
Artificial Intelligence (AI) in the NHS: Promise, Progress and the Future of Healthcare
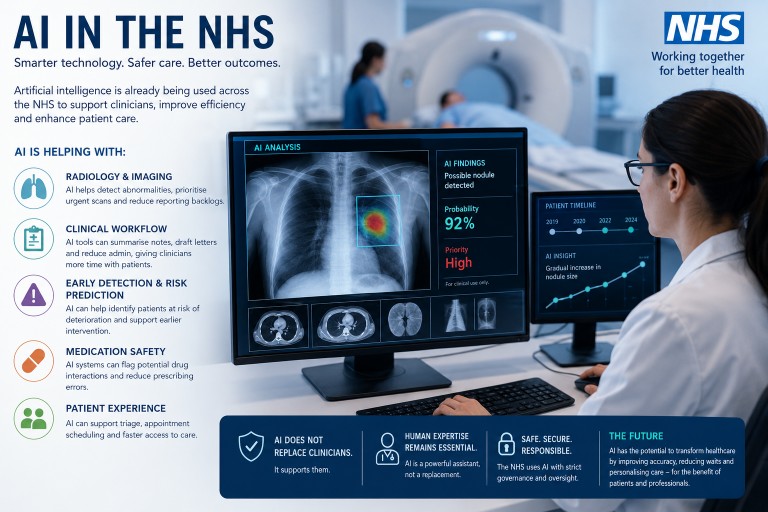
Artificial intelligence (AI) is no longer a futuristic idea within the NHS. AI technologies are already being used in some areas of healthcare across the UK, particularly in radiology, diagnostics, administration and workflow support. However, the reality is more nuanced than many headlines suggest.
At present, AI in the NHS is best understood as a collection of promising technologies being introduced gradually, cautiously and under clinical oversight. Some NHS trusts are using several AI-assisted systems routinely, while others have little or no operational AI deployment beyond pilot projects.
The direction of travel is clear: AI is likely to become an increasingly important part of healthcare over the next decade. However, the NHS is moving carefully because healthcare is a high-risk environment where mistakes can have serious consequences.
What Does AI Mean in Healthcare?
In healthcare, AI usually refers to computer systems that can analyse large amounts of data and identify patterns more quickly or consistently than humans alone.
Examples include:
- Analysing medical scans
- Helping detect cancers or fractures
- Supporting diagnosis
- Summarising clinic consultations
- Reducing paperwork
- Predicting patient deterioration
- Helping prioritise urgent cases
- Supporting medication safety checks
Importantly, most NHS AI systems are currently designed to support clinicians rather than replace them.
AI in NHS Radiology
Radiology is currently one of the biggest areas of AI development within the NHS.
AI systems are being used or trialled to help analyse:
- Chest X-rays
- CT scans
- MRI scans
- Mammograms
- Retinal photographs
- Dermatology images
AI is particularly attractive in radiology because the NHS faces:
- Large radiologist shortages
- Increasing imaging demand
- Growing reporting backlogs
- Rising complexity of scans
How AI Is Currently Used
Most NHS radiology AI systems currently operate in one of three ways:
1. AI as a “Second Reader”
The scan is interpreted by a radiologist, while AI acts as an additional safety check.
AI may flag:
- Possible lung nodules
- Fractures
- Brain bleeds
- Abnormal mammograms
- Signs of stroke
The human clinician still makes the final decision.
2. Prioritisation (“Triage”)
AI can rapidly review scans and move potentially urgent cases higher in the reporting queue.
This may help speed up treatment for:
- Stroke
- Pulmonary embolism
- Pneumothorax (collapsed lung)
- Intracranial bleeding
3. Identifying Likely Normal Scans
Some AI systems are being studied to identify scans that appear very likely to be normal.
The aim is to allow radiologists to focus more attention on:
- Abnormal scans
- Complex cases
- Uncertain findings
However, this remains an area of careful evaluation and regulation.
Does AI Sometimes Perform Better Than Humans?
In certain narrow and repetitive tasks, AI can sometimes outperform humans or help reduce specific types of errors.
AI can be very good at:
- Detecting tiny abnormalities
- Maintaining consistency
- Working without fatigue
- Rapid image analysis
- Comparing huge numbers of images
Humans can become:
- Tired
- Distracted
- Overloaded
- Inconsistent under pressure
For example, AI may detect very small lung nodules or subtle fractures that could potentially be overlooked during a busy reporting session.
However, AI also has important weaknesses.
AI may struggle with:
- Rare diseases
- Complex clinical context
- Unusual anatomy
- Poor-quality scans
- Unexpected combinations of disease
Importantly, AI and humans often make different kinds of mistakes.
The emerging evidence suggests that:
Human + AI is often better than either alone.
Will Radiologists Be Replaced?
At present, the NHS does not view AI as a replacement for radiologists.
Instead, AI is mainly being introduced as:
- A support tool
- A safety net
- A prioritisation system
- A workflow assistant
Radiologists still provide:
- Clinical judgement
- Contextual interpretation
- Decision-making
- Communication
- Management of uncertainty
In the foreseeable future, radiology is likely to become increasingly AI-assisted but still human-led.
Longitudinal Analysis: One of the Most Exciting Future Possibilities
One of the most promising future applications of AI is longitudinal analysis.
This means comparing:
- Current scans
- Previous scans
- Blood tests
- Lung function
- Medications
- Clinical notes
- Symptoms
- Outcomes over time
Humans are not particularly good at consistently recognising very subtle changes across years of imaging and clinical data.
AI could potentially become extremely powerful at:
- Tracking disease progression
- Measuring tumour growth
- Monitoring fibrosis
- Quantifying cavity enlargement
- Identifying treatment response
- Predicting future deterioration
This could be especially valuable in chronic diseases such as:
- Chronic Pulmonary Aspergillosis (CPA)
- Bronchiectasis
- Chronic Obstructive Pulmonary Disease (COPD)
- Interstitial lung disease
- Cancer
In the future, AI may help move medicine from:
“What does this scan show today?”
towards:
“What is happening over time, and what is likely to happen next?”
AI Beyond Radiology
AI Clinical Documentation
The NHS is increasingly exploring AI systems that can generate:
- Clinic letters
- Consultation summaries
- Medical notes
- Coding suggestions
These “AI scribes” may help reduce administrative burden and allow clinicians to spend more time with patients.
AI Triage Systems
Some NHS services now use AI-assisted triage systems to:
- Route patient requests
- Identify urgent problems
- Prioritise appointments
- Support NHS App workflows
Medication Safety
AI may eventually help identify:
- Drug interactions
- Prescribing errors
- Missed monitoring
- Unsafe medication combinations
Operational Efficiency
The NHS is also exploring AI for:
- Appointment scheduling
- Referral management
- Staff rostering
- Reducing missed appointments
- Managing workflow
Why AI Adoption Is Uneven Across the NHS
AI adoption currently varies considerably across the NHS.
Some trusts use multiple AI systems routinely, while others have minimal deployment.
This variation is influenced by:
- Funding differences
- IT infrastructure
- Digital maturity
- Research partnerships
- Clinical confidence
- Procurement complexity
- Availability of evidence
Large teaching hospitals and academic centres often adopt new technologies earlier than smaller hospitals.
As a result, current NHS AI deployment is best described as:
Selective, cautious and evolving.
Why the NHS Is Proceeding Carefully
The NHS is naturally cautious about AI because healthcare is fundamentally different from many other industries.
Mistakes can have serious consequences, including:
- Missed cancers
- Delayed diagnosis
- Medication harm
- Unsafe treatment decisions
For this reason, NHS AI systems generally require:
- Clinical validation
- Governance review
- Safety monitoring
- Regulatory approval
- Human oversight
- Ongoing audit
There is also awareness that:
- commercial hype can exceed evidence,
- real-world NHS workflows are complex,
- and some AI systems may not perform as well outside carefully controlled studies.
Potential Risks and Concerns
Although AI has enormous potential, there are also important concerns.
Patient Safety
AI systems can make mistakes and may occasionally be confidently wrong.
Bias
If training data is incomplete or biased, AI performance may vary between different patient groups.
Loss of Human Contact
Some patients worry that healthcare could become less personal if technology replaces human interaction.
Data Privacy
AI systems often require access to large healthcare datasets, raising understandable questions about confidentiality and data governance.
The Likely Future
The most likely future is probably not:
“AI replaces doctors.”
Instead, it is more likely to be:
“Clinicians increasingly work alongside AI systems.”
AI may gradually become another routine layer of healthcare infrastructure, much as:
- electronic patient records,
- CT scanners,
- MRI scanners,
- and digital pathology systems
became normal parts of modern medicine.
Over time, patients may benefit from:
- Earlier diagnosis
- Safer systems
- More personalised medicine
- Faster reporting
- Reduced waiting times
- Better chronic disease monitoring
However, successful implementation will depend heavily on:
- careful governance,
- good evidence,
- clinical oversight,
- public trust,
- and maintaining the human side of healthcare.
A Balanced Summary
AI in the NHS is already real, but still at an early stage of adoption.
Current use is best described as:
Promising applications in partial use, being introduced gradually and carefully while safety, effectiveness and governance continue to be evaluated.
The NHS is unlikely to move recklessly because healthcare carries high stakes. Instead, adoption will probably continue incrementally, with evidence and clinical confidence building over time.
If implemented wisely, AI has the potential to become one of the most important developments in modern healthcare — not by replacing clinicians, but by helping them deliver safer, faster and more personalised care.
Useful Resources and Further Reading
- NHS England: Artificial Intelligence and Machine Learning
- NHS AI Lab
- NHS AI Knowledge Repository
- NICE: Evidence Standards Framework for Digital Health Technologies
- UK Government: AI Opportunities Action Plan
- Royal College of Radiologists: Artificial Intelligence
- British Institute of Radiology: Artificial Intelligence Special Interest Group
- The Health Foundation: How Could AI Improve the NHS?
- The King’s Fund: Artificial Intelligence and the NHS
- Nature: Artificial Intelligence in Healthcare Collection
- The Lancet Digital Health

Living With Aspergillosis: When Others Do Not Fully Understand How You Feel
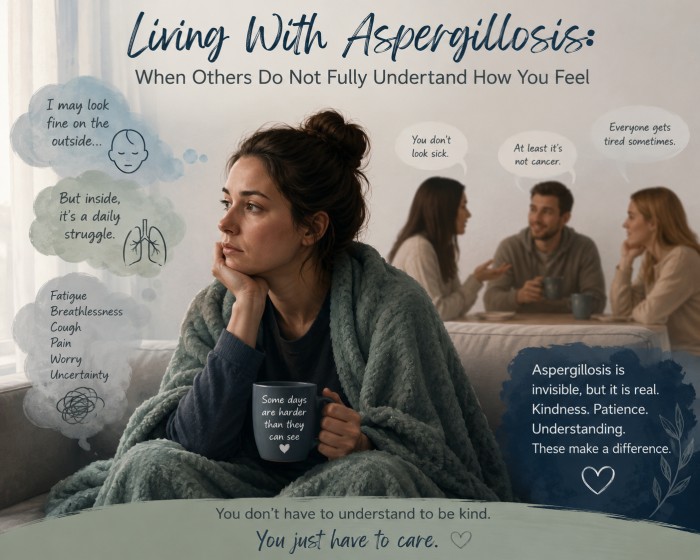
Living with aspergillosis can affect far more than the lungs. Many patients have symptoms that are difficult to explain, difficult to measure, and difficult for other people to fully understand.
Breathlessness, fatigue, coughing, chest tightness, sleep disruption, anxiety during flare-ups, medication side effects, and uncertainty about the future can all become part of daily life. These symptoms may fluctuate from day to day, and people may appear well at times even when they are struggling.
This can leave patients feeling misunderstood, dismissed, or even blamed for focusing too much on their health.
Key points
- Symptoms of aspergillosis and chronic lung disease are real, even when they are invisible to others.
- Feeling anxious, frustrated, or preoccupied with health is understandable when symptoms affect daily life.
- Validation from family, friends, and clinicians can reduce distress.
- Finding meaningful things to do beyond illness can also help patients cope.
- The aim is balance: being heard and supported, while also protecting quality of life.
Why aspergillosis can be hard for others to understand
Many people with chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), severe asthma, bronchiectasis, or other long-term lung conditions live with symptoms that are not always visible.
A patient may look well, speak normally, or have reasonable oxygen levels at rest, but still experience severe fatigue, breathlessness on exertion, anxiety during breathing difficulty, or a long recovery after simple activities.
Symptoms may also fluctuate. Someone may manage an activity one day but be unable to do the same thing the next. This inconsistency can be confusing for family, friends, employers, and sometimes even healthcare professionals.
“Stop obsessing” is usually not helpful
Patients with chronic illness are sometimes told to “stop obsessing” about their health. This may be said with good intentions, but it can feel dismissive.
Patients may hear:
“You are making too much of this.”
or:
“It is all in your head.”
In reality, many patients are not choosing to focus on illness. The illness is already demanding attention through symptoms, medication routines, appointments, uncertainty, and changes to daily life.
However, there is also a useful point hidden inside the poor wording. Constantly monitoring every symptom can become exhausting and may increase anxiety. The better message is not “stop obsessing”, but:
“Your symptoms are real, but you also deserve space in your life that is not only about illness.”
Validation matters
Validation means recognising that a person’s experience is real and understandable. It does not mean agreeing that every symptom is dangerous, or that every worry needs urgent medical action.
Useful validating phrases include:
- “I believe you.”
- “That sounds exhausting.”
- “I know this affects much more than people can see.”
- “How is today compared with your usual baseline?”
- “What would help you most today?”
Validation can reduce distress. When patients feel dismissed, they may feel driven to repeat themselves, seek reassurance, or prove how unwell they are. When they feel heard, they may find it easier to step back from constant symptom monitoring and focus on other parts of life.
The mind and body interact
Breathlessness is not just a physical sensation. It can trigger fear very quickly. This is a normal human response: breathing difficulty naturally makes the brain more alert to danger.
This does not mean symptoms are imaginary. It means chronic respiratory illness affects the whole person: physically, emotionally, socially, and psychologically.
Anxiety, uncertainty, poor sleep, and repeated flare-ups can all increase awareness of symptoms. At the same time, genuine physical symptoms can increase anxiety. The two can reinforce each other.
Recognising this interaction can help patients and clinicians work together without blame.
Finding something else to think about can help
For many patients, finding meaningful activities beyond illness is genuinely helpful. This might include hobbies, gentle exercise, time outdoors, music, crafts, reading, gardening, photography, volunteering, family activities, or peer support.
This is not the same as ignoring illness. It is a way of protecting identity and quality of life.
The aim is not to deny symptoms, but to prevent illness becoming the only focus of every day.
“Your illness is real, but it should not be allowed to take over every part of who you are.”
What families and friends can do
Family members and friends may not be able to fully understand what chronic aspergillosis feels like. They do not need perfect understanding to be supportive.
Helpful support includes:
- believing the person’s symptoms are real;
- recognising that fatigue and breathlessness may not be visible;
- avoiding dismissive comments;
- asking what would help rather than assuming;
- understanding that symptoms may fluctuate;
- encouraging enjoyable activities without pressuring the person to “push through”.
Less helpful comments include:
- “You look fine.”
- “You were able to do it yesterday.”
- “You need to stop thinking about it.”
- “Everyone gets tired.”
What clinicians may be trying to say
Sometimes clinicians may say things such as “try not to focus on it too much” because they believe further tests or treatments may not currently help. They may be trying to avoid unnecessary antibiotics, steroids, scans, or procedures.
That can be a reasonable clinical concern, but the message needs to be communicated carefully.
A better way to say it might be:
“I believe your symptoms are real and distressing. We will continue to look for changes that need treatment. At the same time, some symptoms may persist despite treatment, so we also need to support your quality of life.”
This keeps the patient heard, while also being honest about the limits of medical treatment.
Practical ways to find balance
- Use structured symptom tracking: a brief daily note may be more helpful than constant checking.
- Know your baseline: understanding what is normal for you makes changes easier to spot.
- Agree an action plan: ask your healthcare team what changes should prompt medical advice.
- Protect non-illness time: plan small, realistic activities that are not centred on health.
- Use peer support carefully: support groups can reduce isolation, but try to avoid constant comparison or fear-based searching.
- Ask for emotional support: counselling, psychological therapies, pulmonary rehabilitation, or breathing physiotherapy may help some people.
When to seek medical advice
This article is general information and does not replace medical advice. Patients should seek medical help if they experience significant or worrying change, especially:
- worsening breathlessness;
- falling oxygen saturations if they monitor them;
- new or worsening chest pain;
- coughing up blood;
- high fever, rigors, or signs of serious infection;
- new confusion, fainting, or severe weakness;
- rapid deterioration from their usual baseline;
- symptoms that feel different from their usual pattern.
If symptoms are severe or rapidly worsening, urgent medical help should be sought.
Final thought
Living with aspergillosis can be physically and emotionally demanding. Patients deserve to be believed, heard, and supported. At the same time, they also deserve help to build a life that is not entirely defined by illness.
A helpful message for patients, families, and clinicians is:
“Your illness is real. Your distress is understandable. You deserve support. And you also deserve a life with meaning, connection, and moments of relief beyond illness.”
Further support and reading
If you are living with aspergillosis and feel that others do not fully understand what you are going through, these resources may help. They offer information about long-term illness, mental wellbeing, breathlessness, invisible symptoms, and patient support.
- Aspergillosis patient support
Information about support meetings, patient resources, and ways to connect with others affected by aspergillosis. - NHS Talking Therapies
NHS support for people experiencing anxiety, depression, or emotional distress, including people living with long-term health conditions. - Asthma + Lung UK: Living with a lung condition
Practical information on living with breathlessness, fatigue, flare-ups, and the emotional effects of lung disease. - Chronic Illness Inclusion
A UK organisation focused on the experiences of people living with chronic, energy-limiting, and often invisible conditions. - The Patients Association: Long-term conditions
Advice and information for people managing long-term health conditions and navigating healthcare conversations.
Important: If your symptoms suddenly worsen, you develop severe breathlessness, chest pain, coughing up blood, confusion, fainting, or signs of serious infection, seek urgent medical advice. In the UK, call NHS 111 for urgent advice or 999 in an emergency.

European Lung Foundation (ELF): Giving Patients a Voice in Respiratory Health
What makes ELF particularly valuable is that it is genuinely patient-led. Patients and carers are not simply consulted occasionally; they actively help shape educational resources, awareness campaigns, research priorities and clinical guideline discussions.
ELF and Aspergillosis
One particularly important area of ELF’s work is its commitment to supporting people affected by aspergillosis and other fungal lung diseases.
The ELF Aspergillosis Information Hub provides accessible, reliable information about:
- ABPA (Allergic Bronchopulmonary Aspergillosis)
- CPA (Chronic Pulmonary Aspergillosis)
- Aspergilloma
- Invasive aspergillosis
- Symptoms and diagnosis
- Treatment approaches
- Living with long-term fungal disease
- Patient experiences and support
The ELF Aspergillosis Patient Advisory Group
ELF has also established a dedicated Aspergillosis Patient Advisory Group, bringing together people from across Europe with direct lived experience of aspergillosis.
The group works alongside clinicians and researchers to improve awareness, encourage earlier diagnosis, develop patient education, influence research priorities and support better long-term care.
Why Patient Participation Matters
Aspergillosis is still under-recognised in many countries, and many patients experience long delays before receiving a diagnosis. Patient involvement can help change this.
By sharing experiences, joining discussions and supporting awareness activities, patients and carers can help improve understanding of fungal lung disease, strengthen educational materials, support newly diagnosed patients and raise awareness among healthcare professionals and the public.
Not everyone needs to become a public speaker or campaigner. Participation can include joining online meetings, completing surveys, sharing experiences confidentially, reviewing patient information, supporting awareness campaigns online or helping identify what matters most to patients.
Ways to Get Involved
- Visit the ELF Aspergillosis Information Hub
- Learn about the ELF Aspergillosis Patient Advisory Group
- Explore the ELF Patient Organisation Network
- Support the Healthy Lungs for Life campaign
- Watch ELF videos on YouTube
A Shared Effort
ELF demonstrates that respiratory healthcare works best when patients, carers, clinicians and researchers work together as partners.
For people affected by aspergillosis, involvement in organisations like ELF can help transform personal experience into something that improves understanding, care and support for others across Europe and beyond.
Every patient story, question, survey response and conversation contributes to building greater awareness of aspergillosis and improving the future of care.
Smoking, COPD and Chronic Pulmonary Aspergillosis (CPA)
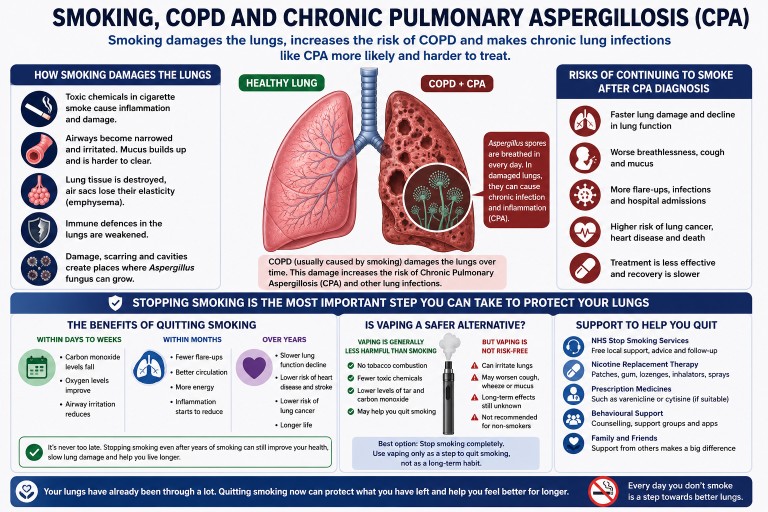
Many people diagnosed with Chronic Pulmonary Aspergillosis (CPA) also have Chronic Obstructive Pulmonary Disease (COPD). One of the strongest shared risk factors between the two conditions is cigarette smoking.
Smoking does not directly “cause” Aspergillus infection in the same way a virus or bacteria causes disease. However, it can create the lung damage and immune dysfunction that make CPA more likely to develop and harder to control.
Why smoking matters in CPA and COPD
Smoking damages the lungs over many years by:
- Destroying normal lung tissue and airways
- Causing chronic inflammation
- Reducing the lungs’ ability to clear mucus, dust and fungal spores
- Damaging the tiny hair-like structures called cilia that normally sweep organisms out of the airways
- Weakening local immune defence inside the lungs
- Increasing emphysema, cavities, scarring and bronchiectasis — all environments where Aspergillus can grow more easily
People breathe in Aspergillus spores every day. Healthy lungs usually remove them without difficulty. Damaged lungs are different. In COPD, especially severe COPD, spores can remain trapped in damaged airways and cavities, increasing the risk of long-term fungal colonisation or infection.
Is smoking causal?
The relationship is complex, but in many patients smoking is likely to be an important contributing cause.
Smoking contributes to:
- COPD development
- Structural lung damage
- Reduced immune clearance
- Increased infection risk
- Faster lung decline
All of these increase vulnerability to CPA.
Smoking is therefore not simply an associated factor. In many patients it is part of the chain of events that eventually leads to CPA developing.
Not every smoker develops CPA, and not every person with CPA has smoked. Some people develop CPA after tuberculosis, severe pneumonia, sarcoidosis, asthma, bronchiectasis, lung surgery or other lung diseases. However, smoking substantially increases risk because it accelerates lung injury and reduces the lungs’ resilience.
Why continuing to smoke after CPA diagnosis is dangerous
Once CPA is established, continuing to smoke can make management much harder.
Smoking may:
- Accelerate further lung destruction
- Worsen breathlessness and cough
- Increase mucus production
- Increase flare-ups and infections
- Reduce physical fitness and oxygen levels
- Reduce quality of life
- Increase hospital admissions
- Make COPD progression faster
- Increase risk of lung cancer alongside CPA
- Make recovery from infections slower
Many patients with CPA already have limited lung reserve. Continuing to smoke can progressively reduce the remaining healthy lung tissue.
“The damage is already done” — is stopping still worthwhile?
Yes. This is one of the commonest and most understandable feelings among long-term smokers with lung disease. However, stopping smoking can still help, even after significant lung damage has already occurred.
Within days to weeks
- Carbon monoxide levels fall
- Oxygen delivery improves
- Airways may become less irritated
- Some coughing and mucus clearance may improve
Within months
- COPD flare-ups may reduce
- Circulation improves
- Physical activity may become easier
- Inflammation begins to reduce
Over years
- Lung function decline slows
- Risk of heart disease and stroke falls
- Risk of lung cancer gradually decreases
- Survival improves compared with continued smoking
For people with CPA, preserving remaining lung function is critical. Slowing further structural damage may help stabilise disease, and antifungal treatment works best in lungs that are not being continually injured by smoke.
Is vaping a safer alternative?
Many patients ask whether vaping, or using e-cigarettes, is a safer option than smoking cigarettes.
Current evidence suggests that vaping is likely to be substantially less harmful than smoking tobacco cigarettes because vaping avoids the combustion process that produces tar, carbon monoxide and many toxic chemicals found in cigarette smoke.
For smokers who are unable to stop nicotine completely, switching entirely from smoking to vaping may reduce harm.
However, vaping is not risk-free.
Vaping aerosols can still irritate the lungs and may contain:
- Fine particles
- Flavouring chemicals
- Heating by-products
- Nicotine
- Other airway irritants
Some people with CPA, COPD, asthma or bronchiectasis report:
- Increased cough
- Throat irritation
- Chest tightness
- Wheeze
- Increased mucus symptoms
Long-term effects of vaping are still being studied.
For patients with CPA, the safest option for lung health is probably:
- Stop smoking cigarettes completely
- Use vaping only if it helps avoid returning to smoking
- Gradually reduce vaping if possible
A common problem is “dual use” — continuing to smoke while also vaping. This usually provides much less benefit than stopping cigarettes completely.
While nicotine itself is addictive, most of the major smoking-related lung damage comes from the toxic products created by burning tobacco.
For many patients, switching from smoking to vaping may still represent an important positive step if it helps them move away from cigarettes permanently.
Nicotine addiction is powerful
Many people with CPA and COPD have smoked for decades. Stopping is rarely simply a matter of willpower. Nicotine is strongly addictive, and smoking often becomes linked to stress relief, routine, anxiety management and social habits.
Patients should not feel ashamed if stopping is difficult. Repeated attempts are normal. Many successful quitters tried several times before succeeding permanently.
What can help?
Support works better than trying alone.
Options include:
- NHS stop smoking services
- Nicotine replacement therapy, such as patches, gum, sprays or lozenges
- Prescription medicines such as varenicline or cytisine, if suitable
- Behavioural support and counselling
- Gradual reduction plans
- Vape or e-cigarette transition strategies in selected patients
- Family and peer support
For many people with severe lung disease, stopping smoking is one of the most important treatments available — alongside inhalers, oxygen, physiotherapy and antifungal medication.
A realistic but important message
Patients with CPA often already live with fatigue, cough, breathlessness and anxiety about the future. Smoking may feel comforting in the short term, but it usually continues the cycle of lung injury that helped create the problem in the first place.
Stopping smoking cannot reverse established CPA, but it may:
- Slow further lung decline
- Improve day-to-day symptoms
- Improve response to treatment
- Preserve independence longer
- Reduce complications
- Improve long-term survival
Even small improvements in lung health can matter enormously when lung reserve is limited.
When to seek medical advice
Patients with CPA, COPD or other lung disease should seek medical advice if they:
- Become significantly more breathless
- Develop chest pain
- Cough up increasing amounts of blood
- Notice worsening wheeze or mucus production
- Develop fevers or signs of infection
- Feel unable to cope with smoking withdrawal symptoms alone
Stopping smoking is often difficult, but healthcare professionals can offer support and treatment options that improve the chances of success.
Breathe deeply at the Asthma + Lung UK Garden
Asthma + Lung UK’s “Breathing Space Garden” at the RHS Chelsea Flower Show is a beautiful reminder of how much our surroundings can affect our lungs, our wellbeing, and our ability to pause and breathe.
Designed by award-winning garden designer Angus Thompson, the garden is inspired by the Japanese idea of yohaku no bi — “the beauty of empty space”. It brings together calming woodland planting, flowing water, accessible design, and quiet areas for rest, reflection, yoga, and tai chi.
The planting has been chosen with lung health in mind, using low-allergen species, soft textures, resilient trees, and calming green spaces that offer a gentler environment for people with sensitive lungs.
For people living with aspergillosis, asthma, chronic obstructive pulmonary disease (COPD), bronchiectasis, and other lung conditions, this message is especially powerful. Clean air, reduced stress, accessible outdoor spaces, and thoughtful planting can all help people feel more comfortable and supported.
Importantly, the garden will continue to make a difference after Chelsea. It is due to be permanently relocated to the Breathing Space lung rehabilitation centre in Rotherham, where it will support people living with lung conditions for years to come.
RHS Chelsea Flower Show: 19–23 May 2026
Read more from Asthma + Lung UK

Physiotherapy for Aspergillosis: Breathing, Mucus Clearance and Keeping Active

Physiotherapy can be an important part of supportive care for some people living with aspergillosis. It does not treat the fungal infection itself, but it can help with breathlessness, mucus clearance, strength, fitness, posture, fatigue and confidence with activity.
This may be especially helpful for people with Chronic Pulmonary Aspergillosis (CPA), Allergic Bronchopulmonary Aspergillosis (ABPA), Severe Asthma with Fungal Sensitisation (SAFS), Aspergillus bronchitis, bronchiectasis, asthma, Chronic Obstructive Pulmonary Disease (COPD), or lung damage from previous infection.
Key points
- Physiotherapy can help some aspergillosis patients manage mucus, breathlessness and reduced activity.
- Airway clearance techniques may be useful when mucus is difficult to clear.
- The Active Cycle of Breathing Technique (ACBT) is commonly used in respiratory physiotherapy.
- Other approaches include huffing, breathing control, postural drainage, airway clearance devices, exercise training and pulmonary rehabilitation.
- Technique matters — airway clearance should ideally be taught by a respiratory physiotherapist.
- National Aspergillosis Centre (NAC) patients can ask for advice from experienced physiotherapists who understand aspergillosis.
Contents
- Why physiotherapy matters in aspergillosis
- Airway clearance and mucus management
- Active Cycle of Breathing Technique (ACBT)
- Other physiotherapy techniques
- Pulmonary rehabilitation and exercise
- Breathing retraining and breathlessness
- Where to get physiotherapy in the UK
- Useful NHS videos and guides
- When to seek medical advice
Why physiotherapy matters in aspergillosis
Many people with aspergillosis have underlying lung conditions that affect how the lungs clear mucus, expand during breathing and cope with exertion. Long-term illness can also lead to muscle weakness, reduced fitness and loss of confidence with activity.
Common problems include:
- thick or persistent mucus
- frequent coughing
- breathlessness on exertion
- fatigue
- reduced walking distance
- weakness after illness or hospital admission
- poor posture from chronic breathlessness or coughing
- anxiety around breathing
- dysfunctional breathing patterns
Physiotherapy aims to improve function and quality of life. It is often most useful when it is personalised to the patient’s lung condition, symptoms, fitness level and treatment plan.
Airway clearance and mucus management
Some people with aspergillosis produce mucus every day. This is particularly common in people who also have bronchiectasis, asthma, Aspergillus bronchitis or repeated chest infections.
Mucus that remains in the lungs can contribute to:
- blocked or narrowed airways
- more coughing
- chest tightness
- breathlessness
- fatigue
- recurrent infections
Respiratory physiotherapists can teach airway clearance techniques to help move mucus from smaller airways towards larger airways, where it can be cleared more easily by huffing or coughing.
Active Cycle of Breathing Technique (ACBT)
ACBT stands for Active Cycle of Breathing Technique. It is one of the most commonly used airway clearance methods in respiratory physiotherapy.
It usually includes three parts:
- Breathing control – gentle relaxed breathing to settle the airways.
- Deep breathing exercises – larger breaths to help air move behind mucus.
- Huffing – a controlled breath out through an open mouth to move mucus upwards.
ACBT can often be adapted depending on symptoms, oxygen levels, energy, breathlessness and the amount of mucus being produced.
Other physiotherapy techniques
Huffing
A huff is a controlled breath out through an open mouth and throat. It can move mucus without the effort of repeated hard coughing. Many patients find huffing less exhausting than forceful coughing.
Postural drainage
Postural drainage uses body position and gravity to help drain mucus from different parts of the lungs. It may not be suitable for everyone, especially people with reflux, severe breathlessness, frailty, oxygen requirements or certain heart and lung complications.
Positive Expiratory Pressure and oscillating devices
Some patients may be advised to use airway clearance devices such as Flutter®, Acapella® or Aerobika®. These devices create resistance or vibration during breathing out, helping to loosen mucus and keep the airways open.
Breathing control
Breathing control can help settle the breathing pattern, reduce panic during breathlessness and make airway clearance less tiring.
Posture and mobility work
Chronic coughing and breathlessness can affect posture. Physiotherapy may include stretching, shoulder mobility, chest wall movement, gentle strengthening and exercises to improve comfort when breathing.
Fatigue management and pacing
Fatigue is common in aspergillosis. Physiotherapists may help patients pace activities, avoid “boom and bust” patterns, and gradually rebuild function without triggering prolonged exhaustion.
Pulmonary rehabilitation and exercise
Pulmonary rehabilitation is a structured programme of exercise and education for people with long-term lung disease who experience breathlessness. NHS England describes pulmonary rehabilitation as an exercise and education programme for people with lung disease who have symptoms of breathlessness.
Programmes may include:
- supervised exercise
- walking or cycling
- strength training
- breathing advice
- education about managing long-term lung disease
- confidence-building around activity
For aspergillosis patients, pulmonary rehabilitation may be particularly useful when breathlessness, weakness or reduced activity are affecting daily life.
Breathing retraining and breathlessness
Some people feel very breathless even when oxygen levels are normal or near normal. This can happen because breathlessness is influenced by airway inflammation, muscle effort, anxiety, breathing pattern, air trapping and the brain’s perception of breathing discomfort.
Breathing retraining may include:
- slower, calmer breathing
- diaphragmatic breathing
- pursed-lip breathing
- relaxation techniques
- coordinating breathing with walking, stairs or other activity
These techniques can be especially useful for patients who feel frightened by breathlessness or who have developed an inefficient breathing pattern.
Where to get physiotherapy in the UK
Access to physiotherapy varies across the UK, but patients with long-term lung disease may be able to obtain support through several routes.
1. Through your GP or respiratory team
Your GP, respiratory consultant, specialist nurse or hospital team may be able to refer you to a respiratory physiotherapist, community respiratory team or pulmonary rehabilitation service.
2. Through pulmonary rehabilitation services
Many local NHS pulmonary rehabilitation services accept referrals for people with chronic respiratory disease, including conditions such as Chronic Obstructive Pulmonary Disease (COPD), bronchiectasis, asthma, interstitial lung disease and other long-term breathing problems. Some services accept GP referrals, hospital referrals or self-referrals, but criteria vary locally.
3. Through community respiratory teams
Some areas have community respiratory teams that provide assessment, education, pulmonary rehabilitation, breathlessness support, oxygen-related advice and airway clearance support.
4. Through hospital respiratory physiotherapy departments
Hospital respiratory physiotherapists often support patients during admissions, after exacerbations, or through specialist outpatient respiratory clinics.
5. Through the National Aspergillosis Centre
National Aspergillosis Centre (NAC) patients can ask their NAC team whether specialist physiotherapy advice would be helpful. NAC has experienced physiotherapists who understand aspergillosis and the particular problems patients may face, including mucus clearance, breathlessness, fatigue, reduced fitness and co-existing lung disease.
6. Private physiotherapy
Some patients choose to see a private physiotherapist. The NHS advises that private physiotherapists should be chartered and registered with the Health and Care Professions Council (HCPC). The Chartered Society of Physiotherapy provides a “Find a Physio” directory that can be searched by location and specialty.
Useful UK links:
- National Aspergillosis Centre Physiotherapy
- NHS: Physiotherapy
- NHS England: Pulmonary rehabilitation
- Chartered Society of Physiotherapy: Find a physiotherapist
- Association of Chartered Physiotherapists in Respiratory Care
Useful NHS videos and guides
The following NHS resources may help patients understand airway clearance techniques. They should not replace individual advice from a respiratory physiotherapist.
Royal Free London NHS Foundation Trust – Active Cycle of Breathing
A clear patient-focused demonstration of ACBT.
Watch: Active Cycle of Breathing – Royal Free London NHS Foundation Trust
NHS Greater Glasgow & Clyde – Active Cycle of Breathing
A detailed demonstration from respiratory physiotherapy services.
Watch: Respiratory Physiotherapy Service – Active Cycle of Breathing
University College London Hospitals NHS Foundation Trust – breathing and airway clearance videos
UCLH has a useful set of patient information videos covering breathing exercises and airway clearance.
Watch: UCLH patient information videos – breathing exercises
UCLH – How to clear phlegm from your chest
A short, practical NHS video explaining how ACBT can help clear phlegm.
Watch: How to clear phlegm from your chest – ACBT
Cambridge University Hospitals NHS Foundation Trust
A patient information page explaining airway clearance and ACBT.
Read: Airway clearance – Active Cycle of Breathing Technique
Hull University Teaching Hospitals NHS Trust
A detailed patient leaflet on ACBT as a secretion clearance technique.
Read: Active Cycle of Breathing Technique – secretion clearance
University Hospitals Plymouth NHS Trust
A step-by-step patient guide to breathing control, thoracic expansion exercises and huffing.
Read: Active Cycle of Breathing Technique
When to seek medical advice
Airway clearance techniques should ideally be taught by a respiratory physiotherapist. Incorrect technique may sometimes worsen coughing, fatigue, airway irritation or breathlessness.
Seek medical advice urgently if you develop:
- new or worsening coughing of blood
- sudden worsening breathlessness
- chest pain
- fever or signs of infection
- dizziness or fainting
- significant oxygen desaturation
- rapid deterioration after starting a new exercise or airway clearance routine
Summary
Physiotherapy can be an important supportive treatment for some people with aspergillosis. It may help with mucus clearance, breathlessness, posture, fatigue, strength, confidence and activity levels.
Techniques such as ACBT, huffing, breathing control, postural drainage, airway clearance devices and pulmonary rehabilitation can all help selected patients. The best approach depends on the person’s symptoms, underlying lung condition and overall health.
For NAC patients, specialist physiotherapy advice is available from professionals experienced in aspergillosis care. If mucus clearance, breathlessness or reduced activity are becoming difficult, it is worth asking the NAC team whether physiotherapy input may help.
Medical note: This article is for general information only. It does not replace advice from your doctor, specialist nurse or respiratory physiotherapist. Airway clearance and exercise plans should be tailored to the individual patient.
Last reviewed: May 2026

When Breathlessness Feels Severe — Even When Oxygen Levels Look “Normal”

Many people living with aspergillosis, severe asthma, bronchiectasis, or other chronic lung conditions describe a confusing and sometimes frightening experience:
“My oxygen saturations are normal, my peak flow is reasonable, there’s little wheeze, but I still feel like I’m drowning.”
This can be distressing for patients and frustrating for carers. Some people feel that because their oxygen levels or breathing tests appear “acceptable”, their symptoms are not fully understood.
Importantly, severe breathlessness can occur even when standard measurements such as oxygen saturations and peak flow readings appear relatively normal.
This does not mean the symptoms are imaginary or “all in the mind”. Breathlessness is complex and can have many different causes.
Why Breathlessness Is More Complicated Than Oxygen Levels
When doctors or nurses assess breathing problems, they often check:
- Oxygen saturation levels (sats)
- Peak flow readings
- Respiratory rate
- Presence of wheeze
- Chest sounds
These are all important. However, they do not always reflect how breathless a person feels.
Some people with chronic respiratory illness may have:
- Normal oxygen saturations
- Reasonable peak flow readings
- Little visible wheeze
- Minimal mucus production
…yet still experience intense sensations of:
- air hunger
- tight chest
- difficulty taking a satisfying breath
- feeling unable to “fill the lungs”
- panic associated with breathing
- extreme fatigue from breathing effort
What Can Cause This?
Breathlessness in aspergillosis and chronic lung disease is often caused by several factors happening together.
Inflammation and Airway Sensitivity
Conditions such as Allergic Bronchopulmonary Aspergillosis (ABPA), Severe Asthma with Fungal Sensitisation (SAFS), bronchiectasis, and Chronic Pulmonary Aspergillosis (CPA) can all cause inflamed and hypersensitive airways.
The lungs may feel irritated or tight even if oxygen exchange remains relatively preserved.
Small Airways Dysfunction
Some breathing problems occur in the smaller airways of the lungs and may not always show clearly on basic tests such as peak flow.
Patients can feel significant chest tightness or air trapping despite “good numbers”.
Muscle Fatigue
Breathing takes muscular effort. Chronic respiratory illness can place a long-term strain on the chest wall and breathing muscles, leading to exhaustion and increased awareness of breathing.
Mucus and Airflow Changes
Even relatively small amounts of mucus or airway narrowing can create sensations of chest heaviness or difficulty moving air.
Breathing Pattern Dysfunction (Dysfunctional Breathing)
This is increasingly recognised in people with chronic respiratory illness.
When breathing becomes difficult over months or years, people may unconsciously develop altered breathing patterns, including:
- rapid shallow breathing
- upper chest breathing
- frequent sighing
- over-breathing (hyperventilation)
- muscle tension around the chest and neck
This can worsen symptoms and create a vicious cycle where the sensation of breathlessness becomes amplified.
Symptoms may include:
- air hunger
- dizziness
- tingling
- tight chest
- panic sensations
- difficulty “switching off” breathing awareness
Importantly, this does not mean the illness is psychological or “not real”. Dysfunctional breathing can happen alongside genuine lung disease.
Why Inhalers Sometimes Seem to Help Less
Reliever inhalers such as salbutamol (Ventolin) are designed mainly to relax tightened airways.
If breathlessness is being driven partly by breathing pattern dysfunction, muscle fatigue, inflammation, hypersensitivity, or air trapping, inhalers may not always provide dramatic relief.
This can be confusing and upsetting for patients.
“But My Tests Are Normal…”
Many patients feel frustrated, frightened, or even dismissed when told that oxygen levels, peak flow readings, or chest examinations are “fine” despite severe breathlessness.
Normal oxygen saturations are reassuring in terms of immediate danger, but they do not always reflect the full experience of chronic respiratory illness.
Breathlessness is influenced by many factors including inflammation, airway sensitivity, breathing effort, muscle fatigue, anxiety associated with struggling to breathe, and altered breathing patterns.
Because of this, some people may feel profoundly breathless even when routine measurements appear relatively stable.
It can sometimes help to explain symptoms in practical, functional terms, such as:
- “I become breathless walking across the room.”
- “I recover much more slowly than usual.”
- “This feels much worse than my normal baseline.”
- “I feel exhausted by the effort of breathing.”
- “Breathing exercises seem to help settle things.”
These descriptions may help healthcare professionals understand how symptoms are affecting day-to-day life, rather than focusing only on oxygen levels or peak flow numbers.
Some patients also find it helpful to ask questions such as:
- Could breathing pattern dysfunction be contributing?
- Would respiratory physiotherapy help?
- Would pulmonary rehabilitation be appropriate?
- How should I judge when symptoms need urgent assessment?
Importantly, severe breathlessness should never simply be ignored. New, worsening, or unusual symptoms still require proper medical assessment.
At the same time, many people with chronic lung disease experience very real symptoms that are not always fully reflected by routine measurements alone.
Why Breathlessness Can Feel So Frightening
The sensation of breathlessness is created by the brain interpreting signals from the lungs, breathing muscles, chest wall, blood chemistry, and nervous system.
This means that the feeling of “not getting enough air” is not determined only by oxygen levels.
In chronic lung disease, several things can trigger the sensation of breathlessness, including:
- inflamed or sensitive airways
- extra effort needed to move air in and out
- air trapping in the lungs
- muscle fatigue
- rapid or shallow breathing
- stress hormones released during breathing distress
- heightened awareness of breathing sensations
When breathing becomes uncomfortable, the body naturally responds with anxiety and adrenaline. This is a protective survival response.
Unfortunately, this can sometimes create a cycle:
breathlessness → anxiety → faster breathing → more chest tightness → worse breathlessness
This does not mean symptoms are “psychological”. The physical sensation is real, but the body’s alarm systems can unintentionally amplify it.
What Can Help During an Episode of Breathlessness?
Different techniques help different people, and severe or rapidly worsening symptoms should always be medically assessed. However, some patients find the following approaches helpful during episodes of distressing breathlessness:
Slow the Breathing Rate
Trying to slow breathing gently can help reduce over-breathing and chest tightness.
Some people find it helpful to:
- breathe in gently through the nose
- breathe out slowly through pursed lips
- focus on making the out-breath longer than the in-breath
Use a Recovery Position
Sitting forward slightly with the arms supported on knees or a table can sometimes reduce the work of breathing.
Reduce Panic and “Air Hunger”
Trying to fight for bigger and bigger breaths can sometimes worsen symptoms.
Some patients find it more helpful to focus on:
- gentle breathing rhythm
- relaxing the shoulders and neck
- slowing breathing rather than deepening it
- focusing attention away from the chest where possible
Use Prescribed Treatments Appropriately
Follow the advice provided by your healthcare team regarding inhalers, nebulisers, airway clearance, or rescue medication.
If inhalers are not helping as expected, this should be discussed with a respiratory specialist rather than simply increasing use repeatedly.
Know Your “Usual” Pattern
Many patients find it useful to learn the difference between:
- their “usual” chronic breathlessness
- breathing pattern dysfunction or over-breathing episodes
- symptoms suggesting infection or acute deterioration
This can help patients feel more confident recognising when urgent medical assessment may be needed.
Can Breathing Retraining Help?
Some patients find breathing retraining exercises very helpful, especially when guided by:
- respiratory physiotherapists
- specialist breathing services
- pulmonary rehabilitation teams
- asthma nurse specialists
Breathing retraining may include:
- slowing breathing rate
- diaphragmatic (“belly”) breathing
- nasal breathing techniques
- recovery breathing positions
- relaxation techniques
- paced activity and pacing strategies
Some NHS respiratory teams recommend online breathing resources and guided exercises to help patients recognise and manage over-breathing patterns.
These approaches are usually intended to work alongside medical treatment — not instead of it.
Living With an “Invisible” Symptom
One of the hardest aspects of chronic breathlessness is that outward signs may not always match how severe symptoms feel internally.
Many patients report feeling dismissed when oxygen levels are normal or when tests appear “better than expected”.
The experience of breathlessness is real, even when routine measurements do not fully explain it.
This is one reason why specialist respiratory assessment can be important in complex conditions such as aspergillosis.
When to Seek Medical Help
You should seek urgent medical advice if breathlessness is:
- suddenly worsening
- associated with chest pain
- causing blue lips or fingertips
- associated with falling oxygen saturations
- accompanied by fever or signs of infection
- causing confusion or severe exhaustion
- significantly different from your usual symptoms
Even if previous episodes have been related to breathing pattern dysfunction, new or worsening symptoms should still be medically assessed.
Further Support
You may also find these resources helpful:
Last reviewed: May 2026
Produced by: National Aspergillosis Centre CARES Team / Aspergillosis Website
Mental Health Awareness Week: Supporting the Emotional Impact of Aspergillosis

Mental Health Awareness Week is a reminder that health is not only physical.
For people living with aspergillosis, and for the family members and carers who support them,
the emotional impact of a long-term lung condition can be significant.
Aspergillosis can bring uncertainty, fatigue, breathlessness, repeated appointments,
medication changes, worries about test results, and concerns about the future.
It is understandable that some people experience anxiety, low mood, frustration,
isolation, or disturbed sleep.
Carers may also feel under pressure. Supporting someone with a chronic illness can be rewarding,
but it can also be tiring and emotionally demanding. Looking after your own mental health is not selfish;
it helps you continue to support the person you care about.
Small steps can help
- Talk to someone you trust about how you are feeling.
- Stay connected with friends, family, or peer support groups.
- Pace your activities and allow time for rest.
- Try gentle movement if this is safe and manageable for you.
- Write down worries or questions before appointments.
- Ask your healthcare team for support if anxiety, low mood, or stress is affecting daily life.
You are not alone
Many people with aspergillosis find it helpful to speak with others who understand what it is like
to live with a rare fungal lung condition. Peer support can reduce isolation and help patients and carers
feel more informed and understood.
The National Aspergillosis Centre and associated patient organisations provide support, information,
and opportunities to connect with others affected by aspergillosis:
- Aspergillosis support resources for families and carers
- Weekly aspergillosis support meetings
- Aspergillosis Support Facebook group
When to seek help
If you are feeling persistently overwhelmed, very low, anxious, unable to cope,
or if your mental health is affecting your day-to-day life, please speak to your GP,
specialist nurse, or healthcare team. Mental health support is an important part of healthcare.
If you feel at immediate risk of harming yourself, or you do not feel safe,
seek urgent help by calling emergency services or going to your nearest emergency department.
More information about Mental Health Awareness Week is available from the
Mental Health Foundation
Your mental health matters. Support, understanding, and connection can make a difference.
Weekly aspergillosis research update: papers published 4–12 May 2026
This week’s PubMed search for aspergillosis identified several new papers relevant to aspergillosis diagnosis, treatment, host-pathogen biology, allergic bronchopulmonary aspergillosis (ABPA), invasive pulmonary aspergillosis (IPA), and chronic pulmonary aspergillosis (CPA).
Key themes this week
- Bronchoscopic intervention in invasive pulmonary aspergillosis: a Chinese clinical analysis reports on bronchoscopic features and interventional therapy in IPA.
- ABPA guidance and imaging: one expert consensus paper and one adult asthma imaging study add to the ABPA literature.
- Diagnostics: new papers discuss galactomannan biology, metagenomic next-generation sequencing, and radiological assessment.
- Complex invasive fungal infection: several case-based reports highlight diagnostic difficulty in mixed or unusual fungal infections.
- Antifungal pharmacology: a real-life cohort study examines isavuconazole pharmacokinetics and pharmacodynamics.
Allergic bronchopulmonary aspergillosis (ABPA)
Expert consensus on ABPA diagnosis and treatment using integrated traditional Chinese and western medicine
Allergy Committee of Chinese Association of Integrative Medicine.
Zhonghua Yi Xue Za Zhi. 2026 May 12;106(17):1678-1695.
doi: 10.3760/cma.j.cn112137-20260101-00001
PMID: 42103676
This Chinese expert consensus addresses diagnosis and treatment of allergic bronchopulmonary aspergillosis. The abstract notes that ABPA is a hypersensitivity lung disease triggered by sensitisation to Aspergillus fumigatus or other Aspergillus species, with reported incidence of 1.0–3.5% in asthma patients and 7–15% in cystic fibrosis patients.
Why it matters: Although this is a Chinese-language consensus document and includes integrated traditional Chinese and western medicine approaches, it may still be useful to track because international consensus documents can show how ABPA recognition and management are evolving globally.
Radiological manifestations of ABPA in adult asthmatic patients
Wahab F, Hussain Babar T, Nadeem SF, Amin Z, Sarwar S, Ahmad S, Wahab A, Mukhtar S.
Monaldi Archives for Chest Disease. 2026 May 7. Online ahead of print.
doi: 10.4081/monaldi.2026.3648
PMID: 42099257
This paper focuses on radiological findings in adults with asthma and allergic bronchopulmonary aspergillosis. The PubMed abstract describes ABPA as developing through type I or type III hypersensitivity reactions to filamentous fungi such as Aspergillus.
Why it matters: Imaging remains central to recognising ABPA complications such as bronchiectasis, mucus plugging and other structural airway changes. Papers that improve recognition of radiological patterns may help reduce diagnostic delay in patients labelled as having difficult asthma alone.
Invasive pulmonary aspergillosis (IPA) and complex fungal infection
Clinical analysis of comprehensive bronchoscopic interventional therapy for invasive pulmonary aspergillosis
Li J, Cai CL, Zhao LN, Wang YH, Mu XD.
Zhonghua Jie He He Hu Xi Za Zhi. 2026 May 12;49(5):555-560.
doi: 10.3760/cma.j.cn112147-20250719-00420
PMID: 42108177
This Chinese-language clinical analysis investigates bronchoscopic features of invasive pulmonary aspergillosis and summarises the clinical efficacy of comprehensive bronchoscopic interventional therapy. Underlying conditions in the reported cases included diabetes mellitus and haematological malignancy.
Why it matters: Bronchoscopy can contribute both diagnostically and therapeutically in selected patients with IPA, particularly where airway obstruction, fungal plaques, necrotic material or local complications are present. This paper may be of interest to clinicians managing complex IPA cases.
Fatal triple co-infection with Aspergillus, Mucorales and Nocardia in aplastic anaemia
Sadeghi Borkehim S, Azhdari Tehrani H, Javandoust Gharehbagh F, Kord M, Azimi M, Alavi Darazam I.
BMC Infectious Diseases. 2026 May 9.
doi: 10.1186/s12879-026-13190-0
PMID: 42106631
This case report describes a fatal triple co-infection involving Aspergillus, Mucorales and Nocardia in a patient with aplastic anaemia.
Why it matters: In severely immunocompromised patients, invasive fungal disease may not occur in isolation. Mixed infections can complicate diagnosis, delay targeted treatment and require broader microbiological investigation than would be needed for a single-pathogen infection.
Cladribine treatment in pulmonary Langerhans cell histiocytosis complicated by invasive aspergillosis
Piekarczyk P, Pajer M, Kupis W, Wojda E, Nowicka U, Radzikowska E.
Polish Archives of Internal Medicine. 2026 May 4. Online ahead of print.
doi: 10.20452/pamw.17292
PMID: 42100864
This free article reports cladribine treatment in a young patient with isolated progressive pulmonary Langerhans cell histiocytosis complicated by invasive aspergillosis. No abstract was available in the PubMed record.
Why it matters: This appears to be a highly specialised case, but it highlights the intersection between rare lung disease, immunomodulatory treatment and risk of invasive fungal infection.
Invasive pulmonary aspergillosis in an apparently immunocompetent host
Beeravolu HR, Ghewade B, Alone V, Mummaneni R, Patil PA.
Respiratory Medicine Case Reports. 2026 Apr 27;61:102425. eCollection 2026.
doi: 10.1016/j.rmcr.2026.102425
PMID: 42088316
This case report describes invasive pulmonary aspergillosis in an immunocompetent host. Although IPA classically occurs in immunocompromised patients, the authors note that it can occasionally occur without obvious immunosuppression, which may contribute to diagnostic delay.
Why it matters: Case reports of IPA in apparently immunocompetent patients should be interpreted cautiously, but they are useful reminders that clinical context, imaging, microbiology and disease trajectory all matter when assessing possible invasive fungal infection.
Diagnostics, biomarkers and fungal biology
Structure and biosynthetic mechanisms of galactomannans in filamentous fungi
Oka T, Kadooka C, Tanaka Y, Hira D.
Biochimica et Biophysica Acta - General Subjects. 2026 May 7;1870(8):130960. Online ahead of print.
doi: 10.1016/j.bbagen.2026.130960
PMID: 42105885
This review focuses on galactomannans in filamentous fungi. Galactomannan contains mannose and galactofuranose; galactofuranose is absent in humans and is clinically important because galactomannan detection is used in the diagnosis of invasive pulmonary aspergillosis.
Why it matters: Galactomannan is one of the best-known fungal biomarkers in aspergillosis diagnostics. Understanding its structure and biosynthesis helps explain both the value and limitations of galactomannan-based testing.
Metagenomic next-generation sequencing for severe influenza complicated by invasive pulmonary aspergillosis
Niu S, Guo L, Li Z, Liu Y, Zhao L.
Frontiers in Cellular and Infection Microbiology. 2026 Apr 21;16:1746504. eCollection 2026.
doi: 10.3389/fcimb.2026.1746504
PMID: 42093770
This study evaluates the diagnostic performance of metagenomic next-generation sequencing for detecting invasive pulmonary aspergillosis in patients with severe influenza.
Why it matters: Influenza-associated pulmonary aspergillosis is increasingly recognised in critically ill patients. Rapid molecular methods such as metagenomic next-generation sequencing may help identify fungal infection earlier, although interpretation requires care because detection of fungal DNA does not always prove invasive disease.
Antifungal treatment and pharmacology
Real-life pharmacokinetics and pharmacodynamics of isavuconazole
Guidi M, Couchepin J, Reinhold I, Kronig I, Neofytos D, Schreiber PW, André P, Buclin T, Lamoth F.
JAC-Antimicrobial Resistance. 2026 May 5;8(3):dlag071. eCollection 2026 Jun.
doi: 10.1093/jacamr/dlag071
This paper reports real-life pharmacokinetic and pharmacodynamic data for isavuconazole, an antifungal used in invasive aspergillosis and mucormycosis.
Why it matters: Real-world pharmacology studies are important because antifungal exposure can vary between patients. Better understanding of drug levels, exposure-response relationships and clinical outcomes may help refine antifungal monitoring and dosing strategies.
Aspergillus species, virulence and non-human disease
Pathogenic mechanisms of Aspergillus lentulus infection in Galleria mellonella
Zhang L, Ji M, Hasimu H, Abliz P.
Mycopathologia. 2026 May 9;191(3):51.
doi: 10.1007/s11046-026-01072-7
PMID: 42105125
This experimental study investigates pathogenic mechanisms of Aspergillus lentulus infection using Galleria mellonella larvae, focusing on oxidative stress and tissue damage.
Why it matters: Aspergillus lentulus is a clinically important cryptic species within the Aspergillus fumigatus complex and may show reduced susceptibility to some antifungals. Model systems such as Galleria mellonella can help explore fungal virulence mechanisms before moving into more complex models.
Antemortem diagnosis of aspergillosis in a gentoo penguin
Matsumoto N, Itoh M, Toyotome T, Watanabe K, Yamada M, Hagino K, Neo S, Yamada K.
Journal of Veterinary Medical Science. 2026 May 7. Online ahead of print.
doi: 10.1292/jvms.25-0377
PMID: 42091553
This veterinary case report describes antemortem diagnosis of aspergillosis in a gentoo penguin using computed tomography and air sac fluid aspiration.
Why it matters: Aspergillosis is an important disease in birds, particularly captive penguins. Although not directly relevant to human clinical care, veterinary aspergillosis studies can contribute to understanding host susceptibility, environmental exposure and diagnostic approaches across species.
Related respiratory and microbiome research
The gut microbiome in cystic fibrosis
Marsh R, Tricker JM, Delhaes L, Bomberger JM, van der Gast C.
Journal of Cystic Fibrosis. 2026 May 9. Online ahead of print.
doi: 10.1016/j.jcf.2026.05.003
PMID: 42108153
This review discusses recent findings and future opportunities relating to the gut microbiome in cystic fibrosis.
Why it matters: This is not primarily an aspergillosis paper, but cystic fibrosis is an important context for allergic bronchopulmonary aspergillosis and airway fungal colonisation. Microbiome research may eventually help clarify how bacterial, fungal and host factors interact in chronic airway disease.
Summary
This week’s most directly relevant papers include new work on bronchoscopic management of invasive pulmonary aspergillosis, ABPA consensus and imaging, galactomannan biology, molecular diagnosis in influenza-associated pulmonary aspergillosis, and real-world isavuconazole pharmacology. Several case reports also underline the continuing diagnostic difficulty of invasive fungal disease, particularly in complex or immunocompromised patients.

Join our UK Citizen Science Project on Damp Homes and Health

Many people living with aspergillosis, asthma and chronic lung disease tell us they are worried about damp, mould and housing conditions — but often struggle to know:
- whether their home really has a problem
- who to trust for advice
- whether mould testing is reliable
- and what effective remediation should involve.
There is currently considerable uncertainty around indoor mould assessment, air sampling and interpretation of results. Many patients report difficulty obtaining clear, independent advice or meaningful remediation.
At the same time, we still know surprisingly little about the real-life health impact of living in damp homes across the UK.
A UK Citizen Science Project
We are supporting a UK citizen science project exploring how damp homes may affect health, including respiratory health and conditions such as aspergillosis.
Citizen science projects involve members of the public helping researchers and healthcare communities better understand real-world problems by sharing experiences and observations.
You do not need to have diagnosed aspergillosis to take part.
We are interested in hearing from people:
- living in damp or mouldy homes
- living in homes without damp
- with respiratory conditions
- and without respiratory conditions.
The initial registration takes about 1 minute and simply records your interest in the project.
Why this matters
By taking part, you may help improve understanding of:
- damp homes and respiratory disease
- mould exposure
- indoor air quality
- housing conditions
- challenges with mould assessment and remediation
- and the wider health impact of dampness in UK homes.
We hope the project will help patients, clinicians, housing professionals and researchers better understand:
- how people experience damp homes in real life
- the difficulties many people face obtaining reliable advice
- the limitations of current mould assessment approaches
- and what practical interventions may genuinely improve health and quality of life.
Related information
You can also read our practical guide discussing damp homes, mould testing, remediation and tenant support:
Read our guide to damp, mould and aspergillosis
Find out more or register your interest
Damp Homes and Health Study UK
Please share this project with:
- patients and carers
- healthcare professionals
- housing professionals
- damp and mould specialists
- environmental health professionals
- researchers
- and anyone interested in improving understanding of damp homes and health.