Browse information
Latest Articles
Support
For Professionals
Search
Weekly Updates
Home
Archive by Category "Weekly Updates"
Weekly Updates
Aspergillosis Weekly Research Update
by GAtherton
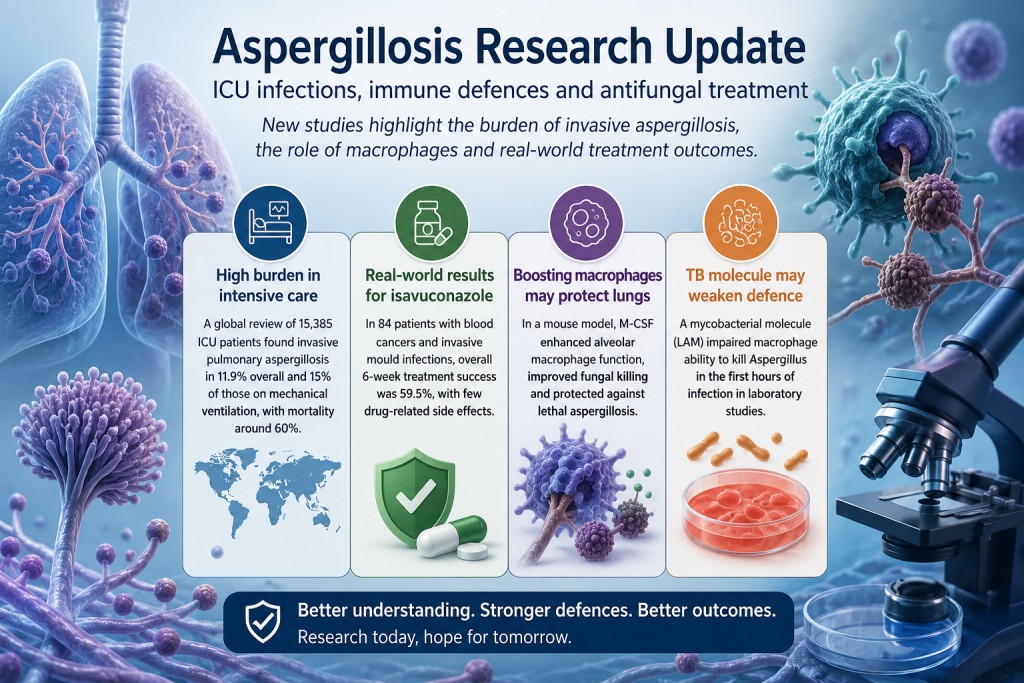
Aspergillosis Research Update: ICU Infections, Immune Defences and Antifungal Treatment
by GAtherton
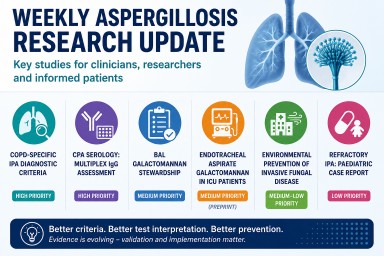
Weekly Aspergillosis Research Update: COPD IPA Criteria, CPA Serology, ICU Galactomannan and Environmental Prevention
by GAtherton
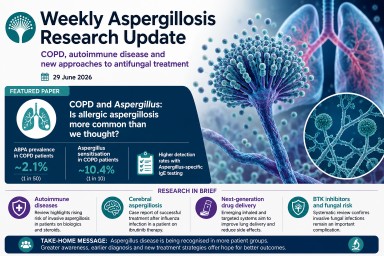
Weekly Aspergillosis Research Update: June 29
by GAtherton
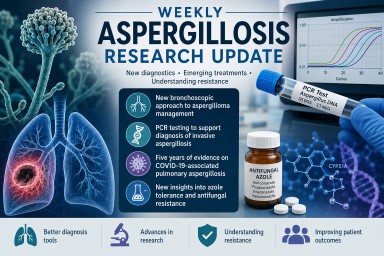
Weekly Aspergillosis Research Update: New Diagnostics, CAPA Evidence, and Why Azole Tolerance Matters
by GAtherton
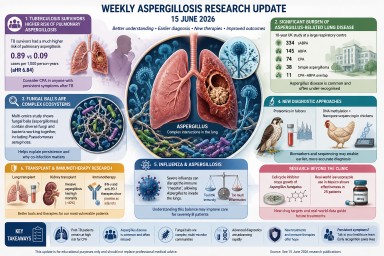
Weekly Aspergillosis Research Update – 15 June 2026
by GAtherton
Professional Aspergillosis Update: May 2026
Audience: respiratory…
by GAtherton
Aspergillosis Research Update: Week Ending 8 June 2026
Key Points This was a…
by GAtherton
Aspergillosis Research Update: Earlier Diagnosis, Better Testing and New Treatment Possibilities
by GAtherton
Weekly Aspergillosis Research Update 18th May 2026
In this week’s aspergillosis…
by GAtherton
1
2
3
…
5