Your Guide to Lung Function Tests: For Patients with Aspergillosis, Severe Asthma, Bronchiectasis, COPD, and Other Lung Conditions
💊 Why Lung Function Testing Matters
Lung function tests (also called pulmonary function tests or PFTs) are vital for understanding how your lungs are working and how your condition is progressing. If you have:
- Aspergillosis (e.g. ABPA, CPA)
- Severe or allergic asthma
- Bronchiectasis
- Chronic Obstructive Pulmonary Disease (COPD)
- or another long-term lung disease
you may be asked to perform one or more of these tests.
Each test looks at a different part of how your lungs function: how well air moves in and out, how oxygen transfers to your blood, how inflamed your airways are, and how your lungs respond to treatment.
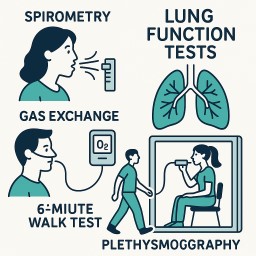
🌬️ Key Lung Function Tests Explained
1. Spirometry
What it does: Measures how much air you can breathe out and how fast you can do it.
Key numbers:
- FEV1: How much air you can blow out in one second
- FVC: Total amount of air you blow out
- FEV1/FVC ratio: Helps detect airflow obstruction
Useful for: Asthma, ABPA, COPD, CPA, bronchiectasis
2. Bronchodilator Reversibility Test
What it does: Compares spirometry before and after taking an inhaler to see if your airways improve.
What it means: A big improvement suggests asthma or ABPA.
3. FeNO (Fractional Exhaled Nitric Oxide)
What it does: Measures airway inflammation by detecting nitric oxide in your breath.
What it means: High levels = eosinophilic inflammation, common in ABPA, asthma.
4. Gas Transfer Test (DLCO/TLCO)
What it does: Measures how well gases like oxygen pass from your lungs into your bloodstream.
What it means: Reduced in CPA, fibrosis, and emphysema. May be normal in asthma or early ABPA.
5. Lung Volume Tests (Plethysmography)
What it does: Estimates total lung capacity and detects air trapping.
How it works: You sit in a sealed cabin and breathe through a tube while pressure and volume are measured (Boyle’s Law).
What it shows:
- High RV/TLC: Air trapping (asthma, CPA)
- Low TLC: Restriction (fibrosis)
6. Peak Flow Monitoring
What it does: Tracks daily variations in how fast you can blow air out.
Useful for: Monitoring asthma, ABPA over time at home.
7. 6-Minute Walk Test + Oxygen Monitoring
What it does: Checks how well you maintain oxygen during activity.
What it shows: Exercise capacity, oxygen needs in CPA, ABPA, fibrosis.
🤔 Are the Numbers Something to Worry About?
Not in isolation. These numbers are pieces of the puzzle, not the whole story.
Your doctor will consider:
- Your symptoms
- Scan results
- Blood markers (e.g. IgE, eosinophils)
- Trends over time
Even if a number seems low, it may not be a concern unless it’s worsening, linked with new symptoms, or part of a larger change.
The key is the pattern over time, and how well you’re functioning in daily life.
🚀 How These Tests Guide Your Treatment
These tests help your team:
- Decide whether your condition is asthma, ABPA, CPA, bronchiectasis, etc.
- Monitor response to inhalers, antifungals, biologics, or steroids
- Adjust or escalate treatment
- Plan oxygen support, pulmonary rehab, or surgery if needed
📊 Summary Table
| Test | What it Measures | Helpful in... |
|---|---|---|
| Spirometry | Airflow (FEV1, FVC) | Asthma, ABPA, CPA, COPD, bronchiectasis |
| Bronchodilator Test | Reversibility of obstruction | Asthma, ABPA |
| FeNO | Airway inflammation (eosinophils) | ABPA, allergic asthma |
| Gas Transfer (DLCO) | Oxygen movement from lungs to blood | CPA, fibrosis, emphysema |
| Lung Volumes | Air trapping, hyperinflation | CPA, asthma, bronchiectasis |
| Peak Flow | Daily airflow changes | Asthma, ABPA |
| 6-Min Walk + O2 | Oxygen levels during activity | CPA, ABPA, fibrosis |
✨ Final Word
Lung function tests can feel unfamiliar, but they are powerful tools for understanding your condition and improving your care. They help build a clearer picture — not of how "bad" your lungs are, but of how they are changing and what support you need.
Always ask your team to explain your results and what they mean for your treatment. You are the expert in how your body feels — and these tests help your team support you better.

🫁 Mucus Plugging in Aspergillosis: What It Is, Why It Happens, and What It Means
For patients with ABPA, CPA, Aspergillus bronchitis, or asthma
🔍 What Is a Mucus Plug?
A mucus plug is a thick clump of sticky mucus that becomes trapped in your lungs. It can block airways, cause coughing, and make breathing more difficult. In people with aspergillosis, this is common — but the type, location, and cause of the mucus can vary.
🧪 What Causes Mucus Plugging?
Your lungs naturally make mucus to protect against germs and irritants. But in fungal or allergic lung disease, this mucus may:
-
Be produced in excess
-
Become too thick or sticky
-
Get trapped due to airway damage
Aspergillosis-related causes include:
-
ABPA (Allergic Bronchopulmonary Aspergillosis) – inflammation causes thick, sticky mucus
-
Aspergillus bronchitis – fungus lives in mucus, producing biofilms
-
CPA (Chronic Pulmonary Aspergillosis) – may lead to mucus due to structural damage
-
Bronchiectasis – airways are widened and can no longer clear mucus properly
🧬 Are All Mucus Plugs the Same?
No. Mucus plugs vary in colour, texture, cause, and treatment. Here's how they differ:
| Type of Plug | What You Might See | What It Could Mean | Common in... |
|---|---|---|---|
| Sticky, stringy | Clear/yellow, like glue | Allergic inflammation | ABPA, asthma |
| Rubbery or solid | Brown, rubbery, “slug-like” | Allergic + fungal mix | ABPA, Aspergillus bronchitis |
| Green or smelly | Thick, foul-smelling | Infection (bacteria) | Bronchiectasis |
| Foamy or frothy | Clear/white, bubbly | Non-infectious irritation | COPD, asthma |
| Black or speckled | May contain fungal specks | Fungal growth | CPA, fungal bronchitis |
🖼️ What Do Mucus Plugs Look Like on a CT Scan?
Below are real examples of CT scan findings showing mucus plugging in different forms of aspergillosis and related conditions.
🧷 1. Finger-in-glove sign (ABPA)
Mucus in large airways appears like fingers inside a glove. This is common in allergic fungal airway disease.
➡ Seen in: ABPA, bronchiectasis with fungal colonisation
📍 Note: Branching tubular opacities filled with mucus.
🌿 2. Tree-in-bud pattern
Small airway blockage — plugs in the tiniest branches of the lungs. Common in infection, inflammation, and Aspergillus bronchitis.
➡ Seen in: Aspergillus bronchitis, asthma, CPA with superinfection
📍 Note: Tiny dots and lines in a tree-like shape.
🧱 3. Lung collapse (atelectasis) from plug
A large mucus plug can block a main airway, causing collapse of part of the lung.
➡ Seen in: Severe ABPA, CPA, patients with weakened cough reflex
📍 Note: Whiteout of part of lung where plug is blocking airflow.
📸 Example CT Findings

1. Bronchiectasis + mucus plug
Area in the left lower lung shows dilated bronchi filled with mucus—classic for bronchiectasis with mucoid impaction

2. Extensive bronchiectasis with plugs
Widespread thick-walled airway dilatation accompanied by mucus plugs (black arrows) and consolidation (black arrowheads)

3. Luminal plugging in small airways
Subtle luminal opacities in peripheral bronchi—the “tree‑in‑bud” pattern common in asthma, COPD, and infections.

4. Atelectasis (part of the lung has collapsed or isn’t fully inflating) due to mucus plugging
Consolidation and small airway blockage leading to lung collapse, highlighted by arrows in the upper lobe.
💡 Clinical Takeaways
| Feature | What it indicates |
|---|---|
| Mucoid impaction | Large airway fungal/allergic plugs (e.g., ABPA) or bronchiectasis |
| Tree‑in‑bud | Small-airway infection/inflammation (e.g., TB, PCD, asthma) |
| Atelectasis | Complete blockage, leading to collapse and consolidation |
| Persistent luminal plugs | Associated with worse airflow obstruction and symptoms in COPD/asthma |
✅ Next Steps / Applications
-
These CT examples are valuable for educational use—they illustrate the different patterns seen in mucus plugging across disease types.
-
Radiologists often use these signs to help diagnose and tailor management (infection, allergy, structural lung disease).
-
If your patients or students need simplified visuals, these scans paired with annotations (e.g., arrows, labels) can make great teaching tools.
🧠 What Does It Feel Like?
People often say:
“It felt like something was stuck and wouldn’t come out.”
“I finally coughed up a rubbery strand — like glue.”
“Once it cleared, I could breathe better instantly.”
🧼 How Are Mucus Plugs Treated?
Treatment depends on the underlying cause:
✅ Medications
-
Steroids – reduce inflammation in ABPA and asthma
-
Antifungals – lower fungal load (e.g., itraconazole, posaconazole)
-
Mucolytics – thin mucus (e.g., carbocisteine, hypertonic saline)
-
Antibiotics – treat bacterial infections
✅ Airway Clearance Techniques
-
Respiratory physio – helps you learn how to shift mucus
-
Devices – flutter valve, PEP mask, Acapella
-
Inhaled/nebulised therapy – opens airways and loosens plugs
⚠️ Always speak to your clinical team before starting a new technique.
🧪 Can Coughing Up a Plug Help Diagnosis?
Yes! If you cough up a rubbery, large, or unusual plug, it can be:
-
Tested for fungus, bacteria, or allergy cells (eosinophils)
-
Sent for culture to detect Aspergillus
-
Helpful in guiding or confirming diagnosis of ABPA or Aspergillus bronchitis
👣 Key Points for Aspergillosis Patients
| Question | Answer |
|---|---|
| Is mucus plugging common? | Yes, especially in ABPA, CPA, and bronchiectasis |
| Are all mucus plugs the same? | No – they vary in size, shape, colour, and cause |
| What should I do if I cough one up? | Tell your doctor – it may be useful to test |
| Can it be seen on scans? | Yes – CT can show where plugs are and how severe |
| Can it be treated? | Yes – treatments include steroids, antifungals, mucolytics, and physio |
🩺 Why an Accurate Diagnosis Matters in Aspergillosis
If you've been told you have aspergillosis — or one of its forms like ABPA or CPA — you may wonder:
"Why does the exact diagnosis matter?"
Isn’t treatment just treatment?
Actually, no. In aspergillosis, getting the right diagnosis makes a huge difference to your care, safety, and long-term health.
This article explains why an accurate diagnosis is essential – not just for treatment, but also for recovery, monitoring, access to specialist care, and living well with the condition.
🔍 What Are ABPA and CPA?
Both ABPA and CPA are caused by the Aspergillus mould, but they affect the body in very different ways:
| Condition | Description |
|---|---|
| ABPA (Allergic Bronchopulmonary Aspergillosis) | An allergic reaction to Aspergillus in the lungs. Most common in people with asthma or cystic fibrosis. |
| CPA (Chronic Pulmonary Aspergillosis) | A chronic lung infection with Aspergillus. Often seen in people with damaged lungs (e.g. past TB, COPD, bronchiectasis). |
Because the symptoms can overlap (like coughing, mucus, or fatigue), it's not always easy to tell them apart — but the treatments are completely different.
🎯 Why Accurate Diagnosis is So Important
1. ✅ Get the Right Treatment
Different types of aspergillosis need very different medicines.
| Diagnosis | Main Treatment | Notes |
|---|---|---|
| ABPA | Steroids (e.g. prednisolone), sometimes antifungals (like itraconazole) | Helps control inflammation and allergy |
| CPA | Long-term antifungals (e.g. itraconazole, voriconazole, posaconazole) | Steroids may make CPA worse |
A wrong diagnosis can lead to the wrong treatment — and that can delay recovery or cause harm.
2. 📆 Plan Your Long-Term Care
Each condition has its own journey:
-
ABPA tends to flare up and settle down, often alongside asthma.
-
CPA is usually chronic and progressive, slowly damaging the lungs if untreated.
Knowing your diagnosis helps your doctors decide:
-
How often to scan your lungs (CT or X-rays)
-
What blood tests to monitor (e.g. IgE for ABPA, IgG for CPA)
-
How long to continue medication
-
What symptoms need urgent review
3. ⚠️ Avoid Side Effects and Harm
If you're given steroids for the wrong condition (e.g. CPA), they can:
-
Weaken your immune system
-
Let the fungal infection get worse
-
Increase the risk of diabetes, weight gain, or bone thinning
And if you’re given antifungals for ABPA without treating the allergy side, you might still keep having flare-ups.
A correct diagnosis helps your team weigh up risks and benefits — and adjust safely.
4. 🏥 Access the Right Specialist Services
In the UK, some treatments are only available for specific diagnoses:
-
Biologic drugs like omalizumab or mepolizumab are only available for severe ABPA under strict NHS criteria.
-
Long-term antifungal treatment for CPA is provided by highly specialised services, such as the National Aspergillosis Centre in Manchester.
Without the right diagnosis on record, access to these treatments may be delayed or blocked.
5. 🧭 Understand What to Expect
An accurate diagnosis helps you understand:
-
What symptoms are normal, and what should be reported
-
Whether your condition is likely to get better, stay the same, or slowly worsen
-
What lifestyle changes, home monitoring, or support groups might help
It also allows your care team to link you to others with similar conditions — for advice, reassurance, and shared experiences.
🧪 What Tests Help Make the Diagnosis?
Your specialist may request:
-
Blood tests (e.g. IgE, IgG antibodies to Aspergillus)
-
CT scans to look at the shape of your lungs
-
Sputum or bronchoscopy samples to grow or detect the fungus
-
Breathing tests (lung function) to assess airflow and trapping
These help build a full picture — no one test is enough on its own.
💬 In Summary
“Aspergillosis” is an umbrella term — but the exact type you have really matters.
Getting the correct diagnosis helps ensure:
-
🧬 You get the most effective treatment
-
📊 You avoid unnecessary harm
-
📆 You have the right follow-up plan
-
🧠 You understand your condition better
-
🩺 You can access the right NHS services
If you're not sure which type of aspergillosis you have — or you feel your diagnosis hasn’t been reviewed in a while — speak to your GP or respiratory team.

🫁 Understanding Bronchiectasis, COPD, and Aspergillosis: What Patients Need to Know
Living with a lung condition can be confusing — especially when the symptoms of bronchiectasis, COPD, and aspergillosis are so similar. This guide explains the differences, how they are diagnosed, and why many people are wrongly diagnosed (or underdiagnosed) at first.
🌬️ What Are These Conditions?
Bronchiectasis
A condition where the airways become damaged, widened, and scarred, often from past infections, immune problems, or conditions like ABPA or CPA. This makes it hard to clear mucus, leading to regular infections.
COPD (Chronic Obstructive Pulmonary Disease)
A group of conditions — including emphysema and chronic bronchitis — that cause narrowed airways and damaged air sacs. Most often caused by smoking or long-term exposure to fumes or dust.
Aspergillosis
An infection or allergic reaction caused by the fungus Aspergillus. Types include:
-
ABPA (allergic bronchopulmonary aspergillosis) — mostly in asthma or bronchiectasis
-
CPA (chronic pulmonary aspergillosis) — causes lung cavities and fungal balls
-
Aspergillus bronchitis — low-grade infection in people with bronchiectasis
🔄 Shared Symptoms
All three can cause:
| Symptom | Bronchiectasis | COPD | Aspergillosis |
|---|---|---|---|
| Chronic cough | ✅ | ✅ | ✅ |
| Sputum (phlegm) | ✅ (often a lot) | ✅ (varies) | ✅ (sticky, sometimes brown) |
| Breathlessness | ✅ | ✅ | ✅ |
| Recurrent infections | ✅ | ✅ | ✅ |
| Fatigue | ✅ | ✅ | ✅ |
| Wheezing | Sometimes | ✅ | ✅ in ABPA |
| Coughing blood (haemoptysis) | ✅ | ⚠️ | ✅ (especially in CPA) |
Because the symptoms are so similar, many people with aspergillosis are first told they have COPD or bronchiectasis until further tests are done.
🖥️ How Are They Diagnosed?
🧪 Tests Used
| Test | Helps Diagnose |
|---|---|
| Spirometry (lung function) | COPD or asthma (airflow obstruction) |
| High-resolution CT scan | Bronchiectasis, CPA, emphysema |
| Aspergillus IgG & IgE blood tests | CPA (IgG), ABPA (IgE) |
| Sputum culture or PCR | Finds Aspergillus or bacterial infections |
| Eosinophil count | High in ABPA |
| Chest X-ray | May show cavities, but CT is better |
🫁 CT Scan Signs: What Do Radiologists Look For?
| Feature | Bronchiectasis | COPD | CPA / Aspergillosis |
|---|---|---|---|
| Airway shape | Widened, thickened (signet-ring sign) | Narrowed or normal | May have overlapping bronchiectasis |
| Lung tissue | Scarring, mucus plugging | Blackened areas (emphysema) | Cavities, fungal balls, fibrosis |
| Mucus | Often present | Sometimes present | Mucus or fungus in airways |
| Other signs | Tree-in-bud, cystic changes | Air trapping, flattened diaphragm | Thickened cavity walls, pleural changes |
💨 What Are Air Trapping and Hyperinflation?
These are signs that air is getting stuck in the lungs — common in asthma, COPD, ABPA, and sometimes CPA.
🔹 Air trapping
Air gets into the lungs but can’t get out fully. You may feel like you can’t finish exhaling.
-
Seen on CT scan as dark areas during breathing out.
-
Lung function tests show high residual volume (RV).
-
Common in asthma, ABPA, bronchiectasis, and COPD.
🔹 Hyperinflation
The lungs are permanently overfilled with air, even when you’re not trying to breathe in.
-
Seen on CT/X-ray as large lungs, flattened diaphragm, and horizontal ribs.
-
Lung function shows high total lung capacity (TLC).
-
Common in emphysema, severe asthma, and ABPA.
Why it matters: Both conditions make breathing harder and less efficient, especially when active. Treatment like inhalers, antifungals, airway clearance, or biologics may help.
💊 Treatment Approaches
| Treatment | Bronchiectasis | COPD | Aspergillosis |
|---|---|---|---|
| Airway clearance physiotherapy | ✅ Essential | Sometimes | ✅ Often vital |
| Antibiotics | ✅ Regularly used | During flares | ✅ For Aspergillus bronchitis/CPA |
| Inhalers (bronchodilators) | Sometimes helpful | ✅ Core treatment | ✅ In ABPA if asthma is present |
| Steroids | In flares or ABPA | ✅ Often | ✅ In ABPA |
| Antifungals (e.g. itraconazole, voriconazole) | ❌ Not routine | ❌ | ✅ Main treatment for CPA/ABPA |
| Pulmonary rehab | ✅ | ✅ | ✅ May help fatigue/breathlessness |
| Oxygen | Rare | ✅ In advanced disease | ✅ In some advanced cases |
🧠 Why It’s Complicated
Many patients are misdiagnosed at first:
-
Aspergillosis can develop on top of COPD or bronchiectasis
-
A long delay in diagnosis is common
-
Some people have all three conditions, or overlapping features (e.g. COPD + ABPA)
That’s why blood tests and CT scans are so important — symptoms alone aren’t enough.
✅ Summary Table
| Feature | Bronchiectasis | COPD | Aspergillosis |
|---|---|---|---|
| Cause | Infection, immune issues | Smoking, pollutants | Fungal allergy or infection |
| Airway problem | Widened, mucus-filled | Narrowed, damaged sacs | Cavities, fungus growth or allergy |
| Diagnostic test | CT scan | Spirometry | CT + Aspergillus IgG/IgE |
| Key treatment | Clearance + antibiotics | Inhalers, steroids | Antifungals ± steroids |
💬 What Should I Ask My Doctor?
-
Could my symptoms be due to more than one condition?
-
Have I had a CT scan and Aspergillus blood tests?
-
Should I be seen by a specialist centre (e.g. for ABPA or CPA)?
-
Am I using the right inhalers or physiotherapy?
-
Could I benefit from a sputum test or antifungal treatment?

🩺 Lung Function Tests Explained: What They Tell Us About Asthma, COPD, Bronchiectasis, and Aspergillosis
If you’re living with a lung condition like asthma, COPD, bronchiectasis, or aspergillosis, you may be asked to have a lung function test. These tests help your medical team understand how well your lungs are working — and how best to treat you.
🌬️ What Are Lung Function Tests?
Lung function tests (also called pulmonary function tests) measure:
-
How fast and deeply you can breathe
-
How well your lungs move oxygen into your blood
-
How much air gets trapped in your lungs
🔬 Main Tests and What They Measure
| Test | What It Measures | Why It Matters |
|---|---|---|
| Spirometry | Speed and volume of air breathed out | Shows obstruction or reversibility (e.g. in asthma) |
| Lung volumes | Total size of the lungs and air left after exhaling | Detects air trapping and hyperinflation |
| Gas transfer (DLCO) | How well gases pass from lungs to blood | Can show scarring, emphysema, or CPA |
| Bronchodilator test | Measures response to inhaler | Helps diagnose asthma or ABPA |
🧠 What Do These Tests Tell Us?
Here’s how different conditions show up in lung function testing:
🟢 Asthma
-
Airways are narrowed, but often improve with inhalers.
-
Shows obstruction that improves significantly after a bronchodilator (reversible).
-
Lung volumes usually normal; DLCO often normal or high.
🔵 COPD
-
Shows irreversible obstruction — lungs are stiff and narrowed.
-
Often shows air trapping and hyperinflation.
-
DLCO is reduced, especially in emphysema.
🟠 Bronchiectasis
-
May show mild-to-moderate obstruction or mixed patterns.
-
Sometimes reversible, depending on overlapping asthma or infection.
-
Lung volumes and DLCO often normal unless CPA or emphysema is also present.
🟣 Aspergillosis
-
ABPA: Like asthma — obstruction, often with reversibility, air trapping, high IgE and eosinophils.
-
CPA: May cause a restrictive pattern (lower lung volumes) or reduced DLCO if fibrosis or cavities are present.
-
Aspergillus bronchitis: May look like bronchiectasis with some obstruction.
💨 What Is Air Trapping?
Air trapping happens when you breathe in, but can’t get all the air back out. Some air stays stuck in the lungs.
| Sign | What It Means |
|---|---|
| High residual volume (RV) | Too much air remains after breathing out |
| Expiratory CT scan shows dark areas | Parts of the lungs aren’t emptying properly |
Common in:
-
Asthma
-
ABPA
-
Bronchiectasis
-
COPD
🎈 What Is Hyperinflation?
Hyperinflation means your lungs are constantly overfilled with air — not just trapped temporarily, but stretched long-term.
| Sign | What It Means |
|---|---|
| High total lung capacity (TLC) | Lungs are too large due to long-term air trapping |
| Flattened diaphragm | Lungs are pressing downward on breathing muscles |
Common in:
-
Severe asthma
-
Emphysema (COPD)
-
ABPA (when uncontrolled)
📊 Summary Table
| Condition | Common Lung Test Features |
|---|---|
| Asthma | Obstruction, reversible, normal DLCO |
| ABPA | Obstruction, reversible, air trapping, high IgE |
| COPD | Fixed obstruction, hyperinflation, low DLCO |
| Bronchiectasis | Variable obstruction, sometimes reversible |
| CPA | Restriction or mixed pattern, reduced DLCO |
| Aspergillus bronchitis | Similar to bronchiectasis, sputum positive for fungus |
💬 Why These Tests Matter
-
They help distinguish what’s causing your symptoms.
-
They track whether treatment is working (inhalers, steroids, antifungals).
-
They identify complications like scarring, cavities, or fungal infection.
-
They help guide eligibility for biologic drugs or oxygen therapy.
📣 Ask Your Doctor:
-
Have I had a bronchodilator response test?
-
Do I have air trapping or hyperinflation?
-
Should we test for Aspergillus (IgG, IgE, sputum)?
-
Would a CT scan add helpful detail?

🟣 Aspergillus Bronchitis: A Patient Guide
If you've been diagnosed with bronchiectasis, COPD, or other chronic lung problems, and keep getting infections or mucus that tests positive for Aspergillus, you might be told you have Aspergillus bronchitis. But what does that mean? And how is it different from ABPA (Allergic Bronchopulmonary Aspergillosis)?
This guide explains what Aspergillus bronchitis is, how it’s diagnosed, how common it is, and how it differs from ABPA.
🌬️ What Is Aspergillus Bronchitis?
Aspergillus bronchitis is a chronic fungal infection of the airways caused by Aspergillus fumigatus. It happens in people with damaged or scarred airways, such as:
-
Bronchiectasis
-
COPD
-
Cystic fibrosis
-
Occasionally asthma (if structural damage exists)
It’s a low-grade infection, not an allergy and not an invasive disease. The fungus lives in the mucus lining the airways, causing persistent inflammation, infection, and symptoms.
🔍 What Are the Symptoms?
| Common symptoms | What to know |
|---|---|
| Persistent cough | Often brings up sticky or brown mucus |
| Worsening breathlessness | Not always explained by asthma or infection alone |
| Fatigue or low energy | Common in chronic fungal infections |
| Frequent infections | May keep returning despite antibiotics |
| Wheeze | Sometimes, especially in asthma or ABPA overlap |
| Weight loss or low-grade fever | Possible in long-standing infection |
📊 How Common Is It?
Aspergillus bronchitis is underdiagnosed but increasingly recognised — especially in patients referred to specialist centres.
Estimated frequency in different conditions:
| Underlying condition | Estimated rate of Aspergillus bronchitis |
|---|---|
| Bronchiectasis | ~5–15%, higher in referral centres |
| COPD | ~1–5%, especially with steroid use |
| Cystic fibrosis | 5–10% (non-allergic cases) |
| Asthma (alone) | Rare unless bronchiectasis is also present |
It may be mistaken for a flare-up or chronic bacterial infection. Many people are told it’s “just colonisation” — but if symptoms persist and Aspergillus keeps growing in sputum, Aspergillus bronchitis should be considered.
🧪 How Is It Diagnosed?
There’s no single test. Diagnosis is based on clinical features plus evidence of fungal growth and a non-allergic immune pattern.
| Test | What it shows |
|---|---|
| Sputum culture / PCR | Repeated detection of Aspergillus |
| Aspergillus IgG (blood) | Often raised, shows chronic exposure |
| Aspergillus IgE & eosinophils | Usually normal — helps exclude ABPA |
| CT scan | Shows bronchiectasis, mucus plugging, but no cavitation |
| Response to antifungals | Clinical improvement supports diagnosis |
🔄 How Is It Different from ABPA?
ABPA is an allergic reaction to Aspergillus that mainly affects people with asthma or cystic fibrosis.
Aspergillus bronchitis, on the other hand, is a fungal infection in damaged airways, not an allergy.
| Feature | Aspergillus Bronchitis | ABPA |
|---|---|---|
| Type of disease | Chronic fungal infection | Allergic lung disease |
| Immune markers | High IgG, normal IgE | High IgE and eosinophils |
| Sputum | Repeated growth of Aspergillus | May or may not grow |
| CT findings | Bronchiectasis, mucus | Central bronchiectasis, mucus plugs |
| Treatment | Antifungals only | Steroids ± antifungals |
| Typical patient | Bronchiectasis, COPD | Asthma (often severe), sometimes CF |
Some patients can have both conditions at once, especially those with asthma and bronchiectasis — so testing is important.
💊 Treatment Options
| Treatment | Purpose |
|---|---|
| Oral antifungals (itraconazole, voriconazole) | Main treatment — often for several months |
| Inhaled antifungals (e.g. nebulised amphotericin) | Alternative if oral drugs not tolerated |
| Airway clearance physiotherapy | Helps remove mucus and fungal load |
| Regular sputum testing | To monitor treatment response |
| Steroids | Not used unless there’s overlapping ABPA or asthma |
🧠 Summary
| Question | Answer |
|---|---|
| Is it an infection? | ✅ Yes — fungal infection in the airways |
| Is it an allergy? | ❌ No — that’s ABPA |
| Can it coexist with ABPA? | ✅ Yes, in some cases |
| How is it diagnosed? | Repeated Aspergillus in sputum + high IgG + symptoms |
| How is it treated? | Antifungal medication (oral or nebulised) |
| Will it go away? | Often improves with treatment, but monitoring is essential |
💬 What to Ask Your Doctor
-
Could my symptoms be from Aspergillus bronchitis?
-
Have I had sputum cultures and Aspergillus blood tests (IgG, IgE)?
-
Would antifungal treatment help me?
-
Should I be referred to a specialist centre (e.g. for CPA, ABPA, bronchiectasis)?
-
Am I on the best airway clearance and physiotherapy plan?

🫁 The FeNO Test: What It Means for People with Aspergillosis
If you have aspergillosis, particularly ABPA (Allergic Bronchopulmonary Aspergillosis) or overlapping asthma, your doctor might suggest a test called FeNO. But what is it—and is it useful for people like you?
This guide explains the FeNO test in simple terms, how it works in patients with aspergillosis, and what to expect from the results.
🔍 What Is the FeNO Test?
FeNO stands for Fractional Exhaled Nitric Oxide. It’s a quick and painless breathing test that measures the level of nitric oxide gas in your breath.
Nitric oxide is naturally produced in your lungs. When your airways are inflamed—especially with eosinophilic (type 2) inflammation—levels go up.
This kind of inflammation is common in:
-
Asthma
-
Allergic Bronchopulmonary Aspergillosis (ABPA)
-
Some cases of chronic aspergillosis with allergic features
🎯 Why Might Aspergillosis Patients Be Offered a FeNO Test?
Your team might use FeNO to:
-
Support a diagnosis of ABPA or allergic asthma
-
Monitor inflammation levels over time
-
Check if inhaled steroids are working
-
Help plan changes to your treatment
FeNO can help show how much inflammation is active in your lungs, even if your symptoms haven’t changed much.
📈 Is the FeNO Test Accurate?
FeNO is a proven and recommended tool in asthma and allergic lung disease, including ABPA. But it works best when used alongside other information—such as:
-
Blood tests (like total and specific IgE)
-
CT scans
-
Lung function tests
-
Sputum cultures and fungal markers
So FeNO doesn’t give a “yes” or “no” answer by itself. It’s part of the bigger picture.
⚠️ What Can Affect the Results?
Certain things can raise or lower your FeNO level:
-
Smoking (lowers it)
-
Recent steroid use (lowers it)
-
Recent infections
-
Foods rich in nitrates (like beetroot, spinach)
-
ABPA flares (may raise it)
This is why your clinician will always interpret your FeNO result in context.
🩺 Should You Trust It?
Yes — when interpreted by an experienced team, FeNO is a safe and useful tool. It helps in understanding how allergic inflammation behaves in your lungs, especially if you're living with ABPA or asthma alongside aspergillosis.
✅ Summary for Aspergillosis Patients
-
FeNO is helpful in allergic forms of aspergillosis, like ABPA
-
It measures airway inflammation, especially type 2 (eosinophilic) inflammation
-
It helps guide treatment with inhaled steroids or biologics
-
It’s not a stand-alone test—it’s used together with other clinical information
-
If you’re unsure what your FeNO result means, just ask your care team
If you’re being treated at the National Aspergillosis Centre, or referred for specialist care, FeNO testing may be used to help plan or fine-tune your treatment.
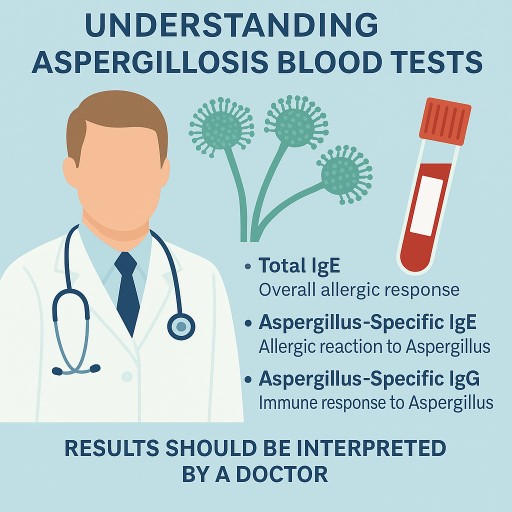
🧪 Understanding Aspergillosis Blood Tests: IgE and IgG Explained
For patients in the UK and internationally
If you are living with aspergillosis, including forms such as chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), or severe asthma with fungal sensitisation (SAFS), you may have had blood tests that measure how your immune system responds to Aspergillus, a common type of fungus.
This guide explains the role of these tests, why results may vary between hospitals, and what they mean for diagnosis and ongoing care.
🔬 What Are These Blood Tests?
✅ Total IgE
-
Measures your body’s overall allergic response.
-
Often raised in people with ABPA or SAFS, but also in asthma, eczema, and parasitic infections.
✅ Aspergillus-Specific IgE
-
Detects allergic reaction specifically to Aspergillus fumigatus.
-
Helps diagnose ABPA and SAFS.
✅ Aspergillus-Specific IgG
-
Measures immune response to longer-term exposure to Aspergillus.
-
Mainly used to help diagnose CPA, but can also support ABPA diagnosis.
📊 What Are the Normal Ranges?
📌 Total IgE Reference Ranges (UK Examples)
| Age Group | NHS Reference Range |
|---|---|
| Children | Varies by age, up to ~75 kU/L |
| Adults | 0–75 to 5–120 kU/L (depends on hospital) |
In ABPA, total IgE is usually > 500 kU/L, and sometimes exceeds 1000 kU/L.
📌 Aspergillus-Specific IgE: Positive Ranges
| Level (kUA/L) | What It Means |
|---|---|
| <0.35 | Negative |
| 0.35–0.7 | Borderline |
| 0.7–3.5 | Positive |
| >3.5 | Strongly positive |
| >17.5 | Very strongly positive |
📌 Aspergillus-Specific IgG: Positive Ranges
| Test Used | Positive Threshold |
|---|---|
| ImmunoCAP (most NHS labs) | >27–40 mgA/L |
| Bordier ELISA | >50–75 AU/mL |
| LDBio ICT (lateral flow strip) | Visual positive line |
The exact “positive” level depends on the test platform used by the lab. Always check which test was used when reviewing results.
🧪 Why Do Reference Ranges Differ Between Hospitals?
It’s common for different hospitals and countries to use slightly different tests and reference ranges. This is due to:
-
Different brands or types of test kits (e.g. ImmunoCAP, Bordier, Serion, LDBio)
-
Varying units of measurement
-
Locally validated ranges based on the population
-
Differences in clinical protocols or disease thresholds
For example, a test result of Aspergillus IgG at 38 mgA/L may be seen as positive in one hospital and borderline in another depending on which assay is used.
🧭 How These Tests Fit into Aspergillosis Diagnosis
🩺 Blood Tests Help Guide the Diagnosis, But Are Not Enough Alone
| Condition | Typical Test Findings |
|---|---|
| ABPA | Total IgE >500 kU/L + Aspergillus-specific IgE >0.35 kUA/L + often raised IgG |
| SAFS | Raised Aspergillus-specific IgE + asthma + poor steroid response |
| CPA | Aspergillus-specific IgG essential; total IgE and IgE may be normal |
Diagnosis always depends on a combination of factors — not just a blood test.
🧩 Other Essential Parts of Diagnosis
| Diagnostic Tool | What It Does |
|---|---|
| Chest CT scan | Detects cavities, nodules, or bronchiectasis |
| Sputum culture or PCR | Confirms presence of Aspergillus |
| Galactomannan or beta-D-glucan | Sometimes used to monitor invasive disease |
| Lung function tests | Assess asthma or airflow limitation |
| Symptoms | Breathlessness, cough, weight loss, fatigue |
| Treatment response | Helps confirm diagnosis if patient improves with treatment |
Blood tests are just one piece of the puzzle. Doctors always interpret them alongside imaging, symptoms, and history.
🩺 What About Management?
Once diagnosed, managing aspergillosis involves more than just monitoring blood tests. Your care plan may include:
-
Antifungal medication (e.g. itraconazole, voriconazole)
-
Steroids or biologics (especially in ABPA)
-
Physiotherapy to clear mucus
-
Regular imaging (e.g. CT scans)
-
Monitoring IgE/IgG over time
-
Patient support for fatigue, emotional health, and quality of life
📋 Understanding Your Results: What Do They Mean?
When you receive blood test results like total IgE, Aspergillus-specific IgE, or Aspergillus-specific IgG, you may see a number alongside a reference range (sometimes called the “normal range”). This helps show whether your result is considered low, normal, or high in that specific laboratory.
🧾 Example:
| Test | Your Result | Lab Reference Range | Interpretation |
|---|---|---|---|
| Total IgE | 580 kU/L | 0–120 kU/L | Elevated |
| Aspergillus-specific IgE | 0.9 kUA/L | >0.35 = positive | Positive |
| Aspergillus-specific IgG | 39 mgA/L | 0–27 mgA/L | Borderline high |
❓ Is a Slightly High Result a Problem?
-
A mild or borderline elevation does not automatically mean disease.
-
Some people may have a raised IgE or IgG but no active symptoms or signs of aspergillosis.
-
Other people with clear disease may have only modest rises in their test levels.
🔍 Important: Test results must always be interpreted in the context of your overall health, scan results, and symptoms.
✅ Let Your Doctor Guide You
It’s completely normal to feel uncertain or anxious about test results — especially if a number is just above the “normal range.” But:
-
Let your doctor or specialist interpret the result as part of your whole clinical picture.
-
They may repeat the test, combine it with a CT scan or lung function test, or monitor changes over time.
-
Some test levels, like total IgE in ABPA, are tracked over months to see if treatment is working.
💬 Ask your doctor:
“How does this result fit in with my symptoms and scan findings?”
🧠 Final Takeaway
Blood tests like IgE and IgG are essential tools in diagnosing and managing aspergillosis, but they are only one part of the bigger picture. Imaging, symptoms, response to treatment, and even how you feel day-to-day are just as important.
Always ask for a copy of your results with reference ranges, and bring them to appointments.
And remember — a slightly raised result doesn’t always mean something is wrong. Your doctor is the best person to interpret it for you.
Patient Guide: Understanding Aspergillus-Related Chronic Pulmonary Disease
Based on new international guidance (2024)
What is Aspergillus and Why Is It Important?
Aspergillus is a common type of fungus found in the environment. Most people breathe it in every day without any problem. However, if you have a lung condition or a weakened immune system, Aspergillus can cause serious problems. It can:
- Trigger allergic reactions in the lungs
- Infect damaged lung tissue
- Worsen symptoms like coughing, wheezing, or breathlessness
Until recently, doctors treated each type of aspergillus-related lung disease as a separate condition. But new guidance recognises that many patients may have more than one form or sit on a spectrum.
What Conditions Are Included?
The term "aspergillus-related chronic pulmonary disease" covers a range of conditions:
| Condition | What it means |
|---|---|
| ABPA (Allergic Bronchopulmonary Aspergillosis) | An allergic reaction to Aspergillus, usually in asthma or cystic fibrosis patients |
| CPA (Chronic Pulmonary Aspergillosis) | A slow-developing fungal infection, often in people with pre-existing lung damage |
| Aspergillus bronchitis | A fungal infection in the airways, often in people with bronchiectasis |
| Overlap syndromes | Some people show features of more than one of the above |
What Are the Symptoms?
Symptoms can vary, but common signs include:
- Persistent cough (sometimes with mucus or blood)
- Wheezing or breathlessness
- Fatigue and low energy
- Weight loss or loss of appetite
- Repeated chest infections
If you experience these symptoms and have an underlying lung condition, it’s important to ask whether Aspergillus might be involved.
How Is It Diagnosed?
Doctors now use a combination of tests to get a clearer picture:
- Chest CT scan – to look for signs of lung damage or fungal balls
- Sputum samples – to check for the presence of Aspergillus
- Blood tests – to detect allergic antibodies (IgE), immune responses (IgG), or fungal antigens
- Bronchoscopy (sometimes) – to collect samples directly from the lungs
These tests help doctors decide whether it’s an allergic reaction, an infection, or both.
How Is It Treated?
Treatment depends on your symptoms and test results. The aim is to:
- Reduce inflammation
- Clear fungal infection
- Prevent further lung damage
Common treatment options include:
| Treatment | Purpose |
| Steroids (e.g. prednisolone) | Reduce allergic inflammation (especially in ABPA) |
| Antifungal drugs (e.g. itraconazole, voriconazole) | Treat fungal infection and reduce fungal burden |
| Biologic therapies (e.g. omalizumab, dupilumab) | Used in difficult-to-treat allergic cases |
| Nebulised antibiotics | If other infections (like Pseudomonas) are also present |
| Surgery (rarely) | To remove fungal balls or damaged tissue in severe CPA |
What Has Changed in the 2024 Guidance?
- Doctors are now encouraged to look for overlapping features, not just one diagnosis.
- More emphasis is placed on early detection and preventing lung decline.
- Guidelines promote the use of multidisciplinary teams (MDTs) for complex cases.
- Newer treatments, including biologics, are being recommended more often.
- Patients with symptoms but unclear diagnoses should be re-evaluated regularly.
What Can You Do as a Patient?
- Know your diagnosis – Ask your team whether your current label still fits your symptoms
- Track your symptoms – Keep a log of cough, breathlessness, fatigue, and infections
- Ask about specialist referral – For example, to a National Aspergillosis Centre
- Stay informed – Visit aspergillosis.org for up-to-date guidance
- Take medications as prescribed and report any side effects promptly
Support and Information
- Patient support groups can help you connect with others
- Pulmonary rehabilitation and breathing therapy can improve quality of life
- Annual reviews and regular scans can help spot problems early
For more information, leaflets, and help getting the right care, visit: aspergillosis.org
You don’t have to manage this alone.

🫁 Understanding ABPA: When and Why It Appears, and Who’s at Risk
Allergic Bronchopulmonary Aspergillosis (ABPA) is a chronic allergic lung condition that’s often misunderstood or misdiagnosed — especially when it appears for the first time in adulthood. This article answers key questions:
-
Why does ABPA usually develop later in life?
-
Can it be diagnosed earlier?
-
What about severe asthma in children — is that an exception?
-
Are there groups at special risk, like those with cystic fibrosis?
This guide is designed for patients, carers, and anyone living with or at risk of ABPA.
🔹 1. What Is ABPA?
ABPA is a hypersensitivity reaction (not a fungal infection) to the fungus Aspergillus fumigatus, which is found in the air we breathe.
In people with asthma, cystic fibrosis (CF), or structurally damaged lungs, Aspergillus can settle in the airways and trigger a strong allergic immune response, causing:
-
Swollen and inflamed airways
-
Mucus build-up that’s hard to clear
-
Worsening of asthma or coughing
-
Irreversible lung damage (e.g. bronchiectasis) if untreated
🔎 2. Why Is ABPA Usually Diagnosed in Adulthood?
Despite being linked to asthma — often a childhood condition — most cases of ABPA are diagnosed in adulthood, typically between ages 20 and 50.
Why? Because ABPA is only diagnosed when several things happen at the same time:
-
High total IgE levels
-
Positive Aspergillus-specific IgE or IgG
-
Lung symptoms like wheezing, cough, mucus
-
CT evidence of mucus plugging or early bronchiectasis
A person might be allergic to Aspergillus (sensitised) for years without having ABPA. Only when their immune system crosses a certain threshold — sometimes after a viral illness, fungal exposure, or change in immune function — does full ABPA emerge.
This helps explain why many people are diagnosed for the first time in their 30s or later, even with a history of asthma.
🧒 3. Is ABPA Ever Diagnosed in Childhood?
✅ Yes — but it’s rare.
There are a few specific exceptions:
🔸 A. Cystic Fibrosis (CF)
-
ABPA is much more common in people with CF — including older children and teenagers.
-
CF causes thick mucus and impaired airway clearance, which promotes persistent exposure to Aspergillus.
-
That’s why CF care guidelines include annual ABPA screening from a young age.
🔸 B. Severe asthma in childhood
-
Children with very severe or poorly controlled asthma may have:
-
High IgE
-
Mucus build-up
-
Sensitisation to Aspergillus
-
-
These children may develop fungal allergic airway disease or be labelled as having SAFS (Severe Asthma with Fungal Sensitisation).
-
Full ABPA may still not be diagnosed until later adolescence or adulthood — but these cases may represent a kind of “pre-ABPA.”
🔸 C. Rare immune disorders
-
Conditions like hyper-IgE syndrome (HIES) or chronic granulomatous disease may cause early ABPA-like features.
-
These are rare and usually managed by immunology specialists.
⚖️ 4. What’s the Difference Between ABPA, SAFS, and Sensitisation?
| Condition | Description | Age group |
|---|---|---|
| Aspergillus sensitisation | Immune system reacts to fungus, but no lung damage or ABPA symptoms | Any age |
| SAFS | Severe asthma + Aspergillus allergy, but does not meet full ABPA criteria | Mostly teens and adults |
| ABPA | Allergy to Aspergillus + lung damage, high IgE, mucus, flare-ups | Usually adults, sometimes teens with CF |
🧪 5. Could a Screening Test Detect ABPA Earlier?
Not currently — but research is ongoing.
Today, ABPA is diagnosed based on a set of criteria (IgE levels, imaging, symptoms), not a single test. That means:
-
Early warning signs may be present for years
-
But ABPA is only diagnosed once enough features appear together
A future screening test for “pre-ABPA” could:
-
Identify at-risk individuals earlier
-
Allow close monitoring
-
Help start treatment at the first signs of disease
This wouldn’t “prevent” ABPA in every case, but could reduce its severity and protect lung function.
💡 6. Can ABPA Be Prevented?
We can’t fully prevent ABPA — but we can reduce risk and prevent long-term damage:
| Strategy | What It Helps Prevent |
|---|---|
| Reduce fungal exposure (damp, compost, hay) | Immune flare-ups, new sensitisation |
| Monitor at-risk patients (CF, severe asthma) | Missed early signs |
| Treat asthma or CF aggressively | Mucus build-up and fungal colonisation |
| Investigate persistent cough/mucus or asthma flares | Delayed ABPA diagnosis |
| Use steroids/antifungals/biologics when needed | Inflammation, progression to bronchiectasis |
📘 7. Summary: Key Takeaways
| Question | Answer |
|---|---|
| Is ABPA a childhood disease? | No, it’s usually diagnosed in adults, even those with childhood asthma |
| Can it appear in children? | Rarely — mostly in CF, severe asthma, or immune disorders |
| Why isn’t it diagnosed earlier? | It requires multiple features to appear at the same time |
| Can it be stopped before it starts? | Possibly in future — early monitoring could reduce damage, even if it doesn’t prevent ABPA |
| What should I do? | Avoid triggers, manage asthma/CF well, seek early specialist input for unexplained symptoms |
🗣️ Patient Tip
“If you’ve just been diagnosed in your 30s, 40s or later — that doesn’t mean it was missed. It means it’s finally been recognised, and now you can get the right treatment.”