratory and immunocompromised patients.
The headline paper proposes COPD-specific diagnostic criteria for invasive pulmonary aspergillosis (IPA), addressing a long-standing gap between classic immunocompromised-host definitions and real-world respiratory practice. Other important papers focus on chronic pulmonary aspergillosis (CPA) serology, bronchoalveolar lavage galactomannan stewardship, endotracheal aspirate galactomannan in ICU patients, and environmental prevention of invasive fungal disease in paediatric cancer care.
Overall, this is a week of cautious progress: better criteria, better test interpretation, and better diagnostic systems — but several findings still require prospective validation.
High priority
Diagnostic criteria for invasive pulmonary aspergillosis in COPD patients
Denning DW, Rogers TR, Takazono T, Su X, Lagrou K, White PL, James DA, Bafadhel M, Lopez JB, Bulpa P, Chotirmall SH, et al.
American Journal of Respiratory and Critical Care Medicine. Published 1 July 2026.
DOI: 10.1093/ajrccm/aamag310
PMID: 42384914
This is the likely headline paper of the week. It proposes COPD-specific diagnostic criteria for IPA in non-ventilated hospitalised patients with COPD exacerbations. The criteria focus on patients with a hospitalised exacerbation plus at least two risk factors, such as systemic or high-dose inhaled corticosteroids, bronchiectasis, diabetes, cardiovascular disease, or prolonged antibiotic exposure.
Recommended investigation includes CT chest imaging, respiratory fungal microscopy and culture, preferably Aspergillus PCR, BAL or bronchoscopy galactomannan where available, serum galactomannan, and Aspergillus IgG. Diagnosis is supported by the combination of a high-risk COPD patient, compatible imaging, and any two positive Aspergillus tests, either from different samples or from different tests on the same respiratory sample.
Why it matters: COPD patients with IPA often do not fit classic EORTC/MSGERC host-factor definitions, which are strongest for haematology and transplant populations. This paper provides a respiratory-focused framework for a group in whom IPA may be missed, diagnosed late, or dismissed as colonisation.
Clinical or diagnostic relevance: The criteria could help respiratory teams investigate hospitalised COPD patients who deteriorate unexpectedly or fail to respond to standard treatment. They may encourage earlier CT imaging and broader fungal testing rather than relying on a single sputum culture.
Limitations / cautions: These are proposed consensus criteria based on literature review and Delphi methodology, not externally validated diagnostic criteria. Further studies are needed to validate them and to improve performance data for fungal assays in COPD. There remains a risk of overdiagnosis from colonisation and underdiagnosis where good respiratory samples or bronchoscopy are unavailable.
Diagnostic performance of IgG against multiplex Aspergillus antigens (mx4) for identifying chronic pulmonary aspergillosis
Sehgal IS, Agarwal R, Muthu V, Prasad KT, Dhooria S, Singh M, Rudramurthy SM, Aggarwal AN, Garg M, Chakrabarti A.
Medical Mycology. Published 2 July 2026.
DOI: 10.1093/mmy/myag071
PMID: 42392187
This prospective diagnostic study compared a multiplex Aspergillus IgG assay, mx4-IgG, with standard A. fumigatus-IgG for diagnosing CPA. The mx4 antigen preparation includes extracts of A. fumigatus, A. flavus, A. niger, and A. terreus. Among 332 adults with suspected CPA, 230 had CPA and 102 were diseased controls with structural lung disease.
Against the primary reference standard, mx4-IgG had sensitivity of 83.0% and specificity of 73.5%, compared with 95.2% and 88.2% for A. fumigatus-IgG.
Why it matters: The study tests an attractive idea: that broader multiplex Aspergillus antigen testing might improve CPA diagnosis. However, the results suggest that mx4-IgG was not superior to standard A. fumigatus-IgG.
Clinical or diagnostic relevance: A. fumigatus-IgG should remain the first-line serological test for CPA based on these findings. A practical finding was that a hierarchical strategy using A. fumigatus-IgG followed by A. flavus-IgG identified 97.7% of CPA cases at the lowest reported cost, USD 24 per patient, and outperformed strategies incorporating mx4.
Limitations / cautions: This was a tertiary chest-clinic cohort with high CPA prevalence, so predictive values may differ in lower-prevalence settings. The abstract does not provide confidence intervals, ROC values, or detailed subgroup data. The subgroup most likely to benefit from A. flavus-IgG requires full-text review.
Medium priority
The clinical utility of bronchoalveolar lavage galactomannan result stewardship within a tertiary medical system
Apostolopoulou A, Hammond SP, Turbett SE, Fishman JA.
Medical Mycology. Published 1 July 2026.
DOI: 10.1093/mmy/myag069
PMID: 42384022
This retrospective quality-improvement study examined stewardship of elevated BAL galactomannan results in a tertiary medical system. The Transplant Infectious Disease team monitored all elevated BAL GM results and, 24 hours after a positive result, sent a standardised email to the primary team if the result appeared unaddressed in the clinical documentation.
Among 55 cases with BAL GM >1.0, 17 cases (31%) had antifungal therapy started after a single positive BAL GM result. The stewardship team contacted primary teams in 14 cases (25%), leading to a new start or change in antifungal therapy.
Why it matters: Fungal diagnostics are only useful if results are recognised and interpreted correctly. This paper highlights a practical gap in BAL GM interpretation and shows how specialist result stewardship may help close the loop.
Clinical or diagnostic relevance: The intervention is highly practical: monitor positive BAL GM results, check whether they have been acknowledged, and provide specialist infectious diseases or mycology input where needed. This could be relevant to transplant, haematology, ICU, and tertiary respiratory services.
Limitations / cautions: The study is small, retrospective, and a quality-improvement evaluation rather than a controlled before-and-after study. It shows that stewardship influenced management, but it does not prove improved survival, reduced harm, or reduced inappropriate antifungal prescribing.
Diagnostic utility of endotracheal aspirate galactomannan for invasive pulmonary aspergillosis in ICU patients
Kumar R, Gupta A, Kumar A, Rao Kordcal S, Baitha U, Singh G, Xess I, Madan K, Soneja M, Wig N.
medRxiv preprint. Published 1 July 2026.
DOI: 10.64898/2026.06.29.26356826
PPR: PPR1271604
This prospective observational cohort study assessed endotracheal aspirate galactomannan as a supportive diagnostic test for IPA in mechanically ventilated ICU patients. The study enrolled 120 medicine ICU patients in India, aged over 14 years and ventilated for more than 48 hours, meeting BM-AspICU entry criteria.
Forty-four patients (37%) were classified as probable IPA and 76 as colonisers or possible IPA. The optimal ETA GM cut-off was 1.097, giving sensitivity of 72.73%, specificity of 84.2%, positive likelihood ratio of 4.86, negative likelihood ratio of 0.35, and AUC of 0.844.
Why it matters: ETA sampling is less invasive and easier than bronchoscopy or BAL in ventilated ICU patients. A useful ETA GM test could support earlier recognition of IPA where BAL is unsafe, delayed, or unavailable.
Clinical or diagnostic relevance: ETA GM may be useful as an adjunct or triage tool in ventilated ICU patients with suspected IPA. A positive result may increase suspicion, but a negative result should not exclude disease.
Limitations / cautions: This is a preprint and may not yet have been peer reviewed. It is single-centre and uses a clinical classification reference standard rather than a perfect gold standard. ETA samples are vulnerable to the colonisation-versus-invasion problem, and the proposed cut-off needs external validation.
The underestimated role of environmental factors in the prevention of invasive fungal disease: experience from a European childhood cancer centre
Malvestiti S, Andresen F, Hufnagel M, Speckmann C, Strahm B, Feuchtinger T, Puzik A.
Mycoses. Published 1 July 2026.
DOI: 10.1111/myc.70204
PMID: 42367057
This retrospective single-centre before-and-after study examined invasive fungal disease incidence in high-risk paediatric cancer and transplant patients before and after relocation from an older 1990s building to a new facility with improved environmental protection standards. The study included 186 patients: 140 before relocation and 46 after relocation.
Antifungal prophylaxis followed local standards throughout, with adherence above 98%. Invasive fungal disease incidence fell from 25 cases in the older building (17.9%) to no cases after relocation (p=0.002). Most cases were pulmonary aspergillosis and occurred in HSCT recipients.
Why it matters: The study highlights environmental protection as an under-recognised component of fungal disease prevention. Pharmacological prophylaxis is important, but building design, air quality, and environmental controls may also strongly influence risk.
Clinical or diagnostic relevance: The findings are relevant to paediatric oncology, HSCT, adult haematology, transplant units, and hospitals undergoing refurbishment or ward relocation. Environmental protection should be part of fungal infection prevention planning.
Limitations / cautions: This is observational, retrospective, and single-centre. The post-relocation period was shorter than the pre-relocation period, and the post-relocation cohort was smaller. The abstract does not list the specific environmental measures, so the reduction should be interpreted as being associated with a prevention bundle rather than any single intervention.
Lower priority
Combination antifungal therapy and formulary optimization for progressive invasive pulmonary aspergillosis in a pediatric patient with acute myeloid leukemia: a case report
Khamis F, Al Busaidi A, Al Bahrani K, Al-Rashdi A.
Clinical Case Reports. Published 1 July 2026.
DOI: 10.1002/ccr3.73041
PMID: 42389035
This case report describes a paediatric AML patient with progressive or refractory IPA. Radiological improvement followed combination antifungal therapy and a switch to brand-name liposomal amphotericin B. The authors suggest that refractory IPA management may require attention not only to antifungal class escalation but also to formulation choice and individualised optimisation.
Why it matters: The case raises a practical stewardship issue: when IPA progresses despite apparently appropriate therapy, clinicians should reassess drug exposure, formulation, host immune recovery, resistance, drug interactions, and combination strategy.
Clinical or diagnostic relevance: This is most relevant to paediatric haemato-oncology, AML, prolonged neutropenia, refractory IPA, and formulary decisions.
Limitations / cautions: This is a single case report and should be treated as hypothesis-generating only. It does not prove superiority of one amphotericin formulation over another. Improvement could reflect combination therapy, immune recovery, timing, supportive care, or other factors.
What to highlight this week
- The COPD IPA diagnostic criteria paper is the headline item. It addresses a major diagnostic gap in respiratory practice, but should be described as a proposed consensus framework requiring prospective validation.
- The CPA serology study is an important negative study. Broader multiplex IgG testing was not better than standard A. fumigatus-IgG. The practical message is to keep A. fumigatus-IgG first-line while considering whether targeted reflex A. flavus-IgG deserves further evaluation in selected settings.
- BAL galactomannan stewardship offers a clear implementation message. Fungal diagnostics need interpretation pathways, not just laboratory reporting. A positive fungal biomarker should trigger documented clinical review.
- Endotracheal aspirate galactomannan in ICU patients is promising but not practice-changing yet. ETA GM may help where BAL is difficult, but results must be interpreted alongside clinical, radiological, and microbiological evidence.
- Environmental protection may substantially reduce invasive fungal disease risk in paediatric cancer and HSCT settings. However, the evidence is observational and bundled, so individual protective measures cannot be credited from the abstract alone.
- The paediatric AML case report is clinically thought-provoking but low-level evidence. It is best mentioned briefly as a reminder to reassess drug exposure, formulation, resistance, immune status, and combination strategy in refractory IPA.
Evidence note
This update is based on available evidence notes and abstracts for some papers. Full-text review may refine details, especially around methodology, subgroup findings, confidence intervals, and implementation implications.