In this compelling personal…
by GAtherton
🧬 Focus Review — Chronic…
Alison shared something that…
Many people with asthma, ABPA…
Many people with…
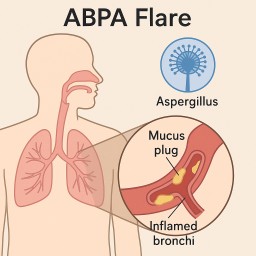
(for ABPA, severe allergic…
Many patients with ABPA,…