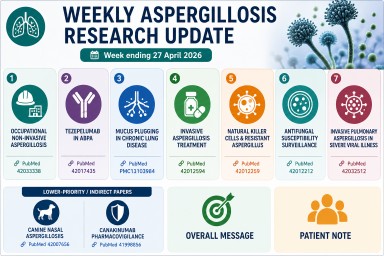
Weekly Aspergillosis Research Update: Week ending 27 April 2026
Highlights this week
- Occupational aspergillosis: workplace exposure to Aspergillus highlighted in a national study.
- ABPA and biologics: early evidence for tezepelumab in allergic bronchopulmonary aspergillosis.
- Mucus plugging: important mechanism in ABPA, bronchiectasis and chronic lung disease.
- Invasive disease: new analysis of antifungal treatment strategies.
- Resistance: ongoing global surveillance of antifungal susceptibility.
Occupational non-invasive aspergillosis
A French national multicentre study reviewed occupational cases of non-invasive aspergillosis over more than 20 years.
Why it matters: workplace exposure (dust, compost, damp buildings, waste handling) may contribute to disease in some patients and should be considered in clinical history-taking.
Reference: Michel A et al.
PMID: 42033338
Tezepelumab in allergic bronchopulmonary aspergillosis
A small 4-patient case series explored the use of tezepelumab in allergic bronchopulmonary aspergillosis (ABPA) with severe asthma.
Why it matters: adds to growing interest in biologics for ABPA, particularly where steroid burden is high. Evidence remains early and limited.
Reference: Sanz-Sanjosé B et al.
PMID: 42017435
Mucus plugging in chronic lung disease
A narrative review examined mucus plugging in chronic obstructive lung diseases and bronchiectasis, including ABPA.
Why it matters: mucus plugs can block airways, worsen breathlessness, and contribute to infection risk and scan abnormalities.
Reference: Schou C et al.
PMCID: PMC13103984
Invasive aspergillosis treatment
A systematic review and network meta-analysis compared antifungal treatment regimens for invasive aspergillosis.
Why it matters: invasive aspergillosis remains a high-mortality infection; early diagnosis and optimal antifungal therapy are critical. Triazoles and other antifungals remain central to management. :contentReference[oaicite:0]{index=0}
Reference: Gu Q et al.
PMID: 42012594
Natural killer cells and resistant Aspergillus
A laboratory study demonstrated antifungal activity of human natural killer cells against azole-resistant Aspergillus fumigatus.
Why it matters: improves understanding of immune defence mechanisms and may inform future therapies.
Reference: Namie H et al.
PMID: 42012259
Antifungal susceptibility surveillance
A multicentre Taiwan study examined susceptibility patterns of clinical Aspergillus isolates (2021–2023).
Why it matters: resistance patterns vary geographically, influencing antifungal treatment choices.
Reference: Hsieh M et al.
PMID: 42012212
Invasive aspergillosis in severe viral illness
A study explored invasive pulmonary aspergillosis complicating severe fever with thrombocytopenia syndrome.
Why it matters: reinforces the link between severe illness, immune disruption, and risk of invasive aspergillosis.
Reference: Du Q et al.
PMID: 42032512
Lower-priority or indirect papers
Veterinary study (canine nasal aspergillosis)
Primarily a veterinary oncology study with limited relevance to human disease.
Reference:
PMID: 42007656
Canakinumab pharmacovigilance
Focuses on drug safety rather than aspergillosis.
Reference:
PMID: 41998856
Overall message
This week’s research highlights the wide scope of aspergillosis—from environmental and occupational exposure to allergic disease, invasive infection, antifungal resistance, and immune responses. The most relevant developments for patients remain ABPA biologics, mucus plugging, and antifungal resistance trends.
Patient note
This summary is for general information only and does not replace medical advice. Always discuss treatment decisions with your specialist team.
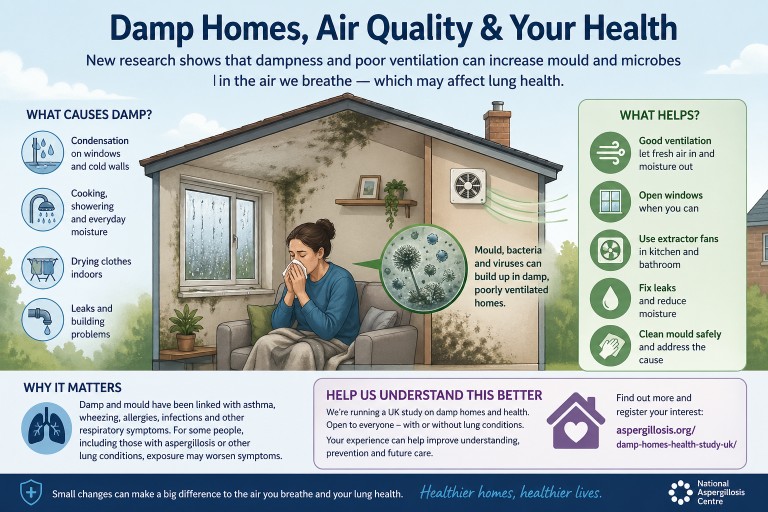
Damp Homes, Indoor Air and Health: What a Recent Evidence Review Tells Us
Summary: A recent rapid review by researchers from the Health and Safety Executive examined evidence on microbiological hazards in buildings, including moulds, bacteria and viruses. The review highlights that dampness, poor ventilation and building design can all affect indoor air quality and respiratory health.
Key points
- People spend much of their time indoors, so indoor air quality can strongly affect health.
- Damp indoor conditions increase the risk of mould growth and musty odours.
- Common indoor moulds include Aspergillus, Penicillium and Cladosporium.
- Dampness and visible or hidden mould are linked with asthma, rhinitis, wheeze and other respiratory symptoms.
- Ventilation is one of the most important ways to reduce moisture and dilute airborne contaminants.
- Improving energy efficiency is important, but very airtight homes still need adequate ventilation.
Contents
- Why indoor air matters
- What the review found
- Damp, mould and lung health
- Aspergillus and aspergillosis
- Ventilation and building design
- What can help reduce risk?
- Help us understand damp homes and health
- When to seek medical advice
Why indoor air matters
Most of us spend a large amount of time indoors — at home, at work, or in public buildings. The air inside buildings can contain particles from many sources, including dust, mould spores, bacteria, viruses, cooking, cleaning products, pets and outdoor air entering the home.
The recent review, Exposure Risks from Microbiological Hazards in Buildings and Their Control — A Rapid Review of the Evidence, looked at evidence for harmful microorganisms in indoor air and on surfaces, and how building design, ventilation and moisture affect exposure.
What the review found
The review found strong evidence that microorganisms can be present in indoor air and on surfaces. These include fungi, bacteria and viruses. The evidence was strongest for the role of dampness and poor ventilation in increasing the risk of indoor mould growth and respiratory health effects.
The review’s main conclusions included:
- Airborne allergenic fungi are well documented in indoor air.
- Damp conditions increase mould growth and mouldy odours indoors.
- Dampness and mould are associated with respiratory ill health, including asthma, rhinitis and wheezing.
- Penicillium, Aspergillus and Cladosporium are commonly detected in damp buildings.
- Infectious viruses and bacteria can also be detected in indoor air and on surfaces.
- Ventilation is a key control measure for reducing moisture and diluting airborne contaminants.
Damp, mould and lung health
Dampness is one of the most important drivers of indoor mould growth. Moisture can come from leaks, condensation, flooding, poor insulation, inadequate heating, drying clothes indoors, cooking, showering, or poor ventilation.
When dampness persists, mould can colonise indoor materials such as plasterboard, wallpaper, wood, carpets, soft furnishings and settled dust. Mould may be visible, but it can also grow in hidden areas such as behind furniture, inside wall cavities, behind wallpaper, under flooring, or around poorly ventilated cold surfaces.
Exposure to damp and mould has been linked with:
- Wheezing
- Asthma symptoms or asthma worsening
- Rhinitis and nasal symptoms
- Cough
- Respiratory infections
- Worsening symptoms in people with existing lung disease
Importantly, the review notes that the relationship between indoor microorganisms and health is complex. Risk depends on the type of organism, the level of exposure, the building conditions and the susceptibility of the person exposed.
Aspergillus and aspergillosis
Aspergillus is a common mould found in the environment. Most people inhale Aspergillus spores every day without becoming ill. However, some people are more vulnerable, including those with asthma, bronchiectasis, chronic lung disease, weakened immune systems, or previous lung damage.
In susceptible people, exposure to Aspergillus may contribute to conditions such as allergic bronchopulmonary aspergillosis (ABPA), severe asthma with fungal sensitisation (SAFS), aspergillus bronchitis, or chronic pulmonary aspergillosis (CPA). The home environment is not the only source of exposure, but damp indoor spaces may increase the amount of fungal material a person breathes in.
This does not mean that every damp home causes aspergillosis, or that every person exposed to mould will become ill. It does mean that reducing dampness, improving ventilation and addressing visible or hidden mould are sensible steps for respiratory health.
Ventilation and building design
One of the strongest messages from the review is that ventilation is central to controlling indoor microbiological risk. Ventilation helps by:
- Removing moisture from indoor air
- Reducing condensation
- Diluting airborne mould spores and other particles
- Reducing the build-up of infectious aerosols
- Improving overall indoor air quality
The review also highlights an important modern problem. Homes are increasingly designed or retrofitted to be more airtight and energy efficient. This can improve warmth and reduce energy use, but if ventilation is inadequate, moisture and airborne contaminants may accumulate indoors.
In other words, insulation and energy efficiency are important, but they need to be balanced with effective ventilation and moisture control.
What can help reduce risk?
The review does not suggest that one single action solves all indoor air problems. Instead, it supports a combined approach.
1. Reduce moisture
- Repair leaks promptly.
- Check roofs, gutters, pipes and window seals.
- Use extractor fans in kitchens and bathrooms where available.
- Avoid drying clothes indoors where possible, or ventilate well if you do.
- Reduce condensation on windows and cold walls.
2. Improve ventilation
- Use trickle vents if fitted.
- Open windows when safe and practical.
- Use mechanical ventilation systems correctly.
- Keep air bricks and vents clear.
- Make sure extractor fans are working effectively.
3. Deal with mould safely
- Small areas of surface mould may be cleaned carefully using appropriate household methods.
- Large, persistent or recurring mould usually needs the underlying damp problem fixed.
- People with significant lung disease, immune suppression or severe symptoms should avoid heavy mould disturbance and seek advice.
4. Reduce dust reservoirs
- Regular cleaning can reduce settled dust and spores.
- HEPA-filter vacuum cleaners may be helpful for some households.
- Hard flooring may be easier to keep dust-free than carpets in high-risk situations.
5. Consider air filtration where appropriate
Portable high-efficiency particulate air (HEPA) filters may help reduce airborne particles in some settings. They are not a substitute for fixing damp or improving ventilation, but they may be a useful additional measure for some people.
Help us understand damp homes and health
The evidence linking damp homes, mould and respiratory health is strong, but there are still important unanswered questions. We need to better understand how different homes, building types, ventilation patterns and damp conditions affect people’s health in real life.
The National Aspergillosis Centre is running a UK citizen science study looking at damp homes and health.
We are inviting people to register their interest in taking part.
The study is open to people with and without lung conditions, and to people living in homes with or without damp or mould. This comparison is important because it helps researchers understand which factors are most strongly linked with health outcomes.
Register your interest in the damp homes and health study
Taking part may involve completing a questionnaire and, at a later stage, providing a dust sample from your home. The information gathered will help improve understanding of indoor environments and respiratory health.
When to seek medical advice
Please seek medical advice if you have:
- New or worsening breathlessness
- Chest pain
- Coughing up blood
- Persistent fever
- Repeated chest infections
- Rapidly worsening asthma symptoms
- Unexplained weight loss or severe fatigue
If you already have aspergillosis, asthma, bronchiectasis, chronic obstructive pulmonary disease (COPD), immune suppression, or another lung condition, it is worth discussing any significant damp or mould exposure with your healthcare team.
Common questions
Can mould affect health even if I cannot see it?
Yes. Hidden mould or dampness may still affect indoor air quality. A musty smell, persistent condensation or symptoms that worsen in a particular room may suggest a problem.
Does all mould cause aspergillosis?
No. Mould exposure is common, and most people do not develop aspergillosis. Aspergillosis usually occurs when exposure combines with individual susceptibility, such as asthma, bronchiectasis, immune suppression or existing lung damage.
Is ventilation always good?
Ventilation is usually important for reducing moisture and improving indoor air quality. However, the best approach depends on the building, outdoor conditions and the person’s health. Ventilation should not replace fixing leaks or removing sources of damp.
Can air purifiers solve damp and mould problems?
No. Air purifiers may reduce airborne particles, but they do not remove the source of moisture or mould growth. Damp problems need to be addressed at source.
Summary
This recent evidence review reinforces a practical message: indoor air quality matters. Dampness, poor ventilation and mould growth are not simply cosmetic housing problems — they can affect respiratory health, especially in people with asthma, aspergillosis or other lung conditions.
The most effective approach is to reduce moisture, improve ventilation, remove mould sources where possible and understand how buildings influence exposure. Research such as the UK damp homes and health study will help build better evidence for patients, clinicians, housing providers and policymakers.
References and further reading
- Beswick A, Crook B, Gosling B, et al. Exposure Risks from Microbiological Hazards in Buildings and Their Control — A Rapid Review of the Evidence. Atmosphere. 2025;16:1243. doi:10.3390/atmos16111243.
- Damp homes and health study — register your interest
- Aspergillosis.org — patient and carer information
Article type: Patient and public information
Last reviewed: April 2026
Based on: Recent evidence review of microbiological hazards in buildings and their control.
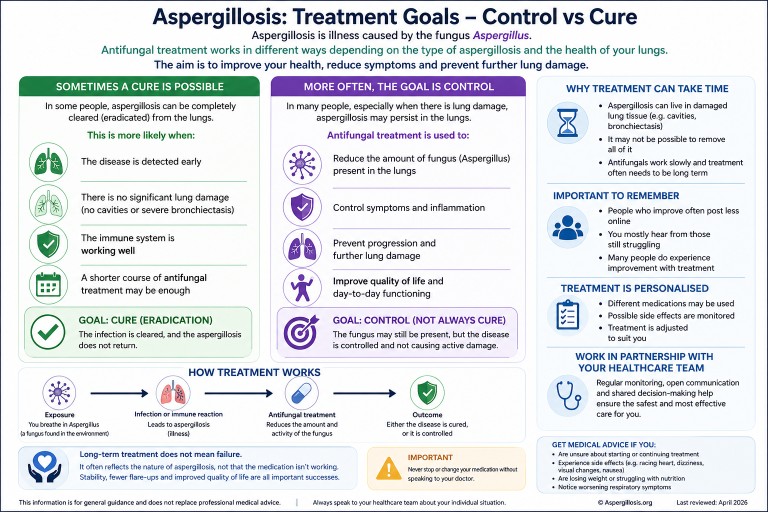
Can Aspergillosis Be Cured? Understanding Treatment, Control, and Long-Term Therapy
Last reviewed: April 2026
Key points
- Aspergillosis is caused by fungi from the Aspergillus group.
- Most people breathe in Aspergillus spores regularly without becoming ill.
- In some people, damaged airways, lung cavities, mucus plugs, or immune responses allow the fungus or fungal material to persist.
- Antifungal treatment may aim to cure, but in many cases the goal is long-term control.
- Steroids can reduce harmful inflammation in allergic disease, but they can also reduce the body’s ability to clear fungus.
Table of contents
- Overview
- Why breathing in spores does not usually cause disease
- Why aspergillosis can be hard to clear
- Infection and ABPA: different reasons for persistence
- Do steroids influence this?
- Control vs cure
- Common antifungal treatments
- Why you may not hear many success stories
- When to seek medical advice
- Common questions
Overview
It is very common for people diagnosed with aspergillosis to feel worried when they read that others have been taking antifungal medication for months or even years.
This can lead to an understandable question:
“Does treatment actually work, or will I have this forever?”
The answer is more nuanced than a simple yes or no. Different forms of aspergillosis behave differently, and treatment goals vary depending on the condition.
Two of the most common conditions are:
- Allergic Bronchopulmonary Aspergillosis (ABPA) – an allergic immune reaction to Aspergillus in the airways
- Chronic Pulmonary Aspergillosis (CPA) – a long-term fungal infection, usually in areas of damaged lung tissue
Understanding this difference is key to understanding why treatment may continue for a long time.
If you would like a more detailed explanation of how these conditions are diagnosed and managed, see our guides to chronic pulmonary aspergillosis (CPA) and allergic bronchopulmonary aspergillosis (ABPA).
Why breathing in spores does not usually cause disease
Aspergillus spores are present in the environment, including air, soil, compost, dust, and decaying vegetation. Most people breathe in small numbers of these spores regularly without becoming ill.
In healthy lungs, spores are usually cleared by the immune system and by the normal cleaning mechanisms of the airways.
This means:
- Exposure to Aspergillus is common
- Most exposure does not lead to disease
- Aspergillosis usually develops only when there are additional risk factors, such as lung damage, mucus trapping, or altered immune responses
So it is not accurate to think of most patients as being “constantly reinfected”. A better way to think about it is that some lungs provide conditions where Aspergillus, or fungal material, can persist and continue to cause problems.
Why aspergillosis can be hard to clear
Aspergillosis can be difficult to clear for several reasons. These include the structure of the lungs, the biology of the fungus, limitations of drug penetration, and the way the immune system responds.
1. Damaged lung tissue can provide protected spaces
In CPA, Aspergillus often grows in areas of abnormal lung, such as cavities, scarred tissue, or areas affected by bronchiectasis.
These areas can act as protected spaces where the fungus is harder for the immune system and antifungal medicines to reach.
2. Thick mucus can trap fungus and fungal material
In airway diseases such as asthma, bronchiectasis, and ABPA, thick mucus can trap spores, hyphae, and fungal fragments.
This trapped material can continue to stimulate inflammation even when the fungus is not invading lung tissue.
3. Antifungal medicines may suppress rather than sterilise
Antifungal medications can reduce fungal activity and help prevent progression, but they may not always remove every trace of fungus from damaged lung spaces or mucus-filled airways.
For this reason, success is often measured by:
- Improved symptoms
- Stabilised weight and energy
- Fewer flare-ups
- Stable or improved scans
- Prevention of further lung damage
Infection and ABPA: different reasons for persistence
Chronic pulmonary aspergillosis: persistence of infection
In chronic pulmonary aspergillosis, the problem is fungal growth in damaged lung tissue.
- Lung cavities provide spaces where fungus can grow
- Drug penetration may be limited
- The immune system may not fully clear infection
Allergic bronchopulmonary aspergillosis: persistence of reaction
In ABPA, the main issue is an exaggerated immune response.
- Mucus traps fungal material
- Small amounts can trigger strong reactions
- Inflammation leads to more mucus
Do steroids influence this?
Yes. Steroids can be helpful but must be used carefully.
In ABPA, they reduce inflammation but may also reduce fungal clearance.
In chronic infection, steroids can increase the risk of persistence or progression.
Monitoring and drug interactions are important during treatment.
Control vs cure: what is the goal?
For many people, the realistic goal is:
- Stability rather than eradication
- Reduced symptoms
- Prevention of progression
Common antifungal treatments
- Itraconazole
- Voriconazole
- Posaconazole
These treatments are selected based on individual factors and require monitoring.
Why don’t I hear many success stories?
People who improve often post less, while those still struggling are more visible in forums.
When to seek medical advice
- Uncertainty about treatment
- Side effects
- Weight loss
- Worsening symptoms
Common questions
Can aspergillosis be cured?
Sometimes, but often it is managed long-term.
Are people constantly reinfected?
No. Most people clear spores regularly without issue.
Why is ABPA difficult to treat?
Because of ongoing immune reactions and mucus trapping.
Further reading
- Chronic Pulmonary Aspergillosis (CPA)
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Antifungal medicines
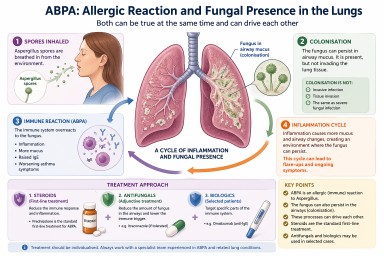
ABPA: Allergic Reaction or Fungal Presence in the Lungs?
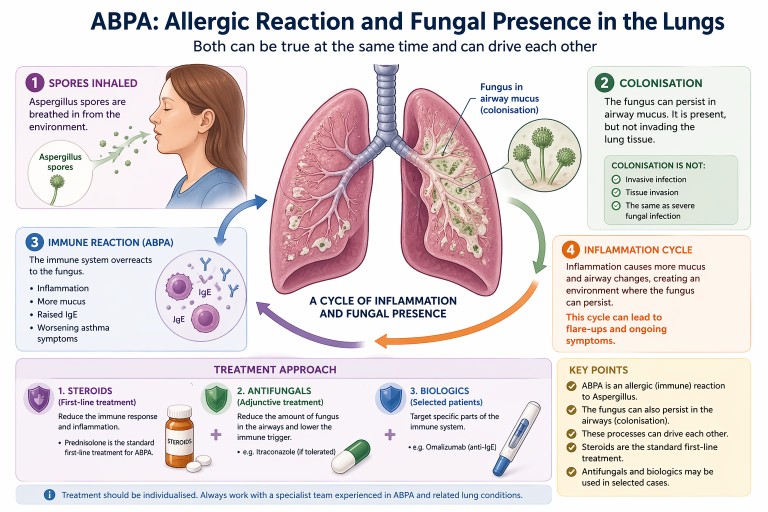
Allergic Bronchopulmonary Aspergillosis (ABPA) can be confusing. It is often described as an allergic condition, yet patients may also be told there is “fungus in the lungs”.
In reality, both can be true at the same time.
Key points
- ABPA is primarily an allergic (immune) reaction to Aspergillus
- The fungus can also persist in the airways (colonisation)
- Colonisation is not the same as invasive infection
- Steroids are the standard first-line treatment
- Antifungals and biologics may be used in selected cases
What is ABPA?
ABPA is a condition where the immune system overreacts to a common environmental fungus, most often Aspergillus fumigatus.
For a full introduction, see our guide to
what is ABPA.
This leads to:
- airway inflammation
- increased mucus production
- worsening asthma symptoms
- raised Immunoglobulin E (IgE) levels
If you are unfamiliar with IgE, see
our explanation of IgE.
Importantly, ABPA is not an invasive fungal infection. The lungs are reacting to fungal material rather than being invaded by it.
Can the fungus live in the lungs?
Yes—this is an important nuance.
In people with conditions such as:
- asthma
- bronchiectasis
the structure of the airways can allow Aspergillus to persist in mucus within the airways. This is known as colonisation.
Colonisation means:
- the fungus is present in airway mucus
- it may grow at low levels locally
- it does not invade lung tissue
This is very different from serious invasive fungal infections seen in severely immunocompromised patients.
How ABPA and colonisation interact
ABPA and colonisation are best understood as part of a spectrum of Aspergillus-related lung disease.
They can interact in a cycle:
- Aspergillus spores are inhaled
- The fungus persists in airway mucus
- The immune system reacts strongly (ABPA)
- Inflammation leads to more mucus production
- This creates an environment where the fungus can persist
This cycle can contribute to:
- recurrent flare-ups
- ongoing inflammation
- persistently raised IgE levels
Standard treatment: steroids
Oral corticosteroids are the traditional first-line treatment for ABPA.
Steroids such as prednisolone are used because they:
- reduce airway inflammation
- suppress the allergic immune response
- improve symptoms such as breathlessness and cough
- help control flare-ups
Learn more in our guide to
steroids and aspergillosis.
Where do antifungals fit in?
Antifungal medications such as itraconazole are often used as an additional (adjunctive) treatment rather than the primary therapy.
The aim is to:
- reduce the amount of fungus present in the airways
- lower the trigger for the immune response
- sometimes allow a reduction in steroid dose
For more detail, see our
antifungal treatments guide.
Biologic treatments
Biologic therapies such as omalizumab (anti-IgE) are increasingly used in some patients, particularly when:
- symptoms are difficult to control
- steroid side effects are significant
- there is severe asthma alongside ABPA
Read more about
biologics in asthma and ABPA.
Why results and symptoms may not match
Some people with ABPA may feel relatively well but still have:
- raised IgE levels
- evidence of fungal presence in the airways
This is because blood tests reflect underlying immune activity, which does not always match how a person feels day to day.
Why treatment is individualised
Although steroids are the standard treatment, management is often tailored to the individual. This is because people may also have:
- asthma
- bronchiectasis
- difficulty tolerating antifungal medications
- side effects from long-term steroid use
Specialist teams balance these factors when planning treatment.
When to seek medical advice
People with ABPA should seek medical review if they experience:
- worsening breathlessness
- increased cough or sputum
- new or persistent chest symptoms
- possible medication side effects
Treatment decisions should always be made with a clinician experienced in managing Aspergillus-related lung disease.
Summary
- ABPA is primarily an allergic condition
- The fungus can also persist in the airways (colonisation)
- These processes can drive each other
- Steroids are the standard first-line treatment
- Antifungals and biologics may be used in selected cases
Last reviewed: April 2026
Prepared by: National Aspergillosis Centre (patient information resource)
Fermented Foods & Lung Health: Safety, Infection Risk and Aspergillosis
Last reviewed: April 2026
Many people with lung conditions ask whether foods like kefir, yoghurt or cider vinegar could trigger infections. This article explains what we know — and what we don’t — based on current evidence and patient experience.
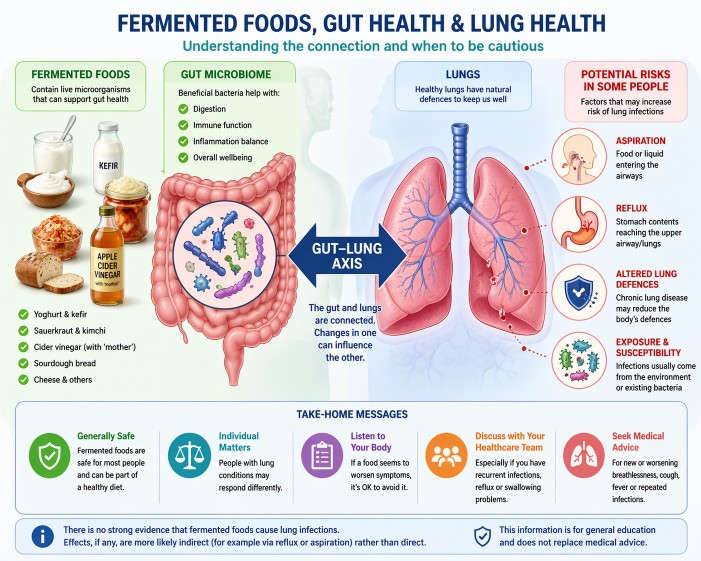
Can fermented foods cause lung infections?
No. There is no strong evidence that fermented foods cause lung infections such as pneumonia. Any effects on the lungs are more likely indirect, for example through reflux or aspiration rather than direct infection.
Quick answer: fermented foods are generally safe, but individual responses vary.
Key Points
- Fermented foods contain live microorganisms, usually beneficial bacteria and yeasts
- For most people, these foods are safe and part of a healthy diet
- There is no strong evidence linking fermented foods to lung infections
- Some people with lung disease may be affected by reflux or aspiration
- If symptoms worsen after certain foods, it is reasonable to avoid them
Table of Contents
- What are fermented foods?
- Are fermented foods safe?
- Can they cause infections?
- Why concerns arise in lung disease
- Who may need caution?
- Practical considerations
- Common questions
- When to seek medical advice
What are fermented foods?
Fermented foods are made using microorganisms (such as bacteria or yeast) to transform food. Examples include yoghurt, kefir, sauerkraut, kimchi, cheese and cider vinegar (including those containing the “mother”).
These microorganisms are generally considered non-harmful or beneficial.
Are fermented foods safe?
For most people, including many with chronic lung conditions, fermented foods are considered safe.
They may support gut health, although evidence varies depending on the product and individual.
You can read more in our
diet and aspergillosis guide
.
Can they cause infections?
There is no clear evidence that eating fermented foods causes lung infections such as pneumonia.
Lung infections usually arise from:
- Microorganisms already present in the airways
- Inhaled organisms from the environment
This is explored further in our article:
Why antibiotics do not always work
.
Why do concerns arise in lung conditions?
People with aspergillosis, bronchiectasis or chronic lung disease may be more sensitive to changes affecting the lungs.
1. Aspiration
If small amounts of food or liquid enter the airway, this can contribute to infection.
2. Reflux
Reflux can reach the upper airway and may play a role in lung irritation.
3. Lung microbiome
The lungs contain their own microbial environment, which can shift during illness.
4. Coincidence vs causation
An infection occurring after a dietary change does not necessarily mean the food caused it.
Evidence in this area is still developing, and most studies focus on gut health rather than direct lung effects.
Who might need to be more cautious?
- Frequent lung infections
- Significant bronchiectasis
- Swallowing difficulties
- Severe reflux
- Weakened immune systems
At specialist centres such as the National Aspergillosis Centre, these factors are considered alongside overall lung health.
Practical considerations
- Avoid foods that appear to worsen symptoms
- Introduce new foods gradually
- Be cautious with unpasteurised products
- Keep a simple symptom diary
Common questions
Are probiotics the same as fermented foods?
No. Probiotics are specific strains studied for health benefits, while fermented foods vary widely.
Should people with aspergillosis avoid fermented foods?
There is no general recommendation to avoid them. Most people tolerate them well.
Can fermented foods affect the lungs directly?
Not usually. Effects, if present, are more likely indirect.
When to seek medical advice
- New or worsening breathlessness
- Persistent cough or sputum changes
- Fever or infection symptoms
- Repeated infections
Summary
Fermented foods are generally safe, but individual responses vary. There is no strong evidence linking them to lung infections, but factors such as reflux or aspiration may be relevant in some people.
Balancing general evidence with personal experience is key.
References
- Marco ML et al. Health benefits of fermented foods.
PMID: 28433791
View on PubMed - Hill C et al. Probiotics consensus.
PMID: 24912386
View on PubMed - Budden KF et al. Gut–lung axis.
PMID: 27694885
View on PubMed - Dickson RP et al. Lung microbiome.
PMID: 26965149
View on PubMed - Marik PE. Aspiration pneumonia.
PMID: 11430328
View on PubMed - NICE Pneumonia guidance
View NICE guidance
Author & Review
This article has been prepared by the National Aspergillosis Centre CARES team for patients and non-specialists.
It is intended for general education and should not replace individual medical advice.
Help us understand how damp homes affect health

We are supporting a UK research project looking at how damp homes may affect health, including respiratory health and conditions such as aspergillosis.
This study is being led by the National Aspergillosis Centre at Manchester University NHS Foundation Trust, and is being shared through aspergillosis.org to support research into damp homes and health.
We are currently inviting people across the UK to register their interest in taking part.
Registering your interest should take less than one minute and does not commit you to taking part.
Why this matters
Damp and mould are often linked to health problems, but there is still limited real-world evidence from people’s homes across the UK.
This project aims to help improve understanding of how home environments may affect health by gathering information from people living in a wide range of housing conditions.
Who can register interest?
We would like to hear from people living in the UK, including:
- people with lung or respiratory conditions
- people without any known lung or breathing condition
- people who have experienced damp or mould at home
- people who have not experienced damp or mould at home
- members of the general public who would like to contribute to the research
We are keen to hear from people with different health backgrounds and a wide range of home environments.
What is the study about?
This research is exploring how damp homes may affect health. The aim is to improve understanding of the relationship between home environments and health symptoms in real-world settings.
This project is for research purposes only and does not provide medical advice or diagnosis.
What might taking part involve later?
If the study opens, some people who register interest may later be invited to:
- complete a short questionnaire about their home and health symptoms
- receive a simple home sampling kit by post
- collect and return a small household sample, for example dust from the home, for research purposes
The home sampling part is intended to be simple and practical. Full instructions would be provided.
Registering your interest now does not commit you to taking part later.
Important information
- Registering interest is voluntary.
- You do not have to take part in the full study later.
- Your details will only be used to contact you about this project.
- Your data will be handled in line with UK data protection regulations.
- You can decide later whether or not to take part.
Frequently asked questions
Am I signing up to take part in the study now?
No. At this stage, you are only registering your interest in hearing more about the study.
Do I need to have a lung condition to register interest?
No. We would like to hear from people with and without lung conditions.
Do I need to have damp or mould in my home?
No. We are interested in hearing from people with a wide range of home environments and experiences.
Will I definitely receive a kit?
Not necessarily. Registering interest helps the research team understand the level of interest and contact people if the study opens.
Will I get personal results about my home or health?
At this stage, no individual results are being promised. More information would be provided if the study proceeds.
What happens after I register interest?
You do not need to do anything further straight away. If the study opens, you may be contacted with more information so you can decide whether you would like to take part.
Register your interest
Ready to help? Complete the form below.
This secure form should take less than one minute to complete.
If the form does not load, you can open it here:
Open the form in a new window
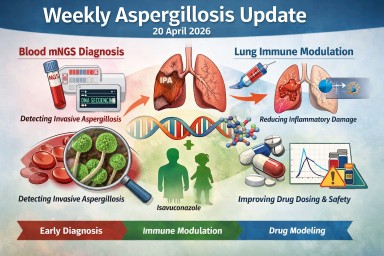
Weekly aspergillosis update – 20 April 2026
This week’s papers point in three useful directions for aspergillosis research: better diagnosis, more precise immune modulation, and improved antifungal pharmacology modelling. The most directly relevant study for day-to-day human aspergillosis care is a new paper on blood metagenomic next-generation sequencing (mNGS) for invasive pulmonary aspergillosis.
1. Blood metagenomic next-generation sequencing for invasive pulmonary aspergillosis
Chen Y, Tang X, Lu S, Guo L, Wang L, Min L, Niu T, Zhou Y.
The diagnostic and prognostic utility of blood metagenomic next-generation sequencing for invasive pulmonary aspergillosis.
Microbiology Spectrum, 17 April 2026.
View on PubMed (PMID: 41995327)
This study addresses one of the hardest clinical problems: distinguishing true invasive pulmonary aspergillosis from colonisation when Aspergillus is detected. A reliable blood-based test could be especially useful where bronchoscopy is not possible or results are unclear.
At present, this should be seen as promising rather than practice-changing, but it is exactly the type of work needed to improve early and accurate diagnosis.
2. Gene delivery of immunomodulatory cytokines to the lung
Makuyana N et al.
Gene delivery of immunomodulatory cytokines to the lung preserves respiratory function during inflammatory challenge.
Science Immunology, 17 April 2026.
View on PubMed (PMID: 41996474)
This preclinical study explores whether delivering immunomodulatory cytokines directly to the lungs can reduce damaging inflammation. The work is linked to influenza-associated pulmonary aspergillosis, where immune-driven lung injury can be severe.
The key idea is that fungal lung disease is not only about infection, but also about how the immune system responds. This represents a shift toward combining antifungal treatment with targeted immune modulation—although this approach is still at an early, experimental stage.
3. Isavuconazole pharmacokinetic modelling (preprint)
Choules MP et al.
Development of an Isavuconazole Physiologically-based Pharmacokinetic Model for Adult and Pediatric Populations.
Research Square, 17 April 2026 (preprint).
This study uses physiologically based pharmacokinetic (PBPK) modelling to predict how isavuconazole behaves in adults and children, including potential drug–drug interactions.
The findings suggest broadly similar interaction risks across age groups, but highlight greater uncertainty and caution in children under 3 years, particularly with drugs such as digoxin and warfarin.
As a preprint, this is best viewed as supportive pharmacology data, not a change to clinical practice.
4. Histopathology in infectious disease diagnosis
Boubacar E et al.
Histopathological Diagnosis of Infectious Diseases: Experience From a Tertiary Care Center in a Sub-Saharan African Country.
International Journal of Surgical Pathology, 16 April 2026.
View on PubMed (PMID: 41989331)
This broader study included a small number of aspergillosis cases and highlights the continued importance of histopathology, particularly when infections mimic cancer or other conditions.
5. Avian aspergillosis biomarker research
Vieu S et al.
Falcon plasma proteomics to improve avian aspergillosis diagnosis.
Journal of Proteomics, 14 April 2026.
View on PubMed (PMID: 41990917)
This veterinary study explores new plasma biomarkers for diagnosing aspergillosis in birds. While not directly applicable to human care, it reflects a broader research trend toward earlier, less invasive diagnosis.
What matters most this week?
The most important development is the blood mNGS study, which targets a real diagnostic gap. The immunology paper is conceptually important for future treatments, while the isavuconazole modelling work supports ongoing improvements in antifungal use.
Bottom line
This week reinforces three key directions in aspergillosis research:
- Earlier and more accurate diagnosis
- Better understanding of immune-driven lung damage
- More precise antifungal drug use and interaction modelling
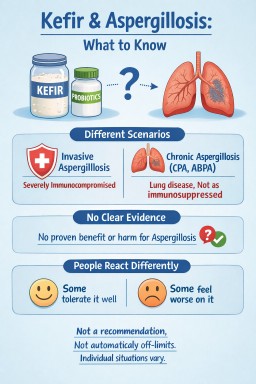
Can People with Aspergillosis Drink Kefir or Take Probiotics?
Many people with aspergillosis ask whether they can safely drink kefir or take probiotics. Kefir is a fermented drink containing live bacteria and yeasts, which raises understandable questions for people with lung conditions. This article explains what is known, what is uncertain, and why advice can differ between chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), and more severe forms of aspergillosis.
Short answer: this is not something with a simple yes-or-no answer. For people with chronic forms of aspergillosis, kefir and probiotic products are not routinely discussed in the same way as they are for people who are severely immunocompromised. However, there is also not enough evidence to say they are helpful for aspergillosis, and people’s experiences vary.
Key Points
- Advice about live foods is often stricter for people with invasive aspergillosis or severe immune suppression
- For chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), and related long-term conditions, the picture is usually less clear-cut
- There is no strong evidence that kefir specifically helps or harms chronic aspergillosis
- Some people feel fine with fermented foods; others feel they do not suit them
- The aim here is to inform, not recommend
What Is Kefir?
Kefir is a fermented drink, usually made from milk, containing a mixture of bacteria and yeasts. It is often described as a probiotic food because it contains live microorganisms.
People may use kefir or probiotic products because of interest in:
- gut health
- recovery after antibiotics
- the microbiome
If you are interested in the wider role of food and nutrition in lung health, see our article on diet and aspergillosis: what helps, what doesn’t, and what matters most.
Why Does This Question Come Up in Aspergillosis?
Different forms of aspergillosis have different risk profiles
It is important not to group all forms of aspergillosis together.
- Invasive aspergillosis usually affects people with very weakened immune systems. In that setting, clinicians are often more cautious about foods or products containing live microorganisms.
- Chronic pulmonary aspergillosis (CPA) usually affects people with underlying lung damage or structural lung disease. Many patients are not severely immunocompromised in the same way.
- Allergic bronchopulmonary aspergillosis (ABPA) and related allergic conditions raise slightly different questions again, because symptom flares may relate more to sensitivity and inflammation than to infection risk.
That distinction matters, because advice that is appropriate for one group may not automatically apply to another.
Chronic vs Invasive Aspergillosis: Why It Matters
For people with chronic pulmonary aspergillosis, the question is usually less about needing to avoid kefir as a rule, and more about recognising that there is no established role for it in treatment. In other words, kefir is not a treatment for CPA, but nor is it routinely listed as something that every patient with CPA must avoid.
For people with ABPA, the picture is slightly different again. Some patients are very aware of foods that seem to trigger symptoms, but that still does not create a universal rule that fermented foods should always be avoided.
What Does the Evidence Say?
At present, there is no strong evidence showing that kefir has a specific benefit for aspergillosis, and there is also no clear evidence that it is harmful in most people with chronic aspergillosis.
Most discussion around kefir and probiotics comes from broader research on:
- the gut microbiome
- antibiotic-associated bowel symptoms
- general digestive health
That is not the same as proving benefit for lung symptoms, fungal disease, or long-term respiratory outcomes.
For related discussion about how antibiotics affect symptoms, infections, and the microbiome, you may also find this helpful: why antibiotics do not always work.
Probiotics and the Gut–Lung Connection
Research into the gut–lung axis suggests that the gut microbiome may influence immune responses elsewhere in the body, including the lungs. This is an active area of research, but it is still early, and it does not yet mean that fermented foods or probiotic supplements should be seen as treatments for aspergillosis.
Some people are interested in probiotics because of repeated antibiotic courses, bowel side effects, or a general wish to support gut health. Those are understandable reasons, but the evidence for a direct lung benefit in chronic aspergillosis remains limited.
Why Do People React Differently?
The main reasons for caution are usually not “aspergillosis” on its own, but the wider clinical picture.
For example, extra caution may be more relevant in people who are:
- severely immunocompromised
- taking high-dose steroids or other immunosuppressive treatment
- acutely unwell
- known to react poorly to fermented foods or probiotic products
In some people, symptoms after kefir may be more about tolerance than infection risk. Patients sometimes describe:
- bloating
- nausea
- abdominal discomfort
- a sense that fermented foods do not suit them
Others report no obvious problems at all. This is one reason it is safer to frame kefir as an individual tolerance issue rather than something routinely recommended or routinely banned.
Kefir in Chronic Pulmonary Aspergillosis (CPA)
For people with CPA, the question is usually less about fungal exposure from kefir and more about whether it suits the individual patient. Many people with CPA have damaged lungs rather than profound immune suppression, so the same dietary warnings used in invasive fungal disease do not automatically apply.
- kefir is not a standard treatment for CPA
- it is not routinely listed as something that must be avoided in all patients with CPA
- individual circumstances, treatments, and tolerance still matter
If you are newly diagnosed or want a broader overview, see our CPA information page.
What About ABPA and Other Allergic Conditions?
In ABPA and related conditions, some people are understandably more alert to foods that seem to trigger symptoms. Fermented products may not suit everyone, but there is not a clear universal rule that they should be avoided.
As with many food-related questions in chronic lung disease, experiences are mixed and difficult to generalise. If you would like a fuller explanation of ABPA itself, visit our ABPA information page.
Homemade vs Shop-Bought Products
Some people also ask whether homemade kefir is different from commercial products. In general terms, homemade fermented products may be less standardised than commercially prepared ones, but that does not automatically mean they will cause a problem. It simply adds another layer of variability.
This is another reason why broad, one-size-fits-all advice is difficult.
How Should This Be Framed for Patients?
A cautious and balanced way to put it is:
Kefir is a fermented drink containing live bacteria and yeasts. Questions about it often come up in aspergillosis because advice is sometimes stricter for people who are severely immunocompromised. For people with chronic conditions such as CPA or ABPA, there is no clear evidence that kefir is either beneficial or harmful for aspergillosis itself. People’s experiences vary, so it is best thought of as an individual tolerance issue rather than something routinely recommended or routinely banned.
When Extra Caution May Be Needed
Extra caution may be more relevant if someone is:
- severely immunocompromised
- on significant immunosuppressive treatment
- recovering from serious illness
- already experiencing ongoing gut symptoms or unexplained food intolerance
In those situations, questions about probiotics, supplements, or fermented foods are often best discussed with a clinician who understands the wider medical picture.
When to Seek Medical Advice
It is sensible to discuss diet or probiotic questions with a clinician or specialist team if:
- you are severely immunocompromised
- you are on significant immunosuppressive treatment
- you develop persistent gut symptoms after using a probiotic product
- you are unsure how advice applies to your particular diagnosis or treatment
Healthcare professionals looking for more formal clinical material can visit our Information for Professionals page.
Common Questions
Can kefir treat aspergillosis?
No. There is no evidence that kefir treats aspergillosis.
Is kefir dangerous with chronic pulmonary aspergillosis?
There is no clear evidence that kefir is harmful in most people with chronic pulmonary aspergillosis, but there is also no evidence that it is beneficial for the condition itself. Tolerance varies between individuals.
Should people with ABPA avoid fermented foods?
Not necessarily. Some people feel certain foods do not suit them, but there is no universal rule that all fermented foods should be avoided in ABPA.
Summary
- Kefir is a fermented probiotic drink containing live bacteria and yeasts
- Advice that applies to invasive aspergillosis does not always apply in the same way to chronic pulmonary aspergillosis or allergic bronchopulmonary aspergillosis
- There is no strong evidence that kefir treats or worsens chronic aspergillosis
- The safest educational position is a neutral one: not a recommendation, not a blanket prohibition
- Individual circumstances, treatments, and tolerance matter
Last reviewed: April 2026
Reviewed by: National Aspergillosis Centre patient information team perspective
Please note: This article is for general education and should not be used as individual medical advice.
Could diarrhoea on itraconazole be C. diff?
Last reviewed: 20 April 2026
Understanding the difference for people with aspergillosis
Key points
- Clostridioides difficile (C. diff) is a bowel infection most often linked to antibiotic use, not antifungal treatment.
- Itraconazole can cause diarrhoea and stomach upset as a recognised side effect, but that is not the same as having C. diff.
- People with aspergillosis may still be at higher risk of C. diff because many have had recent antibiotics, repeated antibiotic courses, hospital care, or other illnesses.
- Persistent watery diarrhoea, tummy pain, fever, bleeding, dehydration, or diarrhoea lasting more than a few days should not be ignored.
- Probiotics may help some people reduce antibiotic-associated diarrhoea, but they are not suitable for everyone and are not a treatment for C. diff.
Contents
- Why this question comes up so often
- What is C. diff?
- Is itraconazole a usual cause of C. diff?
- Why people with aspergillosis may still worry about C. diff
- Side effect or infection?
- What do NHS sources advise?
- Do probiotics help?
- Common questions
- Why this matters in aspergillosis
- When to seek medical advice
- Take-home message
- Suggested internal links
- References
Why this question comes up so often
If you live with aspergillosis, it can be hard to work out why new symptoms have appeared. Many patients have had antibiotics at some point for chest infections, have been in hospital, or take several medicines at once. So when diarrhoea develops while on itraconazole, it is understandable to wonder whether the antifungal is to blame, whether it is a simple side effect, or whether something more important is going on.
That confusion is common, because several different problems can cause similar gut symptoms.
What is C. diff?
Clostridioides difficile (C. diff) is a bacterium that can infect the bowel and cause diarrhoea, abdominal pain and sometimes much more severe illness. It often affects people whose usual gut bacteria have been disrupted, especially after antibiotic use.
Some people carry C. diff without symptoms, but when the balance of the gut changes, the bacteria can multiply and produce toxins that irritate and inflame the bowel. That is why C. diff is more than “just diarrhoea”. It is a specific infection with recognised causes and recognised risks.
Is itraconazole a usual cause of C. diff?
In general, no. Itraconazole is an antifungal, not an antibiotic, and it is not recognised as a typical trigger for C. diff. Most guidance links C. diff mainly to antibiotics, especially in people who are older, frailer, recently hospitalised, or otherwise vulnerable.
That said, itraconazole can cause gastrointestinal side effects, including diarrhoea. So someone may genuinely develop bowel symptoms while taking itraconazole without having C. diff.
The important point is this: diarrhoea on itraconazole does not automatically mean C. diff, but it should not automatically be dismissed as “just the antifungal” either.
Why people with aspergillosis may still worry about C. diff
Even if itraconazole is not the usual cause, people with aspergillosis may still face a real risk of C. diff because many have had one or more recognised risk factors:
- recent or repeated antibiotic courses
- recent hospital stay or healthcare exposure
- older age
- other illnesses or frailty
- sometimes medicines such as proton pump inhibitors have also been associated with increased risk
So in practice, a patient may be taking itraconazole when diarrhoea starts, but the bigger driver may actually be a recent antibiotic course or hospital admission rather than the antifungal itself.
Side effect or infection?
Here is the distinction many patients find helpful.
Diarrhoea more suggestive of a medicine side effect
A simple side effect from itraconazole may cause:
- looser stools
- nausea
- abdominal discomfort
- symptoms that are unpleasant but relatively mild and not rapidly worsening
Diarrhoea more concerning for C. diff or another bowel infection
Symptoms that deserve proper attention include:
- frequent watery diarrhoea
- tummy pain or cramping
- fever
- blood in the stool or bleeding from the bottom
- dehydration, such as very dry mouth, dizziness, or passing very little urine
- diarrhoea lasting more than 7 days
- feeling generally very unwell
| More suggestive of side effect | More concerning for infection such as C. diff |
|---|---|
| Mild diarrhoea or looser stools | Frequent watery diarrhoea |
| Mild nausea or stomach discomfort | Tummy pain, cramping, fever |
| Symptoms remain mild | Symptoms worsening or lasting several days |
| No bleeding or dehydration | Bleeding, dehydration, or feeling very unwell |
In other words, the pattern and severity matter. Mild stomach upset can happen with many medicines. Persistent watery diarrhoea, pain, fever or bleeding should not simply be written off as “one of those things”.
What do NHS sources advise?
NHS advice is to seek urgent help if diarrhoea happens while taking, or after recently taking, antibiotics, if there is blood in the diarrhoea, or if it lasts more than 7 days. Severe pain, fever, or signs of dehydration are also warning signs.
This matters because true C. diff is a recognised medical problem with specific treatment pathways.
Do probiotics help?
Probiotics are products that contain live microorganisms (usually bacteria or yeast) intended to support the balance of the gut microbiome. They are often sold as capsules, powders, or drinks.
They are widely available, but their role in preventing or managing diarrhoea is still being studied, and product quality varies considerably.
What does the evidence suggest?
- Some studies suggest probiotics may help reduce antibiotic-associated diarrhoea.
- There is some evidence they may reduce the risk of C. diff in certain situations, particularly when started early during antibiotic treatment.
- However, results are inconsistent, and benefits are usually modest.
Are probiotics a treatment for C. diff?
No. Probiotics are not a standard treatment for confirmed C. diff infection. Medical treatment is required for confirmed cases.
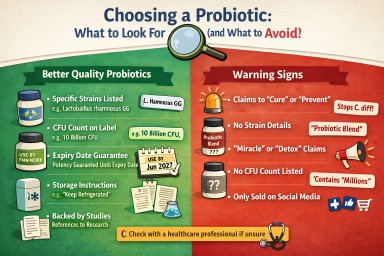
How to recognise a higher-quality probiotic
If people are considering probiotics, it can be helpful to understand what distinguishes more credible products from less reliable ones.
- Clearly labelled strains – for example Lactobacillus rhamnosus GG rather than just “Lactobacillus”. Evidence is strain-specific.
- CFU count (colony forming units) – this indicates the number of live organisms. Typical products range from millions to billions of CFU.
- Expiry-date guarantee – reputable products state the number of live organisms at the end of shelf life, not just “at manufacture”.
- Storage instructions – some require refrigeration; unclear instructions may suggest lower quality control.
- Evidence transparency – more reliable manufacturers refer to published studies rather than making vague claims.
Common red flags to be cautious about
- Claims to “cure” or “prevent” serious conditions such as C. diff
- Very long lists of ingredients without clear strain identification
- No CFU count or unclear labelling
- Heavy marketing language such as “miracle”, “detox”, or “boosts immunity dramatically”
- Products sold only through social media or unverified online sources
Are probiotics safe for everyone?
Probiotics are often well tolerated, but they are not suitable for everyone.
- People who are immunocompromised or seriously unwell may be at risk of rare infections linked to probiotic organisms.
- This includes some patients with complex lung disease, those on immunosuppressive treatment, or those with central lines.
- Because of this, probiotics should be discussed with a healthcare professional before use in these groups.
What is the practical take?
- Probiotics may help some people reduce diarrhoea associated with antibiotics.
- They are not routinely recommended for everyone.
- They are not a treatment for C. diff.
- Product quality varies, so understanding labels is important.
- For people with long-term conditions such as aspergillosis, it is sensible to check before using them.
As research into the gut microbiome develops, understanding of probiotics may improve. For now, they are best seen as a possible supportive option in some situations, rather than a standard part of care.
Common questions
Can antifungals cause C. diff?
Not usually. The main recognised trigger is antibiotic exposure, not antifungal therapy. But antifungals such as itraconazole can cause diarrhoea as a side effect, which can create understandable confusion.
Could I get C. diff if I have not had antibiotics recently?
Yes, it is possible, but antibiotics are the classic and most important risk factor. Recent hospital contact and other vulnerabilities can matter too.
If my diarrhoea started after itraconazole, does that prove itraconazole caused it?
No. Timing can be a clue, but it does not prove the cause. A side effect is possible, but so are other explanations, including infection, recent antibiotics, other medicines, or unrelated bowel problems.
Could acid-suppressing tablets increase risk?
Possibly. Proton pump inhibitors have been associated with C. diff risk in some studies, but that does not prove they directly cause it.
Why this matters in aspergillosis
For aspergillosis patients, this topic matters for two reasons.
First, gut symptoms are common, especially when treatment is complex. That makes it easy to mislabel symptoms. Second, many patients have also needed antibiotics for chest infections or have had hospital admissions, which means true C. diff risk may be more relevant than it first appears.
The safest message is not “itraconazole causes C. diff” and not “it is definitely nothing serious”, but rather: know the difference, notice the red flags, and get persistent symptoms checked.
When to seek medical advice
Seek medical advice promptly if diarrhoea is:
- frequent and watery
- continuing rather than settling
- happening after recent antibiotics
- accompanied by tummy pain, fever, bleeding, or dehydration
- making you feel significantly unwell
Take-home message
Long-term itraconazole use is not a typical direct cause of C. diff. However, itraconazole can cause diarrhoea, and people with aspergillosis may still be at risk of C. diff because of recent antibiotics, hospital exposure, and other health factors.
The key is not to jump to conclusions either way: mild diarrhoea can be a medicine side effect, but persistent watery diarrhoea, pain, fever, bleeding or dehydration should be taken seriously.
Suggested internal links
- Antifungal treatment hub
- Why antibiotics do not always work
- Chronic Pulmonary Aspergillosis
- Allergic Bronchopulmonary Aspergillosis (ABPA)
- Information for professionals
References
- NHS. Clostridioides difficile (C. diff) infection.
- NICE. Clostridioides difficile infection: antimicrobial prescribing (NG199).
- BNF. Itraconazole.
- UK Health Security Agency. Clostridioides difficile guidance, data and analysis.
- UK Health Security Agency. Increase in Clostridioides difficile infections: current epidemiology data and investigations.
Author: National Aspergillosis Centre CARES Team
Epigenetics and Aspergillosis: Why Your Body Responds Differently – and What Future Treatments May Look Like
Last reviewed: April 2026
Audience: Patients, carers, GPs, specialist nurses
This article explains how the immune system, environment, and emerging research all connect. If helpful, you can explore each topic in more detail using the links throughout this page.
Key Points
- Epigenetics controls how your genes behave without changing your DNA sequence.
- It helps explain why people with similar lung disease develop different forms of aspergillosis.
- Both the human immune system and the fungus itself use epigenetic mechanisms.
- These processes influence inflammation, immune response, and treatment effectiveness.
- Future treatments may combine antifungals, biologics, and epigenetic approaches.
- There are currently no epigenetic therapies for aspergillosis in routine NHS care.
Table of Contents
- What is epigenetics?
- How epigenetics works (simple explanation)
- Why this matters in aspergillosis
- Different diseases, different immune patterns
- Damp, mould, and environmental exposure
- Why treatment works differently
- Biologics vs epigenetics
- What research is trying to do
- Epigenetics in Aspergillus itself
- What this means for the future
- Common questions
- When to seek medical advice
- References
What is epigenetics?
If you are new to aspergillosis, you may find it helpful to first read our overview of what aspergillosis is.
Epigenetics refers to changes in how your genes are used by your body, without changing the underlying DNA sequence.
You can think of your DNA as a library of instructions. Epigenetics controls:
- Which instructions are read
- When they are used
- How strongly they are activated
This allows your body to adapt to its environment—but it can also contribute to disease.
How epigenetics works (simple explanation)
There are three main mechanisms:
- DNA methylation – switches genes off
- Histone modification – controls how tightly DNA is packaged (affecting access to genes)
- MicroRNAs – fine-tune gene activity
These processes are now recognised as key regulators of immune and fungal biology
(Nie et al., 2018).
Why this matters in aspergillosis
Patients often ask:
“Why did I develop this when others didn’t?”
Epigenetics helps explain why similar exposures to Aspergillus can result in:
- Allergic disease
- Chronic infection
- No disease
This reflects differences in immune system “programming”.
Importantly, this programming is influenced by:
- Past infections
- Lung damage (e.g. COPD, TB)
- Environmental exposure
- Medications
Is the body “testing” responses before they become permanent?
It can sometimes feel as though the body is “trying out” different ways of responding to infection or environmental exposure.
This idea comes close to how epigenetics works—but it is important to understand it carefully.
A useful way to think about it
Epigenetics allows the body to rapidly adjust how genes behave in response to the environment. This can happen over days, months, or years, and may influence how the immune system reacts to fungi such as Aspergillus.
In this sense, epigenetics can be thought of as allowing the body to explore different “settings” of immune response—for example:
- A stronger allergic response (as seen in ABPA)
- A weaker or less effective response (as seen in CPA)
- A balanced response with minimal symptoms
What epigenetics does not do
It is important to be clear that the body is not deliberately “testing” changes in a planned way, and epigenetic changes are not directly converted into permanent genetic mutations.
Instead:
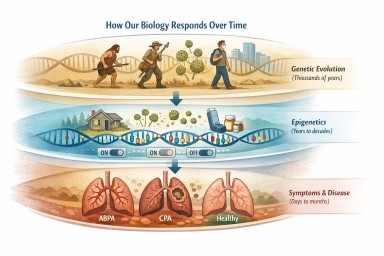
- Epigenetic changes are fast and flexible
- Genetic changes (mutations) occur slowly and randomly
- Natural selection acts over long timescales to favour traits that improve survival
How the two processes connect
Although separate, epigenetics and evolution can interact over time.
If a particular way of responding to infection is consistently helpful, individuals whose genes naturally produce a similar response may be more likely to thrive over generations.
This means:
- Epigenetics shapes how the body responds in the short term
- Evolution shapes which responses persist in the long term
Why this matters in aspergillosis
This helps explain why:
- Different people respond very differently to the same fungal exposure
- Symptoms can change over time
- Modern environments (such as damp housing or long-term steroid use) may produce responses that our immune systems were not originally adapted for
Can epigenetic changes be inherited?
Most epigenetic changes happen within a single lifetime and are not passed on to children. However, there is growing evidence that some epigenetic changes may persist or be transmitted across generations under certain conditions.
This is sometimes called transgenerational epigenetic inheritance.
For example, research suggests that:
- Environmental exposures (such as diet, stress, or infection) may leave lasting epigenetic marks
- Some of these marks may influence how genes behave in the next generation
- This effect is usually partial and not always predictable
In humans, this area is still being studied, and the extent to which epigenetic changes are inherited remains uncertain.
What this means in practice
It is important not to overinterpret this idea:
- Epigenetic inheritance is not a replacement for genetic inheritance
- Most traits and diseases are still determined by DNA and environment
- There is currently no evidence that conditions like aspergillosis are directly passed on through epigenetic changes
However, this research does suggest that environment and health may have longer-term effects than previously thought, potentially influencing future generations in subtle ways.
In simple terms:
Epigenetics allows the body to adapt quickly. Evolution determines what lasts.
Different diseases, different immune patterns
See also:
Allergic pattern (ABPA)
- Strong Th2 immune response
- High IgE and eosinophils
- Exaggerated reaction to fungal spores
Epigenetic changes may increase expression of cytokines such as IL-4, IL-5, and IL-13, driving allergic inflammation.
Chronic infection pattern (CPA)
- Reduced ability to clear fungus
- Persistent infection in damaged lung areas
- Chronic inflammation and tissue damage
Epigenetic changes may “lock in” ineffective immune responses.
Damp, mould, and environmental exposure
Long-term exposure to damp and mould is highly relevant.
It may:
- Alter airway cell behaviour
- Increase sensitivity to fungal spores
- Promote ongoing inflammation
These effects may persist through epigenetic changes, even after exposure is reduced.
See:
Why treatment works differently
Epigenetics may explain why patients respond differently to treatment.
- Some respond well to steroids
- Others develop resistance or side effects
- Biologic response varies between individuals
A key mechanism involves reduced activity of enzymes such as histone deacetylase 2 (HDAC2), which is important for steroid response.
See also: Why antibiotics do not always work
Biologics vs epigenetics
Biologics
- Target specific immune signals (e.g. IgE, IL-5)
- Fast and precise
- Widely used in severe asthma and ABPA
Epigenetics
- Acts at a deeper level
- Influences multiple pathways
- May create longer-lasting effects
Epigenetics is unlikely to replace biologics—it is more likely to enhance and personalise them.
What research is trying to do
1. Restoring steroid sensitivity
Research is exploring how to restore HDAC2 activity and improve steroid effectiveness.
2. Trained immunity (immune memory)
Immune cells can be “trained” by past exposures. This may lead to:
- Better defence
- Or harmful chronic inflammation
Scientists are studying how to reset this balance.
3. MicroRNA biomarkers
MicroRNAs may help predict:
- Disease severity
- Risk of relapse
- Treatment response
4. Metabolic and immune reprogramming
Immune cell metabolism is closely linked to epigenetic regulation. Modifying this may improve immune function.
Epigenetics in Aspergillus itself
The fungus is not passive—Aspergillus fumigatus also uses epigenetic control.
This influences:
- Virulence (how aggressive it is)
- Biofilm formation
- Resistance to antifungal drugs
Recent research shows that epigenetic regulators directly affect fungal interaction with the host
(Liu et al., 2026).
Other studies show control of toxin production and colonisation
(Hao et al., 2023).
What this means for the future
The most realistic model is layered care:
- Antifungals
- Steroids
- Biologics
- Environmental control
- Future epigenetic approaches
Epigenetics may:
- Improve treatment response
- Reduce relapse
- Enable personalised care
These approaches are still in development.
Common Questions
Can I change my epigenetics?
Not directly. However, reducing damp exposure and maintaining general health may support better immune regulation.
Are these treatments available?
No. They are still in research.
Why do my symptoms fluctuate?
Immune regulation changes over time. Epigenetics may contribute alongside infection and exposure.
Is this the next generation of treatment?
It is better seen as an additional layer that may improve existing treatments.
When to seek medical advice
- Worsening breathlessness
- Increased cough
- Chest pain
- Weight loss
- Sudden symptom changes
This article is for education and does not replace clinical advice.
References
- Liu H et al. (2026)
- Nie X et al. (2018)
- Hao L et al. (2023)
- BTS Clinical Statement
- ISHAM Guidelines