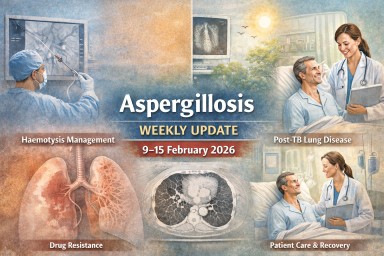
Weekly Updates
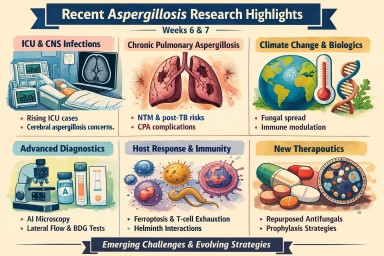
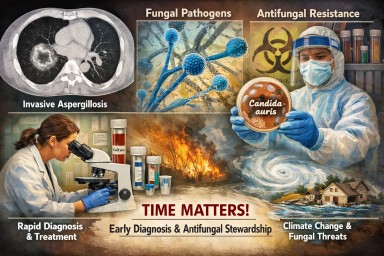
Systemic fungal infections: why speed, diagnosis and stewardship matter
Systemic fungal infections —…

Connecting patients, carers, clinicians and scientists to improve life with aspergillosis
World Aspergillosis Day (WAD)…

Systemic fungal infections —…
World Aspergillosis Day (WAD)…