Question: “I have…
by GAtherton
People living with chronic…
In this compelling personal…
Alison shared something that…
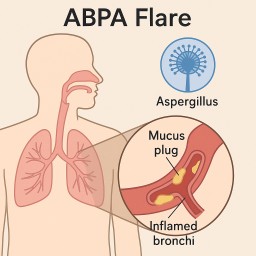
Many people with…
Information for people living…
Living with aspergillosis…