And Why That Could Be…
by GAtherton
A Guide for People with…
Fibre is no longer just about…
Living with…
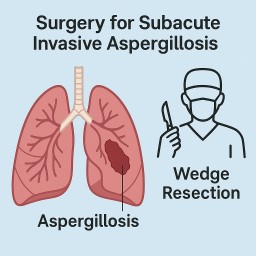
Subacute Invasive…
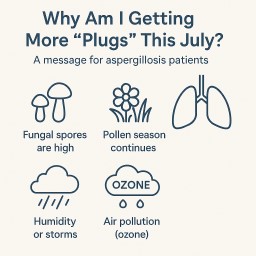
A message for aspergillosis…
Conversation with Tom…
Conversation with Marcela…
For people living with…