by GAtherton
Patients presenting with…
Last reviewed: March 2026…
Last reviewed: 20 March……
Last reviewed: 18 March 2026…
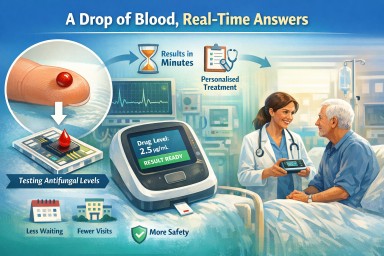
How new diagnostic…