Living with Aspergillosis

When Sleep Won’t Come: Coping with Anxiety and Restless Nights in Aspergillosis
“My GP prescribed 5 mg…

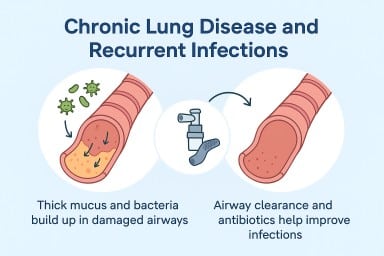
🩵 Coughing and Aspergillosis: Why You Might Still Cough Even When You Feel Well
Many people living with…


“My GP prescribed 5 mg…
Many people living with…