Diagnostics
Systemic fungal infections: why speed, diagnosis and stewardship matter
Systemic fungal infections —…

Can blood tests help predict if chronic pulmonary aspergillosis will come back?
This study from the National…
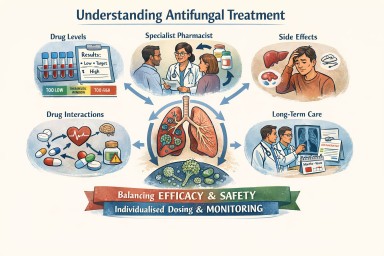




Beyond guidelines: what do I need to know when dealing with fungal diagnostics?
Cornelia Lass-Flörl. Clinical…

Understanding Aspergillosis Through Imaging: A Guide for Patients and Non-Specialist Clinicians
Imaging — especially chest…
