
Lung Bleeding (Haemoptysis) in Aspergillosis: What It Means and What to Expect
 Last reviewed: March 2026
Last reviewed: March 2026Audience: Patients, carers, and non-specialist healthcare professionals
Applies to: Chronic Pulmonary Aspergillosis (CPA), bronchiectasis, and related lung conditions
Key Points
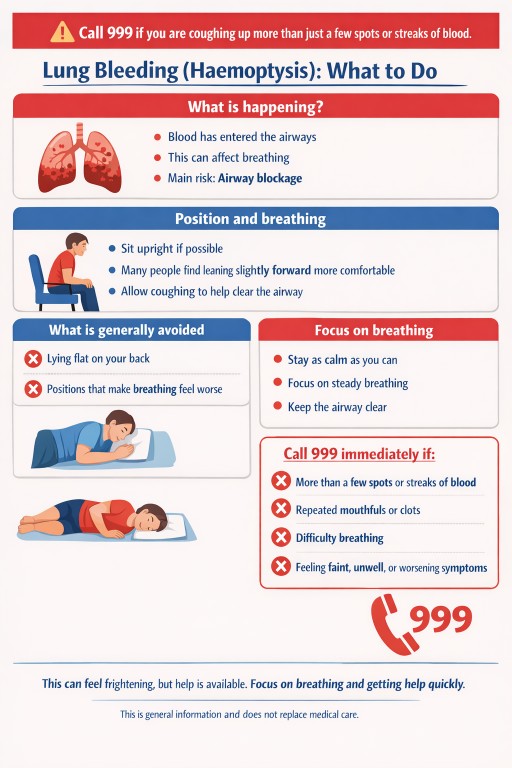
- Coughing up more than a few spots or streaks of blood is a medical emergency
- If bleeding is heavier or affects breathing, call 999 immediately
- The main immediate risk is airway blockage, not just blood loss
- Emergency care focuses on keeping airways clear and protecting breathing
- Some general positioning approaches are commonly used in healthcare settings
- This page provides general information only and is not a substitute for medical care
Table of Contents
- What is haemoptysis?
- Why can it happen in aspergillosis?
- Why does it feel so frightening?
- When is it an emergency?
- What happens during emergency care?
- While waiting for help (general guidance)
- Why positioning matters
- Understanding airway safety
- What is generally avoided
- What happens after hospital care?
- Medications such as tranexamic acid
- Common questions
- When to seek medical help
What is haemoptysis?
Haemoptysis means coughing up blood from the lungs or airways. This can range from small streaks in sputum to larger bleeds.
In people with Chronic Pulmonary Aspergillosis (CPA) and related lung conditions, haemoptysis can occur due to changes in lung structure and blood vessels.
Why can it happen in aspergillosis?
- Areas of lung damage (such as cavities) may develop
- Blood vessels in these areas can become fragile
- Inflammation may increase susceptibility to bleeding
Not all patients will experience haemoptysis, but awareness is important.
Why does it feel so frightening?
Many patients describe a strong sensation of being unable to breathe during a lung bleed.
This can occur because blood enters the airways, which may interfere with airflow. Even small amounts in the wrong place can feel overwhelming.
This reaction is common and understandable.
When is it an emergency?
NHS guidance advises calling 999 if you are coughing up more than just a few spots or streaks of blood.
Call 999 immediately if:
- You are coughing up more than just a few spots or streaks of blood
- You are coughing up repeated mouthfuls or clots
- You have difficulty breathing
- You feel faint, unwell, or symptoms are worsening
Small streaks or flecks of blood should still be checked by a healthcare professional, but larger or increasing amounts should be treated as an emergency.
What happens during emergency care?
Emergency responders and hospital teams focus on:
- Supporting breathing (for example, with oxygen)
- Monitoring vital signs
- Identifying the source of bleeding
- Protecting unaffected areas of the lung where possible
In some cases, procedures such as bronchial artery embolisation may be used to control bleeding.
While waiting for help (general guidance)
If you are waiting for emergency services to arrive, general first-aid principles often focus on maintaining comfort and supporting breathing.
- If possible, try to remain in a position that feels easiest for breathing
- Many patients find that being upright or slightly forward is more comfortable
- Try to keep the airway clear by allowing coughing if needed
The priority is to seek urgent medical help rather than attempting to manage the situation alone.
In an emergency, it may not be possible to adopt an “ideal” position—focus on calling for help.
Why positioning matters
In healthcare settings, positioning is sometimes used to help:
- Keep airways as clear as possible
- Reduce the spread of blood within the lungs
- Maintain breathing while further treatment is arranged
This is based on general principles of lung anatomy and airflow. The aim is not to stop bleeding, but to support breathing.
Many people find it easier to breathe when upright or leaning slightly forward. This may help fluid move out through the mouth rather than further back into the main airways.
Understanding airway safety
In situations where there is bleeding (or sometimes vomiting), the main concern is keeping the airway clear so that air can move in and out of the lungs.
Fluid in the airway can interfere with breathing, which is why emergency care focuses on maintaining airway clearance as well as treating the underlying cause.
Positions that allow fluid to move out of the mouth rather than back into the airway are generally preferred. Many people find being upright or slightly forward helps with this.
If someone becomes unable to remain upright, is very drowsy, or is vomiting, placing them on their side (recovery position) may help keep the airway clear while waiting for emergency services.
This information is general and does not replace emergency care. Always call 999 if symptoms are severe.
What is generally avoided
In clinical practice, certain positions are usually avoided because they may make breathing more difficult.
- Lying flat on the back
- Positions that feel like they worsen breathing
If you feel unsure, prioritise comfort and breathing while waiting for help.
What happens after hospital care?
After an episode of haemoptysis, your clinical team may:
- Investigate the cause of bleeding
- Review your current treatment
- Discuss whether any preventative measures are appropriate
If you have experienced haemoptysis, it may be helpful to ask your team whether you need an individualised plan.
Medications such as tranexamic acid
Some patients may be prescribed tranexamic acid to help reduce bleeding.
If you have been given this medication with clear instructions, it may be intended for use during bleeding episodes. It should only be taken exactly as directed by your clinical team.
Tranexamic acid does not replace the need to seek urgent medical help. If you are coughing up more than a few spots or streaks of blood, or feel unwell or breathless, call 999.
If you are unsure whether to take it during an episode, seek urgent medical advice.
Common Questions
Is coughing up blood always serious?
Any new or unexplained bleeding should be assessed. Larger amounts require urgent attention.
Can I manage this at home?
Significant haemoptysis should not be managed at home. Always seek urgent medical help.
Will it happen again?
This varies between individuals. Your specialist team can advise based on your condition.
When to seek medical help
Call 999 immediately if:
- You are coughing up more than just a few spots or streaks of blood
- You have difficulty breathing
- You feel faint, unwell, or symptoms are worsening
Seek medical advice urgently (NHS 111 or GP) if:
- You notice new or increasing blood in sputum
- You have recurrent or ongoing minor bleeding
Important safety note
This information is for general education only and does not replace medical advice. In an emergency, always seek immediate professional care.
References
- NHS. Coughing up blood (haemoptysis): https://www.nhs.uk/symptoms/coughing-up-blood/
- European Respiratory Society and interventional radiology guidance on haemoptysis
Author and review
Author: National Aspergillosis Centre (Patient Education Team)
Review: Specialist clinicians, Manchester University NHS Foundation Trust
Next review due: March 2027

Muscle Cramps in Aspergillosis (Including ABPA and CPA): Causes, Triggers, and What May Help
Audience: Patients, carers, and non-specialist healthcare professionals
Key Points
- Muscle cramps—especially at night—are commonly reported by people with long-term lung conditions such as allergic bronchopulmonary aspergillosis (ABPA) and chronic pulmonary aspergillosis (CPA).
- There is usually no single cause; cramps often result from a combination of factors including medications, fatigue, hydration, and electrolyte balance.
- In CPA, additional factors such as antifungal therapy and kidney function may play an important role.
- Persistent or worsening cramps should be discussed with a healthcare professional, as some causes are treatable.
Contents
- Overview
- Why do muscle cramps happen?
- How is this linked to aspergillosis and its treatment?
- Additional considerations in chronic pulmonary aspergillosis (CPA)
- Common contributing factors
- What may help reduce cramps
- When to seek medical advice
- Common questions
- References
Overview
Muscle cramps are sudden, involuntary contractions of a muscle that can last from seconds to several minutes. Many people describe them as painful tightening or “locking” of the muscle, often affecting the calves, thighs, feet, or hands.
For people living with aspergillosis, including allergic bronchopulmonary aspergillosis (ABPA) and chronic pulmonary aspergillosis (CPA), cramps are frequently discussed in patient communities. They are particularly common at night and may affect sleep and quality of life.
Importantly, while cramps can be uncomfortable and sometimes severe, they are often manageable once contributing factors are identified.
Why do muscle cramps happen?
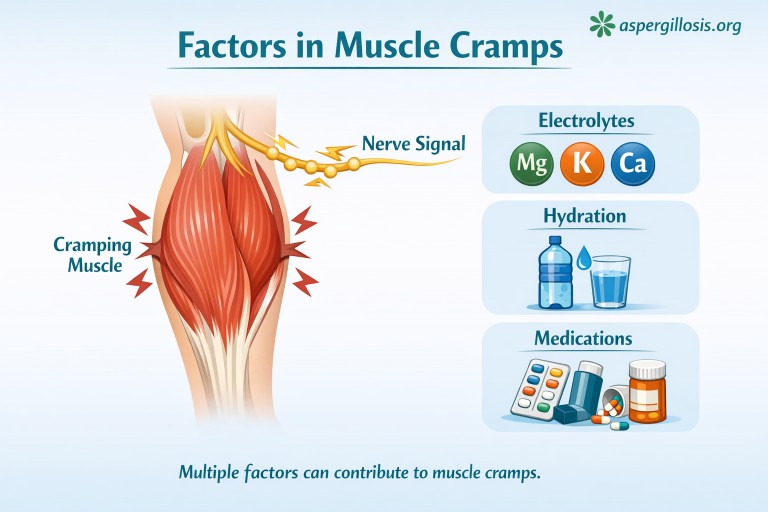
Muscle cramps occur when the normal signals between nerves and muscles become disrupted. This can be influenced by:
- Changes in fluid balance (hydration)
- Electrolyte levels (such as magnesium, potassium, calcium)
- Muscle fatigue or overuse
- Nerve sensitivity or irritation
In many cases, more than one of these factors is involved.
How is this linked to aspergillosis and its treatment?
People with aspergillosis may experience additional factors that increase the likelihood of cramps:
- Medications – some treatments used in lung disease (including antifungals, corticosteroids, and inhalers) may affect muscle function or electrolyte balance
- Chronic inflammation – ongoing inflammation in the body can affect muscles and nerves
- Reduced activity or sudden changes in activity – both inactivity and overexertion can trigger cramps
- Co-existing conditions – such as kidney or hormonal conditions, which can influence electrolyte balance
Because many patients take multiple medications, it can sometimes be difficult to identify a single cause.
Additional considerations in chronic pulmonary aspergillosis (CPA)
People living with chronic pulmonary aspergillosis (CPA) may experience additional factors that increase the likelihood of muscle cramps.
- Long-term antifungal therapy – medications such as azoles (e.g. itraconazole or voriconazole) can affect electrolyte balance or interact with other medicines
- Kidney function – the kidneys play a key role in regulating electrolytes, and even mild changes may contribute to cramping
- Electrolyte imbalance – including magnesium, potassium, and calcium levels, which may fluctuate despite supplementation
- Medication combinations – multiple treatments may have additive effects on muscles or nerves
- Fatigue and reduced conditioning – common in chronic lung disease and may increase susceptibility to cramps
These factors mean that cramps in CPA are often multifactorial and may change over time.
Common Contributing Factors
Based on patient reports and clinical understanding, the following are commonly associated with muscle cramps:
- Physical exertion – especially in physically demanding jobs
- Age-related muscle changes
- Dehydration
- Electrolyte imbalance
- Medication effects
- Poor sleep or positioning
Some people also report cramps affecting multiple muscle groups at the same time, which can feel particularly intense.
What May Help Reduce Cramps
While individual responses vary, some general approaches that people find helpful include:
- Maintaining hydration
- Gentle stretching before bed
- Regular, moderate activity
- Medication review with a clinician or pharmacist
- Balanced nutrition
Important: Supplements such as magnesium are commonly used, but may not be effective for everyone and should be discussed with a healthcare professional—particularly if you have kidney conditions or are taking multiple medications.
When to Seek Medical Advice
You should consider speaking to your GP or specialist team if:
- Cramps are becoming more frequent or severe
- They involve multiple muscle groups regularly
- They are disrupting sleep or daily life
- You have recently started or changed medications
Seek more urgent medical advice if:
- Muscle weakness develops
- There is swelling or redness
- Dark urine or reduced urine output occurs
Common Questions
Are muscle cramps a symptom of aspergillosis?
They are not a defining symptom but are commonly reported, likely due to a combination of treatment effects and general health factors.
Why do cramps happen at night?
Night-time cramps are common and may relate to fatigue, hydration, and circulation changes during rest.
If I take magnesium, shouldn’t cramps stop?
Not necessarily. Muscle cramps often have multiple causes.
Are cramps more important to report in CPA?
Yes—particularly if you are on long-term antifungal treatment or have kidney-related issues, as these may be relevant.
References & Further Reading
- National Institute for Health and Care Excellence (NICE) – Muscle cramps guidance
- UK National Health Service (NHS) – Leg cramps overview
- General clinical literature on electrolyte balance and muscle function
Author & Review Information
Author: Aspergillosis Patient Education Team
Review status: General educational content aligned with UK clinical practice
Disclaimer: This article is for information only and does not replace medical advice. Always consult your healthcare team regarding symptoms or treatment.
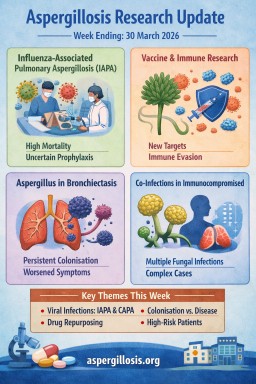
Aspergillosis Research Update: Week Ending: 30 March 2026
Contents
- Key highlights
- 1. Influenza-associated pulmonary aspergillosis (IAPA)
- 2. Aspergillus colonisation in bronchiectasis
- 3. Immune recognition and vaccine development
- 4. Drug repurposing: antiretrovirals and antifungals
- 5. Co-infection in immunocompromised patients
- 6. COVID-19 and CAPA risk
- 7. Paediatric invasive fungal disease trends
- 8. Plastic bronchitis and Aspergillus (contextual)
- 9. Veterinary aspergillosis
- Overall themes this week
- What this means for patients
Key highlights
- Increasing clarity on influenza-associated pulmonary aspergillosis (IAPA) and ongoing uncertainty around prophylaxis
- New insights into immune recognition of Aspergillus relevant to vaccine development
- Evidence that persistent Aspergillus colonisation may worsen bronchiectasis outcomes
- Early-stage research into drug repurposing strategies
- Continued reports of complex co-infections in immunocompromised patients
Paper summaries
Incidence and outcomes of influenza-associated pulmonary aspergillosis and the role of antifungal prophylaxis: a structured literature review
Sedik S, Felber D, Schellongowski P, Salzer HJF, Bellmann R, Muhr T, Auer J, Krippl P, Lux M, Zajic P, Werner M, Bauer N, Watzinger N, Mesaric G, Tinawi Y, Dichtl K, Wolfgruber S, Biswas S, Prattes J, [...] Hoenigl M
Critical Care, 26 March 2026
PMID: 41888868
Summary
This structured review examines how often influenza-associated pulmonary aspergillosis occurs, the outcomes associated with it, and whether antifungal prophylaxis has a role in prevention.
Key points
- IAPA remains a serious complication of influenza in critically ill patients.
- Mortality appears high, particularly in patients requiring intensive respiratory support.
- The evidence for antifungal prophylaxis remains inconclusive.
- Diagnostic uncertainty continues, especially when trying to distinguish colonisation from invasive disease.
Relevance
This is important because it mirrors concerns seen with COVID-19-associated pulmonary aspergillosis and underlines the need for clearer ICU diagnostic and prevention pathways.
Effect of transient versus persistent Aspergillus colonisation on clinical outcomes in bronchiectasis
Michaud A, Jarand J, Thornton CS
ERJ Open Research, 23 March 2026
PMID: 41878279
Summary
This study looks at whether transient and persistent Aspergillus colonisation have different effects on people with bronchiectasis.
Key points
- Persistent colonisation was associated with worse respiratory outcomes.
- Patients with persistent colonisation appeared to have more symptoms and exacerbations.
- Transient colonisation seemed less clinically important.
- The findings sit outside Allergic Bronchopulmonary Aspergillosis (ABPA), which makes them especially interesting.
Relevance
This is one of the most clinically relevant papers this week for chronic lung disease. It suggests Aspergillus in sputum may not always be an incidental finding, especially if it is repeatedly present.
α-1,3-Glucan-Driven Remodeling of the Conidial Cell Wall in an Aspergillus fumigatus Vaccine Strain Alters Innate Immune Recognition
Singh K, Ankur A, Yarava JR, Fernandes CM, Vascelli G, Sulla A, Zelante T, Del Poeta M, Wang T
Journal of the American Chemical Society, 26 March 2026
PMID: 41883285
Summary
This experimental paper explores how changes in the Aspergillus fumigatus conidial cell wall alter how the innate immune system detects the fungus.
Key points
- Changes in α-1,3-glucan altered the structure of the fungal cell wall.
- That remodelling changed how the fungus was recognised by innate immune pathways.
- The work may help inform future vaccine design or immune-targeted therapies.
Relevance
This is early-stage science rather than immediately practice-changing work, but it improves understanding of how Aspergillus may evade immune recognition and how future preventive strategies could be designed.
Synergistic antifungal activity of antiretrovirals with amphotericin B against Aspergillus species
Khan AA, Salama EA, Seleem MN
PLOS One, 25 March 2026
PMID: 41880294
Summary
This laboratory study investigates whether antiretroviral drugs can enhance the antifungal activity of amphotericin B against Aspergillus species.
Key points
- Some antiretrovirals showed synergistic activity with amphotericin B.
- The combination improved inhibition of hyphal growth.
- This raises the possibility of drug repurposing in invasive aspergillosis.
Relevance
This is interesting as a proof-of-concept study. It is not ready for clinical use, but it points toward possible future combination strategies, especially where resistance or toxicity limits current treatment options.
Coexistence of pulmonary aspergillosis and cryptococcosis following treatment for SARS-CoV-2 infection in a kidney transplant recipient: a rare case report and literature review
Hu C, Ying L, Zhan Y, Wang J, Ye J, Lu J, Jin H, Tan X, Gu L, Yao Y, Jiang N
BMC Nephrology, 23 March 2026
PMID: 41872830
Summary
This case report describes a kidney transplant recipient who developed both pulmonary aspergillosis and cryptococcosis after SARS-CoV-2 infection.
Key points
- Demonstrates the potential for multiple opportunistic fungal infections in highly immunosuppressed patients.
- Shows how diagnosis can become particularly complex when symptoms and imaging overlap.
- Reinforces the need for a broad differential diagnosis in transplant recipients and similar high-risk groups.
Relevance
Although a single case, it is a useful reminder that fungal infection in immunocompromised patients may not always be limited to one pathogen, particularly after severe viral infection or intense immunosuppression.
Severe COVID-19 in the Republic of Korea: Epidemiology, Risk Factors, Therapeutics, and Prognostic Models From Nationwide Data
Choi JY
Journal of Korean Medical Science, 23 March 2026
PMID: 41873446
Summary
This review of nationwide Korean data includes discussion of severe COVID-19 complications, including COVID-19-associated pulmonary aspergillosis.
Key points
- There was a trend toward increased COVID-19-associated pulmonary aspergillosis (CAPA).
- Risk appeared higher in patients needing the most advanced respiratory support, including ECMO.
Relevance
This reinforces the continuing importance of CAPA internationally and supports ongoing vigilance in critical care settings, especially where viral lung injury and immunomodulatory treatment intersect.
Temporal Trends and Clinical Outcomes of Pediatric Invasive Fungal Diseases: A Ten-Year Retrospective Study from a Tertiary-Care Center in Thailand
Niyomthammarat C, Meesilpavikkai K, Chintanapakdee W, Sophonphan J, Anugualruengkitt S, Puthanakit T, Jantarabenjakul W
Research Square, 23 March 2026
Status: Preprint v1
Summary
This ten-year retrospective study of paediatric invasive fungal disease includes a substantial number of invasive aspergillosis episodes.
Key points
- Invasive aspergillosis was one of the major fungal disease categories identified.
- Outcomes varied according to underlying condition and likely also the speed of diagnosis and treatment.
Relevance
This paper does not currently have a PubMed listing because it is a preprint rather than a final indexed journal paper, but it still offers useful background on paediatric invasive fungal disease burden.
Initial presentation, etiology and risk factors for adverse outcomes in infection-associated plastic bronchitis in children
Cao H, Liang D, Huang H, He Q, Wu L
Frontiers in Pediatrics, 28 March 2026
PMCID: PMC13021623
Summary
This retrospective paediatric study is not primarily an aspergillosis paper, but it mentions allergic bronchopulmonary aspergillosis among conditions relevant to plastic bronchitis.
Key points
- ABPA appears as part of the broader differential diagnosis in children with this presentation.
- The study mainly concerns airway obstruction and risk factors for poor outcome rather than aspergillosis itself.
Relevance
This has limited direct relevance to most aspergillosis readers, but it is a useful contextual reminder that Aspergillus-related disease can form part of wider airway pathology discussions.
Note: I have not added a PubMed link here because no PMID was supplied. If you want, I can convert this heading to a Europe PMC or PMC link instead.
Aspergillus deflectus-associated disseminated invasive aspergillosis in a German Shepherd dog with discospondylitis: first isolation in Europe
Gernone F, Uva A, Aresu L, Bonfanti U, Ricciardi M, Miglianti M, Barrs VR
Veterinary Research Communications, 25 March 2026
PMID: 41880044
Summary
This veterinary case report documents disseminated invasive aspergillosis caused by Aspergillus deflectus in a German Shepherd dog, reported as the first isolation in Europe.
Key points
- Expands awareness of the range of Aspergillus species capable of causing invasive disease.
- Shows how invasive aspergillosis can present as a disseminated multisystem infection.
Relevance
This is not directly about human disease, but it contributes to the wider ecological and pathogenic picture of Aspergillus species.
Overall themes this week
- Colonisation versus disease remains a major question.
Persistent Aspergillus colonisation may be clinically important in bronchiectasis and should not automatically be dismissed. - Severe viral infection remains a major trigger for invasive aspergillosis.
Both influenza and COVID-19 continue to feature strongly in the literature. - Innovation is active but mostly early-stage.
Vaccine science, immune recognition work, and drug repurposing studies are all progressing, but none are ready to change routine care yet. - Complex patients are at risk of complex fungal disease.
Transplant recipients and critically ill patients remain especially vulnerable to difficult-to-diagnose opportunistic infections.
What this means for patients
- Finding Aspergillus repeatedly in samples may sometimes matter more than a single isolated result.
- Severe viral illness can increase the risk of serious fungal complications in some people.
- Researchers are exploring better ways to prevent and treat aspergillosis, but most of these approaches are still under investigation.
- People with weakened immune systems remain at greatest risk of invasive disease.
Why Headaches Can Occur in Aspergillosis
Last reviewed: March 2026
Key Points
- Headaches are relatively common in people living with aspergillosis, but they usually have multiple contributing causes.
- Common causes include sinus involvement, inflammation, sleep disturbance, and medication effects.
- Antifungal medicines such as itraconazole may improve some symptoms indirectly but can also occasionally cause headaches.
- Patterns (timing, location, triggers) can help identify likely causes, but headaches are rarely due to one factor alone.
- New, severe, or unusual headaches should always be assessed by a healthcare professional.
Table of Contents
- Overview
- Sinus involvement (common cause)
- Inflammation and immune response
- Allergic-type responses (e.g. ABPA)
- Medication effects
- Sleep disturbance and night symptoms
- Breathing and oxygen levels
- General health factors
- Understanding headache patterns
- Common questions
- When to seek medical advice
- Summary
- Author and review
- References
Overview
Many people living with aspergillosis report headaches at some point during their illness. These headaches can vary in type, severity, and timing, and may be confusing—especially when they change over time or seem linked to treatment.
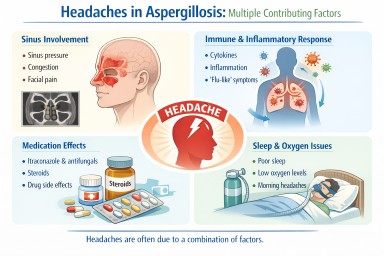
In most cases, headaches are not caused by a single factor. Instead, they reflect a combination of:
- local effects (such as sinus pressure)
- immune system activity
- medication effects
- sleep and general health factors
Understanding these different contributors can help make sense of symptoms and support more informed discussions with your clinical team.
Sinus involvement (common cause)
When Aspergillus affects the sinuses (sometimes called fungal sinusitis), this can directly cause headaches.
This happens because:
- sinus drainage becomes blocked
- pressure builds up in the sinus cavities
- the lining of the sinuses becomes inflamed
Typical features:
- pain or pressure in the forehead, cheeks, or behind the eyes
- worsening when bending forward
- a feeling of fullness or congestion
This is one of the most direct ways aspergillosis can lead to headaches.
Inflammation and immune response
Even when the sinuses are not directly involved, the body’s immune response to fungal material can cause systemic effects.
The immune system releases signalling molecules (such as cytokines) that can:
- increase inflammation
- affect blood vessels
- trigger headache pathways
This type of headache can feel similar to a “flu-like” or inflammatory headache.
Allergic-type responses (e.g. ABPA)
In conditions such as Allergic Bronchopulmonary Aspergillosis (ABPA), the immune system reacts strongly to Aspergillus.
This may involve:
- allergic pathways
- histamine and related mediators
- ongoing airway inflammation
Possible symptoms:
- head pressure or discomfort
- fluctuating headaches
- a “foggy” or unwell feeling
These headaches are often less clearly localised than sinus-related pain.
Medication effects
Some treatments used in aspergillosis can contribute to headaches.
Antifungal medications (e.g. itraconazole):
- headache is a recognised side effect in some people
- effects vary between individuals
Steroids (if prescribed):
- can affect sleep and mood
- may influence blood pressure
- can indirectly contribute to headaches
Medication effects can sometimes overlap with disease-related symptoms, making patterns harder to interpret.
Sleep disturbance and night symptoms
Sleep disruption is common in chronic lung conditions.
Possible contributors include:
- night-time coughing
- breathlessness
- discomfort or anxiety
Poor sleep can lead to:
- morning headaches
- increased sensitivity to pain
- fatigue-related headaches
Breathing and oxygen levels
In some people with more advanced lung involvement:
- oxygen levels may be slightly reduced
- breathing effort may increase
This can contribute to:
- morning headaches
- fatigue and cognitive symptoms
Not all patients experience this, but it is an important factor in some cases.
General health factors
Headaches can also be influenced by general aspects of living with a long-term condition:
- dehydration
- fatigue
- reduced activity levels
- stress or anxiety
These factors can contribute to tension-type headaches or make other headache types more noticeable.
Understanding headache patterns
Looking at patterns can sometimes help identify likely contributors.
- Facial pressure worse on bending: may suggest sinus involvement
- Early morning headaches: may relate to sleep or breathing patterns
- Fluctuating or “wave-like” symptoms: may reflect inflammation or immune activity
- New headaches after starting medication: may be treatment-related
However, these are general observations only and do not replace clinical assessment.
Headaches in Aspergillosis: Interactive Decision Aid
This tool helps patients and carers think about common patterns that can contribute to headaches in aspergillosis. It does not diagnose the cause of a headache.
It is designed to support discussion with a healthcare professional and highlight possible contributors such as sinus involvement, inflammation, medication effects, sleep disturbance, and breathing-related factors.
1. Where is the pain mainly felt?
2. When is it most noticeable?
3. What does it feel like?
4. What other features are present?
5. Are there any red flags?
Possible contributors
This panel highlights common patterns only. It is not a diagnosis and does not replace medical assessment.
Common questions
Are headaches a recognised symptom of aspergillosis?
They can occur, but are usually indirect and caused by associated factors such as sinus disease or inflammation.
Can antifungal treatment improve headaches?
In some cases, yes—if symptoms are linked to fungal-related inflammation. However, antifungals can also occasionally cause headaches as a side effect.
Are “histamine-type” headaches part of aspergillosis?
Some patients describe symptoms in this way, but the underlying mechanism is often more complex than histamine alone.
Why do my headaches change over time?
This is common and may reflect changes in inflammation, treatment, sleep, or overall health.
When to seek medical advice
You should seek medical advice if you experience:
- new or unusually severe headaches
- headaches that are worsening over time
- neurological symptoms (e.g. vision changes, weakness, confusion)
- fever, neck stiffness, or other concerning symptoms
If you are unsure whether your headaches are related to aspergillosis, treatment, or another cause, it is important to discuss this with your healthcare team.
Summary
Headaches in people with aspergillosis are usually caused by a combination of factors rather than a single issue.
The most common contributors include:
- sinus involvement
- immune and inflammatory responses
- sleep disturbance
- medication effects
Understanding patterns and changes over time can be helpful, but medical assessment is important if symptoms are new, severe, or concerning.
Author and review
Prepared for: aspergillosis.org
Audience: Patients and non-specialist readers
Important: This article is for general information only and does not replace individual medical advice.
References
- Patterson TF et al. (2016). Practice Guidelines for the Diagnosis and Management of Aspergillosis.
PMID: 27365388 - Denning DW et al. (2016). Chronic pulmonary aspergillosis guidelines.
PMID: 26699723 - Chakrabarti A et al. (2009). Fungal sinusitis: a categorization and definitional schema.
PMID: 19522756
Why Do My “Histamine” Headaches Improve on Itraconazole?
Last reviewed: March 2026
Key Points
- Itraconazole is an antifungal medicine. It is not an antihistamine.
- Some people notice that symptoms such as headaches, flushing, or a “histamine-type” feeling become shorter or less intense after starting treatment.
- This is most likely because itraconazole reduces the fungal burden and the immune response it triggers, rather than blocking histamine directly.
- Symptoms that happen in the early hours of the morning may also be influenced by the body’s natural day-night rhythm.
- Changes in symptoms can be helpful clues, but headaches can have more than one cause.
Table of Contents
- Overview
- What is itraconazole and how does it work?
- What do people mean by “histamine dump” headaches?
- Why might symptoms improve on itraconazole?
- Why do symptoms often happen at night?
- Does this mean histamine is the main problem?
- Common questions
- When to seek medical advice
- Summary
- Author and review
- References
Overview
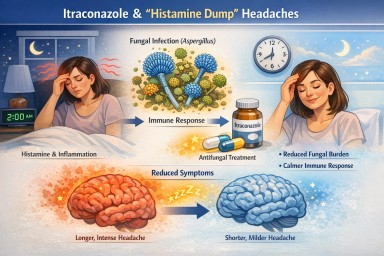
Some people taking itraconazole for non-lung or lung forms of aspergillosis notice that symptoms they describe as “histamine-type” symptoms, such as headaches, flushing, pressure, or a general sense of inflammatory overload, become shorter or less severe.
A typical pattern might be:
- Symptoms start overnight, for example, around 2 am
- Symptoms previously lasted most of the day
- Symptoms are now settling much earlier after starting treatment
This can be confusing, especially when the symptoms feel similar to a histamine reaction. The important point is that itraconazole does not work like an antihistamine, but it can reduce symptoms indirectly if a fungal process is contributing to them.
What is itraconazole and how does it work?
Itraconazole is an antifungal medicine used to treat infections caused by fungi such as Aspergillus.
It works by interfering with the production of ergosterol, an essential part of the fungal cell membrane. This weakens the fungus and helps reduce fungal growth and survival in the body.
As the fungal burden falls, the immune system may be less strongly stimulated, and that can lead to a reduction in inflammation-related symptoms.
So although itraconazole does not block histamine directly, it may reduce the underlying trigger that is causing the body to react.
What do people mean by “histamine dump” headaches?
“Histamine dump” is not a formal medical diagnosis, but some patients use it as a practical way of describing symptoms such as:
- sudden headaches, especially overnight or early in the morning
- flushing or a feeling of heat
- pressure in the head or sinuses
- a sense of being “wired”, agitated, or unwell
These symptoms may involve histamine, but they can also reflect broader inflammation, immune activation, mast cell activity, or other signalling chemicals in the body.
Why might symptoms improve on itraconazole?
If itraconazole is helping, it is most likely doing so indirectly. There are several possible reasons for this.
1. Reduced fungal burden
If fungal material in the body is reduced, there may be less for the immune system to react to. That can mean less inflammatory signalling overall.
2. Reduced immune activation
Fungi can stimulate the immune system in ways that lead to inflammation and, in some people, histamine-related symptoms. If antifungal treatment lowers that stimulus, symptoms may become less intense or settle more quickly.
3. Shorter inflammatory response
Some people find that the symptom still begins, but does not “run on” for as long. For example, a headache that used to last from 2am until late afternoon may now settle by 5am.
Why do symptoms often happen at night?
The body has a natural circadian rhythm, a 24-hour cycle that affects hormones, inflammation, sleep, and immune activity.
- Some inflammatory signals can be more noticeable overnight
- Cortisol rises in the early morning, and helps suppress inflammation
Does this mean histamine is the main problem?
Not necessarily. Symptoms may involve multiple pathways, including immune response to fungi, general inflammation, mast cell activity, and sinus pressure.
Common questions
Does itraconazole act like an antihistamine?
No. It does not block histamine receptors.
Why are my symptoms improving but not gone?
This is common and may reflect partial control of the underlying trigger.
Does this prove Aspergillus is the cause?
No. It suggests a possible link but does not confirm causation.
Will symptoms continue to improve?
Possibly, but responses vary between individuals.
When to seek medical advice
- new or severe headaches
- neurological symptoms (vision, speech, balance)
- worsening or persistent symptoms
- concerns about medication side effects
Summary
Itraconazole does not directly affect histamine but may reduce symptoms by lowering fungal burden and immune activation.
Author and review
Prepared for: aspergillosis.org
Audience: Patients and non-specialist readers
Important: This does not replace individual medical advice.
References
- Patterson TF, Thompson GR 3rd, Denning DW, et al. (2016).
Practice Guidelines for the Diagnosis and Management of Aspergillosis.
View on PubMed (PMID: 27365388) - Denning DW et al. (2016).
Chronic pulmonary aspergillosis guidelines.
View on PubMed (PMID: 26699723) - Barnes PJ, Adcock IM (2009).
Circadian rhythm in airway disease.
View on PubMed (PMID: 19336589) - Stone KD et al. (2010).
IgE, mast cells, and eosinophils.
View on PubMed (PMID: 20176269)
Aspergillosis in Pets: A Practical Guide for Owners
Last reviewed: March 2026
Key Points
- Aspergillosis is an environmental fungal infection, not contagious between pets or people.
- Dogs are most commonly affected, particularly in the nose and sinuses.
- Risk increases with exposure to disturbed soil, compost, and decaying plant material.
- Different animals are affected in different ways depending on behaviour and anatomy.
- Early recognition and veterinary treatment usually lead to good outcomes.
Table of Contents
- What is aspergillosis?
- Which pets are more susceptible?
- Do risks differ between animals?
- Warning signs to look out for
- Environmental risks: what to avoid
- Treatment and management
- Risk to people and other pets
- When to seek veterinary advice
- Common questions
What is aspergillosis?

Aspergillosis is caused by Aspergillus, a group of moulds commonly found in soil, compost, and decaying vegetation. Pets are exposed to these spores regularly in everyday environments.
In dogs, the infection most often affects the nasal passages and sinuses. In other animals, particularly birds, it more commonly affects the lungs.
Important: This is not a contagious disease. It is acquired from the environment.
Which pets are more susceptible?
Dogs
- Most commonly affected species
- Higher risk in long-nosed breeds (e.g. German Shepherds, Collies, Greyhounds)
- Risk increased by sniffing, digging, and outdoor exploration
Cats
- Less commonly affected
- Can develop nasal or sinus infection, occasionally more invasive
Birds
- Most sensitive species
- Infection usually affects the lungs and air sacs
- Risk increased in dusty or poorly ventilated environments
Other animals
- Farm animals (e.g. horses) can be affected, but this is uncommon
- Small pets (rabbits, rodents) are rarely affected
Do risks differ between animals?
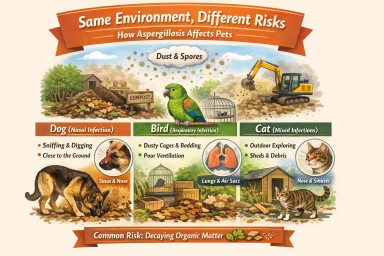
Yes. The same environment can pose different risks depending on how an animal interacts with it.
- Dogs: close to the ground → inhale spores while sniffing or digging
- Cats: roaming behaviour → exposure in gardens, sheds, and debris
- Birds: airborne exposure → sensitive lungs affected in enclosed or dusty spaces
Key insight: The common factor is exposure to fungal spores, but the route of exposure differs between species.
Warning signs to look out for
Dogs (most common presentation)
- Persistent nasal discharge (often one-sided)
- Sneezing
- Nosebleeds
- Pain around the nose
More advanced signs
- Swelling around the nose or eyes
- Loss of pigment or ulceration on the nose
- Lethargy or reduced appetite
Birds
- Breathing difficulty
- Lethargy
- Reduced appetite
Key message: Persistent symptoms—especially nasal discharge or breathing problems—should always be checked by a vet.
Environmental risks: what to avoid
Aspergillus grows in decaying organic material. Risk increases when this material is disturbed and spores become airborne.
Higher-risk environments
- Disturbed soil (construction or garden clearance)
- Rotting leaves, wood, or plant debris
- Compost heaps and garden waste
- Bark chippings or mulch
- Stored hay, straw, or grain
- Dusty sheds, barns, or enclosed spaces
Situations that increase exposure
- Digging or burrowing
- Prolonged sniffing in debris-rich areas
- Dry, windy conditions
- Poor ventilation (especially for birds)
Common factors across all pets
- Decaying organic material
- Disturbance of soil or vegetation
- Dust and airborne particles
- Enclosed or poorly ventilated environments
Simple precautions
- Keep dogs on a lead near disturbed areas
- Avoid allowing pets to dig in compost or debris
- Keep bird enclosures clean and well ventilated
- Allow disturbed sites to settle before use
- Rinse paws and muzzle after muddy walks
Balanced view: These environments are common and most pets are exposed without becoming ill. The aim is to reduce exposure during higher-risk periods.
Treatment and management
Aspergillosis in dogs is usually treatable and often curable.
Typical treatment
- Antifungal medication applied directly into the nasal passages under anaesthetic
- Removal of fungal material (debridement)
Other approaches
- Oral antifungal medication in selected cases
- Supportive care (pain relief, monitoring)
Follow-up is important to ensure the infection has fully cleared.
Risk to people and other pets
- Not contagious between animals or humans
- Healthy people are at very low risk
- Higher-risk individuals are those with lung disease or weakened immune systems
When to seek veterinary advice
- Nasal discharge lasting more than a few days
- Blood from the nose
- Persistent sneezing or discomfort
- Breathing problems (especially in birds)
- Swelling around the face
Early diagnosis improves outcomes significantly.
Common questions
Can pets catch aspergillosis from people?
No. It is acquired from the environment.
Is a damp home a cause?
Damp environments can contain spores, but most cases—especially in dogs—are linked to outdoor exposure.
Is this common?
It is uncommon overall, but a recognised cause of nasal disease in dogs.
Summary
Aspergillosis is an environmental fungal infection that affects different animals in different ways. Dogs are most commonly affected through sniffing contaminated material, while birds are more sensitive to airborne spores in enclosed spaces. Although exposure is common, illness is uncommon, and simple precautions combined with early veterinary care usually lead to good outcomes.
Author: Aspergillosis Patient Support & Education Team
Review: This information is for general guidance only and does not replace veterinary advice. If you are concerned about your pet, please consult your veterinary surgeon.

Why Join an Online Support Group if You Have Aspergillosis?
You are not alone with aspergillosis
Join a friendly online support meeting — no pressure, just listen if you prefer.
Many patients find that even attending once helps them feel more reassured, informed, and supported.
Why Join an Online Support Group if You Have Aspergillosis?
Living with aspergillosis can feel isolating. Many people go for years without meeting another person with the same condition. Family and friends may be supportive, but they may not fully understand what it is like to live with breathlessness, fatigue, treatment side effects, uncertainty, or repeated hospital visits.
That is one reason online support groups can be so valuable. They bring people together who understand, often immediately, many of the challenges that aspergillosis can bring.
Key points
- Online support groups reduce isolation and help patients feel understood
- They offer shared experience alongside emotional support
- They improve confidence and understanding of the condition
- They help patients feel better prepared for appointments
- They are flexible — you can simply listen if you prefer
What changes when people join a support group?
Before joining
- Feeling alone with the condition
- Uncertainty about symptoms
- Limited practical advice
- Low confidence at appointments
- Worry about the future
After joining
- Connection with others who understand
- Better understanding of the condition
- Practical day-to-day coping ideas
- More confidence asking questions
- Feeling more supported and reassured
Why aspergillosis can feel so isolating
Aspergillosis is a relatively rare condition, and many patients never meet someone else with the same diagnosis. Online support groups help bridge that gap by creating a shared space for understanding and connection.
1. You realise you are not alone
Hearing others describe similar symptoms and challenges can be immediately reassuring and reduce feelings of isolation.
2. Shared experience can be deeply reassuring
Support groups provide practical, real-world insight into managing fatigue, pacing, work, and daily life.
3. You may understand your condition better
Listening to others and accessing shared resources helps build confidence and understanding.
4. It can help you feel more confident at appointments
Patients often feel better prepared and more able to ask the right questions.
5. Emotional support matters too
These groups provide encouragement, understanding, and a sense of belonging.
What happens in a typical online support session?
- Friendly welcome — no pressure to speak
- Open discussion — share or listen
- Optional topics — such as fatigue or treatment experiences
- Flexible participation — camera and microphone optional
- Safe, moderated space
Many people attend their first session just to listen — and that is completely fine.
What patients often say
“I wish I had joined sooner. Just hearing others talk made a huge difference.”
“I didn’t speak in my first meeting, but it really helped just listening.”
“It helped me understand my condition and feel more confident.”
Thinking of joining?
You can attend once, listen, and decide if it feels helpful. There is no obligation to continue.
View meeting times and book here:
https://aspergillosis.org/support-meetings/
Meetings are held online using Microsoft Teams. You will receive a joining link after booking.
Bottom line
Online support groups offer connection, reassurance, and understanding. They cannot replace medical care, but they can make living with aspergillosis feel more manageable and less lonely.
Please note: These groups are for support and shared experience. They do not replace advice from your own doctor or specialist team.

Donating Your Body for Medical Research in the UK
This is an uncommon request, but it can be very helpful to researchers. There is no compulsion at all to consider body donation. It is entirely a personal choice. Many people will decide that it is not for them, and that is completely understandable. For those who do wish to explore it, however, body donation can make an important contribution to medical education, training, and research.
What does body donation mean?
In the UK, donating your body means leaving it after death to a medical school or other appropriately licensed institution for anatomical examination, education, training, or research.
You cannot usually donate your body specifically to “aspergillosis research” alone. However, donation may still support work that is highly relevant to people affected by aspergillosis, including:
- lung disease
- infection
- immune responses
- medical training in complex respiratory illness
The most important point: consent must be given in advance
Under UK law, body donation must be arranged before death. This means:
- you must give written consent
- the consent must usually be witnessed
- your family cannot normally make this decision for you after you die
How to arrange body donation
- Choose a medical school
You need to contact a medical school directly. Most only accept donations from their local area. - Request an information pack
The school will explain its process, send consent forms, and set out any restrictions. - Complete the consent forms
Keep copies with your important papers and let your family know your wishes. - Tell your next of kin or executor
They will usually need to contact the medical school promptly after death.
Important to understand
- Not every donation can be accepted. Even if you have registered, a medical school may not be able to accept the body in every circumstance.
- A backup funeral plan is important.
- Body donation is separate from organ donation. They are different systems and require separate arrangements.
Can I ask for donation to help lung or aspergillosis-related research?
You can certainly explain that your interest is in supporting research and education relevant to lung disease, infection, or aspergillosis. However, you cannot usually guarantee exactly how a donated body will be used. Even so, donation may still support education and research that benefits future patients with complex respiratory and fungal conditions.
Where to start: Human Tissue Authority
The best first step is the Human Tissue Authority (HTA), which provides UK guidance and a way to identify the correct medical school for your postcode.
Examples of medical school body donation pages
Please note: contact details and catchment arrangements can change, so it is wise to confirm current information directly on each medical school’s website.
- University of Manchester
Body donation / bequeathals information - University of Liverpool
Human Anatomy Resource Centre body donation page
Email: [email protected]
Tel: 0151 794 5442 - University of Leeds
Bequests information
Email: [email protected]
Tel: 0113 343 4297
Final thought
Donating your body for medical education or research is an unusual and deeply personal decision. There is absolutely no obligation to consider it. But for those who do, it can be a generous and lasting way to support future learning, better care, and research that may help people living with serious conditions, including aspergillosis.
Last reviewed: March 2026
How Inflammation in One Part of the Body Can Affect the Rest of the Body
Last reviewed: 24 March 2026
Audience: Patients, families, and non-specialist clinicians
Author: Aspergillosis.org editorial team
Many people think of inflammation as something that stays in one place: a painful joint, an inflamed lung, an irritated sinus, or a bowel flare. In reality, inflammation is often a whole-body process. Signals released at one site can travel through the blood, nervous system, and immune system, influencing other organs and changing how the body feels and functions overall.
This helps explain why a local health problem can sometimes lead to symptoms that seem much broader, such as fatigue, poor concentration, low mood, loss of appetite, aches, disturbed sleep, or worsening of other long-term conditions.
Key points
- Inflammation is not always confined to one organ or body part.
- Inflamed tissues release chemical messengers that can circulate throughout the body.
- The brain, heart, kidneys, liver, gut, lungs, and immune system all communicate with one another.
- This “cross-talk” can be helpful in short-term illness, but harmful when inflammation becomes prolonged.
- Ongoing inflammation is linked with fatigue, brain fog, low mood, cardiovascular strain, and worsening of other chronic diseases.
Table of contents
- What is inflammation?
- Why inflammation does not always stay local
- How the body communicates during inflammation
- Common whole-body effects of inflammation
- Why this matters in lung disease and aspergillosis
- Acute inflammation versus chronic inflammation
- What can help?
- When to seek medical advice
- Common questions
- References
What is inflammation?
Inflammation is part of the body’s defence system. It is one of the ways the immune system responds to infection, injury, irritation, allergens, or tissue damage. In the short term, inflammation is often helpful. It can help the body fight infection, clear damaged tissue, and begin repair.
But inflammation can also become too strong, too prolonged, or poorly controlled. When that happens, the effects may no longer stay limited to the original problem area.
Why inflammation does not always stay local
When tissue becomes inflamed, immune cells release small signalling proteins called cytokines and other inflammatory mediators. These act like chemical messages. Some stay nearby, but many enter the bloodstream and influence distant organs.
This is why inflammation in one part of the body can sometimes cause:
- tiredness or exhaustion
- feeling unwell or “washed out”
- poor concentration or “brain fog”
- worsening appetite
- sleep disruption
- higher strain on the heart or kidneys
- worsening of other inflammatory conditions
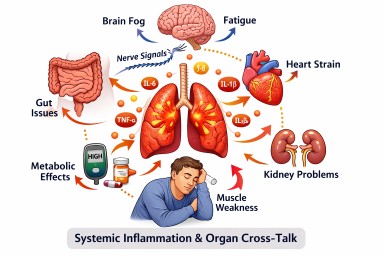
Researchers increasingly describe this as systemic inflammation or organ cross-talk. In other words, organs do not operate in isolation. They are part of an interconnected network.
How the body communicates during inflammation
1. Chemical messengers in the blood
Inflamed tissues can release cytokines such as interleukin-6 (IL-6), interleukin-1 beta (IL-1β), and tumour necrosis factor alpha (TNF-α). These may affect blood vessels, metabolism, the brain, the heart, and other immune cells.
These signals are useful during short-term illness, but if they remain elevated they may contribute to chronic symptoms and long-term health effects.
2. Organ-to-organ immune cross-talk
Modern immunology shows that the gut, liver, lungs, brain, heart, kidneys, and bone marrow can influence one another through immune signalling. A problem in one organ may therefore alter immune behaviour somewhere else.
This can be protective, but it can also become part of a vicious circle, especially in chronic disease.
3. Nerve signalling between the body and brain
Inflammation is not communicated only by blood. The nervous system also plays a role. Signals from inflamed tissues can travel through nerves, including the vagus nerve, to the brain. The brain then responds by adjusting immune activity and body-wide stress responses.
This helps explain why inflammation can affect fatigue, mood, motivation, sleep, and mental clarity.
4. Stress, hormones, and metabolism
Inflammation also interacts with the body’s hormonal and metabolic systems. This can influence energy use, blood sugar regulation, muscle strength, and appetite. Over time, chronic inflammation may put extra strain on the cardiovascular and kidney systems.
Common whole-body effects of inflammation
Fatigue
One of the most common effects of inflammation is fatigue. This is not simply feeling sleepy. It can be a profound lack of physical and mental energy. Many chronic inflammatory illnesses are associated with this kind of exhaustion.
Brain fog and mood changes
Inflammatory signals can affect the brain, contributing to reduced concentration, slowed thinking, low motivation, anxiety, or low mood. This does not mean symptoms are “all in the mind”. It means that immune activity can influence brain function.
Heart and blood vessel effects
Inflammation can make blood vessels less healthy over time and may contribute to a higher cardiovascular risk. This is one reason why long-standing inflammatory diseases are often linked to heart and circulatory problems.
Kidney effects
The kidneys are sensitive to inflammatory stress. In some conditions, long-term systemic inflammation can contribute to kidney damage or worsen existing kidney disease. Kidney disease itself can also increase inflammation, creating a two-way relationship.
Muscle weakness and reduced stamina
Ongoing inflammation can alter how muscles use energy and recover after activity. This may contribute to weakness, reduced exercise tolerance, and slower recovery after exertion.
Why this matters in lung disease and aspergillosis
For people with chronic lung conditions, including some forms of aspergillosis, inflammation in the airways or lungs may have effects beyond breathing alone. The lungs are not separate from the rest of the body.
Inflammation in the lungs may contribute to:
- general fatigue
- poor stamina
- sleep disruption
- brain fog
- loss of appetite
- worsening of other conditions
This can be especially relevant for people living with long-term inflammatory lung disease, repeated infections, allergic inflammation, or complex treatment burdens.
It is also one reason why patients sometimes feel that their symptoms are “bigger” than what would be expected from the lungs alone. Often, that experience is real and biologically plausible.
Acute inflammation versus chronic inflammation
Acute inflammation
This is the short-term response seen with infection, injury, or a sudden flare. It may cause fever, pain, swelling, and marked tiredness. Usually, it settles when the trigger is controlled.
Chronic inflammation
This is lower-grade or persistent inflammation that continues over time. It may be driven by chronic infection, immune dysregulation, ongoing tissue damage, obesity, autoimmune disease, long-term lung disease, or other medical problems. Chronic inflammation is often less dramatic but may have broader long-term effects.
What can help?
The right approach depends on the underlying cause. Broadly, management focuses on:
- identifying and treating the cause of inflammation where possible
- controlling infections or allergic triggers
- optimising treatment of the underlying disease
- supporting sleep, nutrition, and pacing of activity
- monitoring the effects on other organs when relevant
There is rarely a single quick fix for chronic inflammation. Good management usually means looking at the whole person, not just the inflamed organ.
When to seek medical advice
Please seek medical advice if inflammation-related symptoms are worsening or if you develop:
- new or severe breathlessness
- chest pain
- confusion or marked drowsiness
- new swelling, reduced urine output, or signs of dehydration
- persistent fevers
- rapid decline in energy, mobility, or daily functioning
If symptoms are sudden, severe, or alarming, seek urgent medical help.
Common questions
Does inflammation always damage the whole body?
No. Short-term, controlled inflammation is a normal and useful response. Problems are more likely when inflammation is severe, repeated, or persistent.
Can one inflamed organ affect another?
Yes. There is now strong evidence that organs influence one another through immune, vascular, metabolic, and nerve-based pathways.
Can inflammation cause fatigue even if blood tests are not dramatically abnormal?
Yes. Symptoms and blood markers do not always match perfectly. Some people experience substantial fatigue and other systemic symptoms even when routine blood tests are only mildly abnormal or intermittently raised.
Is this relevant to chronic lung disease?
Yes. Lung inflammation can have effects that go beyond breathing, including fatigue, reduced stamina, and wider body effects.
References
- Dou J, et al. The Interplay of Cross-Organ Immune Regulation in Inflammation and Cancer. MedComm. 2025.
- Jin H, Li M, et al. A body–brain circuit that regulates body inflammatory responses. Nature. 2024.
- Katkenov N, et al. Systematic Review on the Role of IL-6 and IL-1β in Cardiovascular Diseases. Journal of Cardiovascular Development and Disease. 2024.
- Nowak KL, et al. Targeting Inflammation in CKD. Current Opinion in Nephrology and Hypertension. 2025.
- Paganin W, et al. Inflammatory biomarkers in depression: a scoping review. 2024.
- Mehta NN, et al. IL-6 and Cardiovascular Risk: A Narrative Review. 2024.
- Che H, et al. Organ cross-talk: molecular mechanisms, biological functions and therapeutic opportunities. 2026.
Disclaimer: This article is for general information and education. It is not a substitute for personalised medical advice. If you are worried about worsening symptoms, new symptoms, or the effect of inflammation on your health, speak to your clinical team.

Aspergillosis Research Update (Week of 16–23 March 2026)
This week’s aspergillosis literature includes important new work on chronic pulmonary aspergillosis (CPA), aspergilloma microbiology, azole resistance evolution, biomarkers, allergic bronchopulmonary aspergillosis (ABPA), and surveillance. As usual, the most clinically useful papers for long-term aspergillosis care are prioritised.
Key points summary
- New evidence suggests that azole persistence and stress tolerance may develop before overt antifungal resistance becomes detectable.
- An aspergilloma appears to be more than a simple fungal ball: it may function as a complex microbial ecosystem involving bacterial adaptation and persistence.
- A new surveillance paper argues for moving beyond Aspergillus fumigatus strain surveillance toward clinical disease surveillance.
- ABPA review literature continues to reflect growing interest in biologic therapies as steroid-sparing treatment.
- A case report reminds clinicians that lung cancer can mimic recurrent aspergillosis, with potential for diagnostic delay.
- Biomarker studies in invasive pulmonary aspergillosis (IPA) are continuing, although most are not yet ready for routine clinical use.
Contents
- Chronic and structural disease
- Antifungal resistance and fungal evolution
- Diagnosis and biomarkers
- ABPA and allergic disease
- Surveillance, epidemiology and environment
- Case reports and diagnostic challenges
- Other relevant papers
1. Chronic and structural disease
Pseudomonas aeruginosa adaptation and persistence in the aspergilloma microbiome revealed by integrated multi-omics
Ribeiro MM, Liu C, Xu JF, Liang S, Goldman GH
G3 (Bethesda), 17 March 2026
PMID: 41843749
This is one of the most interesting papers this week for those focused on CPA and aspergilloma. The authors examine the microbial ecology of aspergilloma and show that Pseudomonas aeruginosa can adapt and persist within this environment. That matters because aspergilloma has often been thought of mainly as a fungal structure, whereas this paper supports the idea that it may be a more complex polymicrobial niche.
The study strengthens the view that chronic pulmonary aspergillosis may involve not only fungal persistence, but also bacterial-fungal interactions, biofilm-like behaviour, and long-term microbial adaptation. This may help explain why some patients remain symptomatic despite antifungal therapy, and why structural lung disease can be so difficult to stabilise.
Why it matters:
- Highly relevant to aspergilloma and CPA.
- Supports growing interest in the lung microbiome and mixed microbial communities.
- May eventually influence how we think about treatment failure, chronic symptoms, and combined antimicrobial strategies.
2. Antifungal resistance and fungal evolution
Evidence that increased azole persistence and stress resistance precede the in vivo evolution of azole resistance in Aspergillus fumigatus
Delbaje E, Pontes L, Savoldi M, Sedik S, Dichtl K, Hoenigl M, Lass-Flörl C, Silva Pereira C, Schreiber AZ, Rokas A, Lu L, Barbosa JCJ, Fill T, Dos Reis TF, Goldman GH
Microbiology Spectrum, 16 March 2026
PMID: 41837673
This is an important resistance paper. The authors provide evidence that azole persistence and stress resistance may emerge before formal azole resistance becomes established in vivo. In other words, the fungus may first become better at surviving azole exposure before developing the classical resistance patterns that laboratories can detect more easily.
That finding is highly relevant to patients with chronic aspergillosis receiving prolonged azole therapy. It suggests that the road to treatment failure may begin earlier than clinicians currently realise, and that traditional susceptibility testing may capture resistance only after important adaptive changes are already underway.
Why it matters:
- Very important for CPA management and long-term triazole treatment.
- Suggests that “susceptible” isolates may still show clinically relevant survival advantages.
- May help explain some cases of gradual loss of treatment response before overt resistance is identified.
Accelerated mutator phenotype in a clinical Aspergillus fumigatus isolate contributes to adaptive evolution
Song Y, Hokken MWJ, Zoll J, Venselaar H, Verweij PE, Melchers WJG, Rhodes J
Emerging Microbes & Infections, 16 March 2026
PMID: 41838943 |
PMCID: PMC12997362
This paper complements the study above. It describes a clinical Aspergillus fumigatus isolate with an accelerated mutator phenotype, meaning it acquires mutations more readily and can therefore adapt more quickly under selective pressure.
For chronic disease, especially where patients receive long courses of azole therapy, this is a concerning but important concept. Some fungal strains may be inherently more capable of adapting during treatment, which could contribute to the emergence of resistance, persistence, or other survival advantages.
Why it matters:
- Relevant to CPA, azole resistance, and treatment monitoring.
- Supports the idea that fungal evolution during chronic infection may be dynamic and patient-specific.
- May eventually help explain why some patients develop resistance more rapidly than others.
3. Diagnosis and biomarkers
Synergistic effects of S100 calcium-binding protein A12 combined with Pentraxin 3 in invasive pulmonary aspergillosis and their clinical application prospects
Zhou X, Hu X, Liu H
Frontiers in Cellular and Infection Microbiology, 20 March 2026
PMCID: PMC12999553
This paper focuses on invasive pulmonary aspergillosis rather than chronic disease. It explores whether combining host biomarkers such as S100A12 and Pentraxin 3 could improve diagnosis and perhaps risk stratification.
As with many biomarker studies, the concept is promising, but the clinical pathway remains uncertain. Biomarkers that reflect the host inflammatory response may ultimately complement fungal biomarkers and imaging, particularly in intensive care or immunocompromised settings.
Why it matters:
- More relevant to IPA than CPA or ABPA.
- Illustrates continued interest in host-response biomarkers.
- Potentially useful in the future, but not immediately practice-changing for routine aspergillosis care.
Diagnostic and prognostic value of serum miR-155 in chronic obstructive pulmonary disease
Wu Y, Zhang K, Zhong R, Wang W, Luo Z, Ma Z, Liang R, Wu X, Zou X
Scientific Reports, 20 March 2026
PMID: 41857172
This is not primarily an aspergillosis paper, but it includes findings relevant to invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease (COPD). The authors report that serum miR-155 levels were lower in IPA than non-IPA patients within their study population.
That is potentially interesting because COPD is a major risk factor for IPA, and there is growing need for better tools to identify invasive fungal disease in such patients. However, this remains exploratory and should be viewed as an early biomarker signal rather than something ready for clinical use.
Why it matters:
- Relevant mainly for COPD-associated IPA risk.
- Adds to the biomarker literature, but is not yet directly applicable in routine practice.
- Limited immediate relevance for CPA and ABPA.
4. ABPA and allergic disease
Allergic bronchopulmonary aspergillosis in internal medicine
Chedal-Anglay C, Martin de Frémont G, Dupin C
Revue de Médecine Interne, 18 March 2026
PMID: 41856838
This review provides an overview of allergic bronchopulmonary aspergillosis, its diagnosis, and treatment. It reiterates that ABPA is a complex and often under-recognised inflammatory lung disease in which treatment may target inflammation, fungal burden, or both.
Importantly, the review reflects current momentum behind biotherapies (biologics) as a growing part of management. This is particularly relevant for patients in whom long-term corticosteroid exposure is problematic, ineffective, or poorly tolerated.
Why it matters:
- A useful review paper for ABPA education and clinical context.
- Supports the continuing move toward steroid-sparing treatment approaches.
- Relevant to current discussions about personalised management pathways in ABPA.
5. Surveillance, epidemiology and environment
From Aspergillus fumigatus pathogen surveillance to Aspergillus disease surveillance
van Grootveld R, van der Beek MT, Buil JB, Schoffelen AF, de Greeff SC, Bosch T, de Boer MGJ, Kuijper EJ, Verweij PE
Journal of Hospital Infection, 18 March 2026
PMID: 41862136
This is an important conceptual paper. Rather than focusing solely on surveillance of Aspergillus fumigatus as an organism, the authors argue for broader Aspergillus disease surveillance. That is a significant distinction: public health and healthcare systems may gain more by tracking actual disease burden, clinical phenotypes, antifungal resistance patterns, and outcomes than by looking only at isolates.
For services interested in national strategy, referral equity, or long-term burden of disease, this paper points toward a more mature surveillance model. It has particular relevance to discussions about CPA burden, referral pathways, registry development, and national service planning.
Why it matters:
- Important for policy, national strategy, and service development.
- Supports the case for stronger data systems around aspergillosis burden and outcomes.
- Potentially relevant to UK service planning and inequity mapping work.
A deep dive into the diversity of the Aspergillus community in the lakes of northern Iran
Kor M, Hedayati M, Abastabar M, Haghani I, Nabili M, Saravani A, Javidnia J, Brandão J, Moazeni M
Frontiers in Public Health, 20 March 2026
PMCID: PMC12999566
This environmental study analyses the diversity of Aspergillus species in lake environments and identifies potentially pathogenic species in water and sediment samples. It is not a clinical paper, but it adds to the wider evidence base showing that environmental reservoirs of Aspergillus are varied and widespread.
Such work contributes to broader understanding of exposure pathways and may be relevant to discussions around damp environments, environmental fungal burden, and risk in vulnerable individuals.
Why it matters:
- Mainly relevant as background epidemiology and environmental context.
- Useful for the bigger public-health picture of Aspergillus exposure.
- Limited immediate clinical impact for patient management.
6. Case reports and diagnostic challenges
Case Report: Lung squamous cell carcinoma mimicking recurrent aspergillosis in systemic lupus erythematosus
Yu J, Tang Y, Tian S, Zhu W, Dai Q
Frontiers in Medicine, 22 March 2026
PMCID: PMC13002587
This case report is particularly valuable because it highlights a major diagnostic pitfall: lung squamous cell carcinoma presenting as recurrent aspergillosis. In patients with complex lung disease or immunological disease, it can be tempting to interpret recurring pulmonary abnormalities through the lens of known infection, inflammation, or prior fungal disease. This paper is a reminder that alternative diagnoses, including malignancy, must remain in view.
For patients with chronic pulmonary abnormalities, repeated “flare” narratives can sometimes delay the recognition of another process. This has strong relevance for clinical vigilance in CPA and related diagnostic pathways.
Why it matters:
- Important reminder that not everything that looks like recurrent aspergillosis is aspergillosis.
- Relevant to diagnostic delay, differential diagnosis, and the overlap between fungal disease and cancer.
- Useful for clinician education and patient-facing discussion about why diagnosis can sometimes take time.
7. Other relevant papers
Genetic background and immune response in paracoccidioidomycosis: A systematic review and meta-analysis of single nucleotide variants
Coelho SDS, Fava WS, Burger E, Pereira-Latini AC, Pontillo A, Venturini J
PLoS Neglected Tropical Diseases, 19 March 2026
PMID: 41855184 |
PMCID: PMC13001940
This paper is not focused on aspergillosis, but it is relevant to the wider theme of host genetic susceptibility to fungal infection. It adds to the growing literature suggesting that inherited immune variation may partly shape vulnerability to invasive mycoses.
A Case of Disseminated Trichophytosis With Vascular Invasion and Multiple Ulcers: Case Report and Literature Review
Fujino K, Umemoto N, Kakurai M, Yabe H, Maekawa T, Harada K, Makimura K, Shibuya K, Demitsu T
Journal of Dermatology, 19 March 2026
PMID: 41853986
This case is relevant mainly because invasive aspergillosis was initially suspected. It is a useful reminder that other invasive fungal infections may enter the differential diagnosis in immunocompromised patients.
IFUCISTRATEGY: A Spanish Survey on the Management of Invasive Fungal Infection (IFI) in Critically Ill Patients
Zaragoza R, Estella Á, Nuvials X, Robles-Plaza M, Casado-Gómez A
Preprints.org, 17 March 2026
Preprint: PPR1166594
This preprint surveys management practices for invasive fungal infection in critically ill patients. It includes references to pulmonary aspergillosis and reflects continuing emphasis on early testing, bronchoalveolar lavage galactomannan, and timely treatment. As a preprint, it should be interpreted cautiously until peer review is complete.
TET2 germline mutation in a patient with sequential lymphoid malignancies: a novel case report
Mao X, Shen K, Wang J, Wang Z, Ao Q, Wang C, Xiao M
Annals of Hematology, 17 March 2026
PMID: 41843166 |
PMCID: PMC12995931
This paper is included as contextual evidence of aspergillosis occurring in a severely immunocompromised setting. Its relevance is mainly in reinforcing the ongoing burden of pulmonary aspergillosis in haematology patients.
Post-transplant Cyclophosphamide Reduces Bronchiolitis Obliterans Syndrome Risk Through Chronic Graft-versus-Host Disease Prevention: A Multicenter Cohort Study
Eggleston RH, Alkhateeb H, Pennington KM, Zhang Z, Torghabeh MH, Hogan WJ, Khera N, Roy V, Durani U, Yadav H
Chest, 16 March 2026
PMID: 41850483
This paper is not principally about aspergillosis, but may be of indirect relevance to post-transplant lung complications and immunosuppressed populations in whom fungal disease risk remains important.
Overall interpretation
This week’s literature is strongest in three areas: chronic disease ecology, fungal adaptation under azole pressure, and diagnostic complexity. For chronic pulmonary aspergillosis in particular, the most notable message is that disease behaviour may be shaped by more than the fungus alone. The aspergilloma paper supports a richer ecological model involving bacterial adaptation, while the resistance papers suggest that fungal survival under treatment may begin to change before classical resistance becomes obvious.
Together, these studies strengthen the case for thinking about chronic aspergillosis as a dynamic long-term host-microbe-environment problem, rather than a static fungal infection. At the same time, the lung cancer case report is an important reminder that persistent or recurrent disease patterns must still be reviewed critically, especially if the clinical course changes.
What seems most relevant this week?
- Most important for CPA: the aspergilloma microbiome paper and the two azole adaptation/resistance papers.
- Most important for ABPA: the ABPA review summarising diagnosis and evolving treatment approaches.
- Most important for service planning: the surveillance paper arguing for disease-level rather than pathogen-only monitoring.
- Most important diagnostic caution: lung cancer masquerading as recurrent aspergillosis.
References
- Ribeiro MM et al. PMID: 41843749
- Delbaje E et al. PMID: 41837673
- Song Y et al. PMID: 41838943
- Zhou X et al. PMCID: PMC12999553
- Wu Y et al. PMID: 41857172
- Chedal-Anglay C et al. PMID: 41856838
- van Grootveld R et al. PMID: 41862136
- Kor M et al. PMCID: PMC12999566
- Yu J et al. PMCID: PMC13002587
- Coelho SDS et al. PMID: 41855184
- Fujino K et al. PMID: 41853986
- Zaragoza R et al. Preprint: PPR1166594
- Mao X et al. PMID: 41843166
- Eggleston RH et al. PMID: 41850483