Treatment


💊 General Strategies to Reduce Antimicrobial Resistance in Clinical Practice
1. IV to Oral Switch (IVOS)…


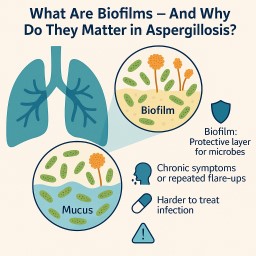
Article 4: Why This New Information on Biofilms Can Be Reassuring — Not Frightening
💬 A Message to Patients: Why…
📝 Article 3: When Microbes Work Together – Aspergillus, Pseudomonas, and Lung Inflammation
🤝 Not all microbes are rivals…