Treatment


🫁 Mucus Plugging in Aspergillosis: What It Is, Why It Happens, and What It Means
For patients with ABPA, CPA,…
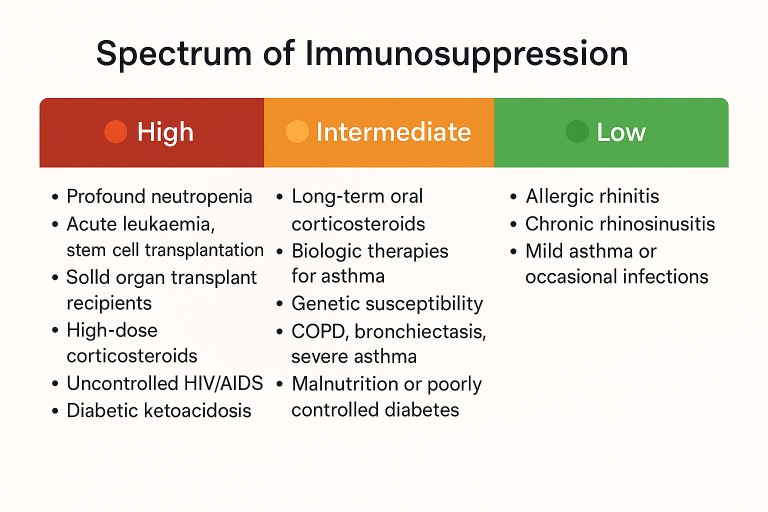
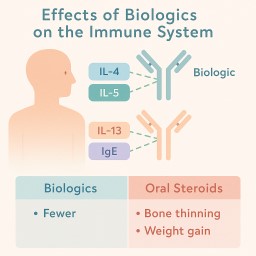
🛡️ Understanding Your Risk: Aspergillosis, Steroids, and the Immune System
If you’ve been diagnosed with…

🫁 Understanding Bronchiectasis, COPD, and Aspergillosis: What Patients Need to Know
Living with a lung condition…