Living with Aspergillosis

Managing fatigue and energy in aspergillosis and allergic fungal lung disease
Key points Many people with…
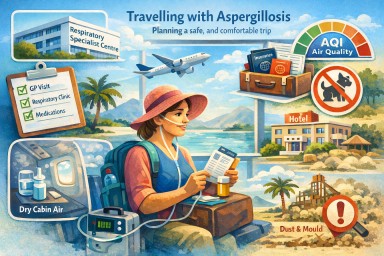
Travelling with Aspergillosis: A Comprehensive Guide to Safe and Stable Travel
This guide is for people…




Key points Many people with…
This guide is for people…