Published: July 2026
Medical research into aspergillosis continues to advance rapidly, with new studies appearing almost every week. Some confirm what doctors already suspected, while others introduce new ideas about how the body fights fungal infections or how treatment might improve in the future.
This week’s research includes a major international review of invasive aspergillosis in intensive care, encouraging real-world results for the antifungal drug isavuconazole, and two laboratory studies suggesting that specialised immune cells called macrophages may play an even greater role in protecting the lungs than previously appreciated.
None of these studies changes current treatment recommendations immediately. Together, however, they highlight an important direction in aspergillosis research: understanding not only how to kill the fungus, but also how to strengthen the body’s own immune defences.
A major international review confirms the burden of invasive aspergillosis in intensive care
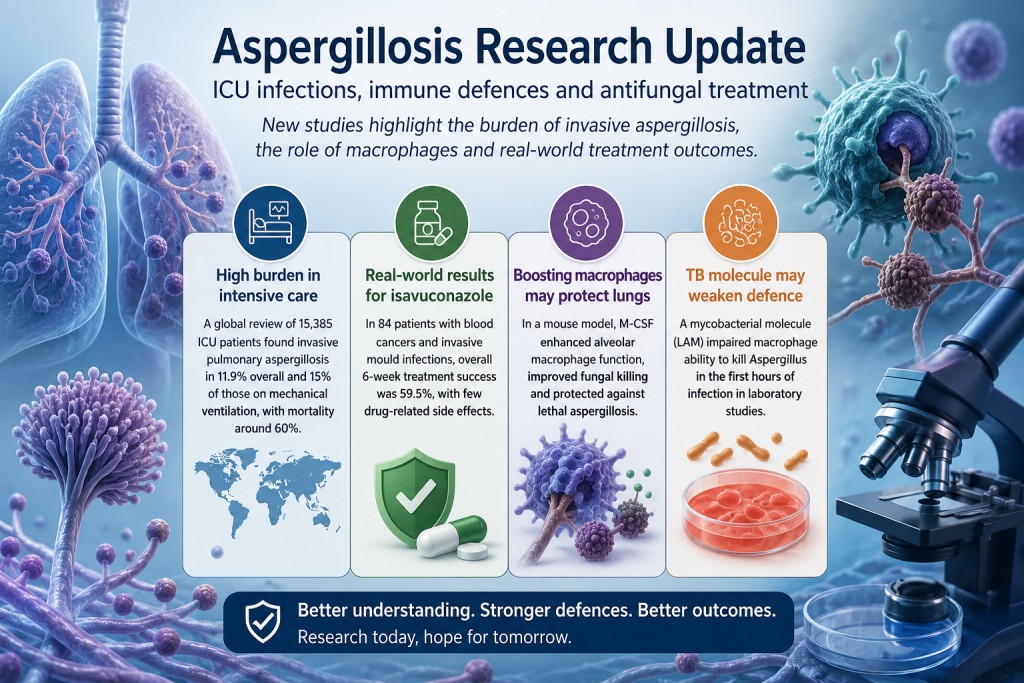
A systematic review and meta-analysis combined results from 56 observational studies involving 15,385 intensive care patients. Among these patients, 2,381 cases of invasive pulmonary aspergillosis, or IPA, were identified.
The researchers estimated that IPA occurred in approximately 11.9% of the critically ill patients included in the studies. The estimated incidence increased to 15% among patients receiving mechanical ventilation.
Mortality among patients diagnosed with IPA was high:
- 59.6% overall mortality
- 61.9% mortality among mechanically ventilated patients
Factors associated with an increased risk of developing IPA included:
- immunosuppression;
- blood cancers and other malignancies;
- corticosteroid use before admission to intensive care;
- chronic lung, kidney, liver or heart disease;
- mechanical ventilation;
- vasopressor treatment;
- and renal replacement therapy.
What does this mean?
This study reinforces that invasive aspergillosis remains a serious complication in selected critically ill patients.
However, the results should not be interpreted as meaning that approximately one in eight people admitted to intensive care will develop aspergillosis. The authors state that the evidence predominantly reflects COVID-19-associated pulmonary aspergillosis, commonly known as CAPA.
Many of the identified risk factors, such as mechanical ventilation, vasopressor treatment and renal replacement therapy, are also signs that a patient is already extremely unwell. The study therefore identifies associations but cannot prove that these treatments independently cause aspergillosis.
The authors conclude that targeted screening and tailored antifungal strategies in high-risk patients deserve prospective evaluation. They do not claim that universal screening or preventive antifungal treatment has already been shown to improve survival.
Read the paper record on PubMed
Real-world evidence continues to support isavuconazole
Another study examined how well isavuconazole performs in routine clinical practice among people with blood cancers who develop serious invasive mould infections.
The retrospective study included 84 adults treated at two hospitals in China between 2022 and 2025:
- 62 had invasive aspergillosis;
- 14 had mucormycosis;
- 8 had mixed mould infections.
The main measure of success was assessed after six weeks. To count as successful treatment, the patient had to survive, show clinical or radiological improvement and avoid stopping treatment because of failure or toxicity.
The overall six-week treatment success rate was 59.5%. Among patients with aspergillosis, treatment success was higher, at 69.4%.
Only four patients experienced recorded drug-related adverse effects, and one stopped treatment because of vomiting.
What does this mean?
These findings are reassuring because they reflect routine clinical practice rather than the more controlled circumstances of a clinical trial.
The study found that patients receiving isavuconazole alone appeared to have better outcomes than those receiving combination antifungal treatment. However, this result must be interpreted cautiously.
Doctors commonly reserve combination therapy for patients who are more severely ill, have failed previous treatment, have mixed infections or are suspected of having resistant disease. The poorer outcomes in the combination-treatment group may therefore reflect the severity of the patients’ infections rather than harm caused by combining antifungal medicines.
This is known as confounding by indication. Because the patients were not randomly assigned to treatment, the study cannot establish that monotherapy is superior to combination treatment.
Overall, the study adds confidence that isavuconazole can be an effective and generally well-tolerated treatment for invasive aspergillosis in patients with haematological malignancies. It does not show that isavuconazole is better than other antifungal medicines, and it does not apply directly to chronic pulmonary aspergillosis, ABPA or Aspergillus bronchitis.
Read the paper record on PubMed
Could strengthening lung macrophages help prevent invasive aspergillosis?
Perhaps the most scientifically intriguing study this week did not test a new antifungal drug.
Instead, researchers investigated whether they could improve the ability of the lung’s own immune cells to eliminate Aspergillus fumigatus before infection became established.
The study focused on alveolar macrophages. These specialised immune cells live inside the air sacs of the lungs and are among the first cells to encounter inhaled Aspergillus spores.
Using a stem-cell transplant mouse model and an unusually low dose of Aspergillus spores intended to resemble everyday exposure, the researchers found that alveolar macrophages played a crucial role in protecting against invasive aspergillosis during the earliest stages of infection.
The researchers then tested whether macrophage function could be improved using macrophage colony-stimulating factor, or M-CSF.
M-CSF treatment:
- improved macrophage migration;
- enhanced phagolysosomal function;
- increased fungal killing;
- preserved lung tissue;
- reduced inflammatory cytokines;
- and protected mice against lethal invasive aspergillosis.
The researchers also tested primary human alveolar macrophages and found that M-CSF improved several of the same antifungal functions.
Importantly, the protective effect disappeared when alveolar macrophages were removed. This provides strong experimental evidence that the macrophages themselves were responsible for much of the benefit.
What does this mean?
This research suggests that tissue-resident macrophages may play an especially important role during the first hours after Aspergillus spores reach the lungs.
It also supports the wider idea of host-directed therapy: treatments designed to strengthen the patient’s immune response rather than attacking the fungus directly.
However, this study was carried out mainly in mice and has been published as a preprint. It has not yet completed formal peer review.
M-CSF is therefore not an established treatment for aspergillosis. Researchers would need to establish appropriate dosing, safety and effectiveness in people, particularly because stimulating immune activity after stem-cell transplantation could potentially affect inflammation, graft-versus-host disease and other immune processes.
Tuberculosis may affect immune defences as well as damaging the lungs
People who have previously had pulmonary tuberculosis are at increased risk of developing chronic pulmonary aspergillosis, or CPA.
The usual explanation is structural lung damage. Tuberculosis may leave behind cavities, scarring, bronchiectasis and damaged airways, creating an environment in which Aspergillus can persist.
A new laboratory study suggests that there may also be an immunological component.
The researchers studied a mycobacterial cell-wall molecule called lipoarabinomannan, or LAM. This molecule is known to interfere with some of the cellular pathways used by macrophages to respond to infection.
Bone-marrow-derived macrophages were exposed to two forms of LAM and then challenged with swollen Aspergillus fumigatus conidia.
Exposure to LAM:
- increased macrophage death;
- increased inflammatory cytokine release, particularly IL-1β;
- and reduced the ability of macrophages to kill Aspergillus conidia during the first six hours of infection.
The reduction in fungal killing was demonstrated using both colony-counting methods and time-lapse fluorescence microscopy.
What does this mean?
This study provides a plausible biological mechanism through which mycobacterial infection might interfere with early antifungal immune responses.
It does not, however, prove that this mechanism causes CPA after tuberculosis.
The experiments were conducted in laboratory-grown macrophages. They do not show that LAM remains present in the lungs for months or years after tuberculosis, nor that macrophages from people with previous tuberculosis behave in the same way.
The findings therefore do not replace the established structural explanation linking tuberculosis and CPA. Instead, they raise the possibility that lung damage and altered local immunity may work together.
Read the paper record on PubMed
A common theme emerges: macrophages matter
Although these studies examined different questions, two independent research groups reached complementary conclusions.
One study found that strengthening macrophage activity improved fungal killing and survival. The other found that disrupting macrophage activity reduced fungal killing.
Together, they support an emerging view that alveolar macrophages may be central to determining whether inhaled Aspergillus spores are cleared rapidly or allowed to develop into disease.
This does not reduce the importance of neutrophils, antifungal medicines or structural lung damage. Instead, it adds a more detailed understanding of what may happen during the earliest stages of fungal exposure.
Future advances in aspergillosis treatment may therefore involve both:
- better drugs that attack Aspergillus directly;
- and treatments that help the immune system respond more effectively.
What does this mean for people living with aspergillosis?
For most patients currently receiving treatment, these studies do not change day-to-day management.
Antifungal medicines remain the foundation of treatment for invasive and chronic Aspergillus infection. Patients should continue following the advice of their respiratory, infectious-diseases or specialist aspergillosis team.
These studies nevertheless provide encouraging evidence that aspergillosis research is progressing across several fronts:
- improving recognition of invasive aspergillosis in intensive care;
- evaluating how existing antifungal treatments perform in routine practice;
- understanding why some people are more vulnerable to Aspergillus than others;
- and exploring whether the immune system itself could become a future treatment target.
Progress is often gradual, and laboratory findings do not always lead to successful treatments. However, each study adds another piece to the puzzle and helps researchers move towards more effective and more personalised approaches to aspergillosis.
References
- Zhou Z, Luo B, Zhang X, et al. Incidence, mortality and risk factors of invasive pulmonary aspergillosis in critically ill patients during the COVID-19 era: a global systematic review and meta-analysis. Annals of Clinical Microbiology and Antimicrobials. Published 10 July 2026. PubMed. DOI.
- Zhang J, Xu M, Mao J, et al. Isavuconazole for invasive mold disease in patients with hematological malignancies: a multicenter real-world study from China on efficacy, safety, and competing risks. Antimicrobial Agents and Chemotherapy. Published 6 July 2026. PubMed. DOI.
- Sheta D, Mokhtari Z, Strobel M, et al. M-CSF-stimulated alveolar macrophages safeguard from invasive aspergillosis. bioRxiv. Preprint published 9 July 2026. DOI and preprint.
- Gonzales-Huerta LE, Williams TJ, Aljohani R, et al. Mycobacterial lipoarabinomannan negatively interferes with macrophage responses to Aspergillus fumigatus in vitro. PLOS ONE. 2026;21(7):e0351935. PubMed. DOI.
This article summarises newly published research for patients and non-specialist readers. It does not replace individual medical advice from a qualified healthcare professional.