Lifestyle & Coping

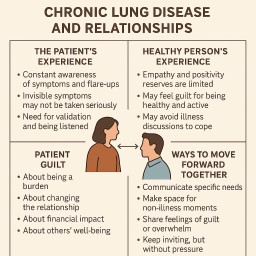
When Caring for a Loved One Becomes Overwhelming: A Guide for Family Carers
Caring for a spouse, parent,…
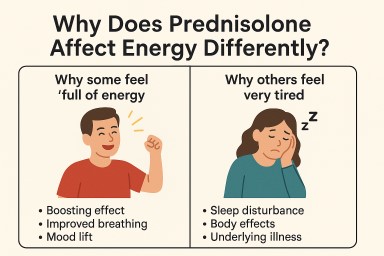
Prednisone, Hydrocortisone, and Adrenal Function – What Patients Need to Know
Why Aspergillosis Patients…

Why It Can Be Hard to Clear Carbon Dioxide (CO₂) From the Lungs in Aspergillosis
When we breathe, oxygen comes…