
Understanding Mucous Casts in Allergic Bronchopulmonary Aspergillosis (ABPA)
People living with Allergic Bronchopulmonary Aspergillosis (ABPA) often notice thick, unusual mucus coming up during a flare. Some of this mucus can look very different from “normal” sputum and may be described as mucous casts. This leaflet explains what they are, why they happen, and what they mean for your ABPA.
⭐ What are mucous casts?
A mucous cast is a thick, sticky plug of mucus that forms inside your airways.
It takes on the exact shape of the airway or branch it was sitting in – a bit like a soft mould of the inside of your lungs.
When coughed up, casts may look:
-
long and tube-shaped
-
soft and rubbery
-
curled or C-shaped
-
occasionally branching, like a twig
-
pale yellow/cream with darker specks
These darker flecks can include dead inflammatory cells, airway debris, and sometimes tiny amounts of fungal material trapped inside.
⭐ Why do they happen in ABPA?
ABPA is not an infection, but an allergic over-reaction to the Aspergillus fungus.
This allergic inflammation causes:
1. Excess mucus production
Your airways create far more mucus than usual.
2. Thicker, stickier mucus
Inflammation changes the chemistry of the mucus, making it harder to clear.
3. Swollen, narrowed airways
This makes it easy for mucus to get stuck and form plugs.
4. Trapped material
Casts can contain:
-
fungal spores
-
inflammatory cells
-
dust or other inhaled particles
-
old blood or tissue debris
All of this can glue together into a cast.
⭐ Are mucous casts harmful?
They are not dangerous on their own, but they can cause problems:
-
Airway blockage → breathlessness, wheeze, sudden tightness
-
Chest infections → trapped mucus is an ideal place for bacteria
-
ABPA flare-ups → casts often appear during periods of high inflammation
-
Reduced airflow on CT scans → seen as “bronchial impaction”
Telling your clinical team when you notice casts helps them judge how active your ABPA is.
⭐ What do mucous casts look like in ABPA?
Patients often describe:
-
“noodles”
-
“worms”
-
“rubbery plugs”
-
“little branches”
-
“specks of brown/black” within pale mucus
These appearances are normal in ABPA and do not mean your lungs are permanently worsening.
⭐ How are mucous casts managed?
1. Airway clearance
This is the most important step. Techniques include:
-
huff-coughing
-
active cycle of breathing
-
nebulised saline (hypertonic or isotonic)
-
flutter/PEP devices (Acapella, Aerobika)
-
chest physiotherapy
These help loosen and move mucus from deeper airways.
2. Medication
Depending on your treatment plan:
-
inhalers (bronchodilator + inhaled steroids)
-
biologics (e.g., mepolizumab, dupilumab, omalizumab)
-
antifungal medication if prescribed as part of your ABPA care
-
oral steroids if medically appropriate
Biologics can reduce the inflammation that causes casts, so many patients notice fewer plugs over time.
3. Monitoring
Your team may keep an eye on:
-
sputum samples
-
IgE levels
-
CT scan changes
-
symptom patterns
⭐ When should I tell my team?
Contact your clinical team if you notice:
-
more frequent mucous casts
-
sudden breathlessness or chest tightness
-
a drop in your usual oxygen saturation
-
fever or signs of infection
-
coughing up blood
-
a change in colour or smell of mucus
⭐ Reassurance
Mucous casts are very common in ABPA.
They can look alarming, but they are simply a sign that your airways are inflamed and producing thick mucus.
Coughing them out is helpful, not harmful.
It allows the affected airway to reopen and can rapidly improve breathing.
✅ Further Reading
For more patient-oriented information, you can visit the AFIT website where the term “casts” is discussed in the context of aspergillosis: Aspergillus.org.uk – search “casts”.

⭐ How to Avoid Being Fooled by Misleading Products, Private Tests and Health Claims
A practical, evidence-based guide for people living with aspergillosis, asthma, bronchiectasis and COPD
People with long-term lung conditions are often targeted by persuasive marketing, “health influencers”, alternative practitioners, and private test companies.
These services frequently exploit fear, frustration, and the very understandable desire for answers.
This expanded guide explains why certain products look scientific, why most are biologically impossible, and how you can protect yourself from being misled or spending money on things that cannot help your condition.
This is about empowerment — never about blaming patients.
🧩 1. Why misleading products look convincing
Companies deliberately use wording and imagery that trigger trust:
-
lab coats
-
microscopes
-
graphs and biological diagrams
-
words like “antifungal”, “immune”, “toxins”, “wellness”, “clinical strength”
These features make a product appear evidence-based — but appearance is not evidence.
Many claims contain a grain of truth, e.g.:
-
“Tea tree oil kills fungus in the lab”
-
“Silver has antimicrobial properties”
-
“This herbal extract reduces inflammation in laboratory tests”
But the missing information is the critical part:
⭐ The lab conditions have nothing to do with the human body.
To “kill fungus in a dish”, companies use concentrations that:
-
would be toxic in humans
-
cannot reach the lung tissue
-
would be broken down in the gut or bloodstream
-
do not survive into the airways
Companies rely on the fact that most customers don’t know this.
🧬 2. “Plausibility comes before testing” — the rule companies hope you don’t know
Scientists follow a simple chain:
1️⃣ Is it plausible?
Can the substance reach the lung?
Does the pathway make sense?
2️⃣ If yes — test it.
If not — don’t.
Products sold online almost always fail at Step 1.
Examples:
Turmeric supplements
Even at huge oral doses, only a tiny amount enters the bloodstream — nowhere near the lung in meaningful levels.
Oregano oil
Kills fungi on metal plates in labs — but the amount needed inside the lung would be toxic.
Silver products
Irritate the lungs and accumulate in tissues — highly implausible as therapy.
Essential oils
Break down long before reaching the airways in meaningful amounts.
Herbal antifungals
Often metabolised by the gut and liver — never reach airways at therapeutic levels.
This is why clinical trials don’t happen —
not because no one has tried,
but because there’s no scientific reason to bother.
🛍️ 3. How companies use “allowed” claims to sound medical
Because these products are not classed as medicines, they must not claim to “treat disease”.
So companies use vague, legally safe wording:
-
“Supports immunity”
-
“Maintains wellness”
-
“Promotes respiratory health”
-
“Contains antifungal botanicals”
-
“Helps with mould exposure”
-
“Advanced detox science”
All of these sound medical but say nothing measurable.
Example:
A supplement cannot say:
-
“Improves aspergillosis symptoms”
But it can say:
-
“Supports healthy immune response”
This tricks the viewer into mentally connecting the dots without the company making any illegal claims.
🧊 4. Air filters — the rare partial exception
Air purifiers can help some people, because they reduce:
-
dust
-
pollen
-
irritants
-
pet dander
-
airborne particulate matter
These changes may ease coughing or wheezing in sensitive people.
BUT…
most devices sold online are far too weak.
A purifier needs:
-
True HEPA H13 filter (not “HEPA-type”)
-
CADR 250–350+ for most rooms
-
Strong fan to turn over room air 4–5 times per hour
Without these, a purifier is just an expensive fan.
What they cannot do:
-
cure aspergillosis
-
remove Aspergillus from the lungs
-
prevent exposure
-
substitute for ventilation
-
fix damp or mould in walls
They improve comfort, not disease.
👩⚕️ 5. Why alternative practitioners are so persuasive
Alternative practitioners often:
-
speak with confidence
-
promise personalised care
-
provide long consultations
-
listen sympathetically
-
use scientific-sounding language
-
offer simple explanations for complex symptoms
Their tests and treatments look legitimate, but the problems include:
❌ No training in lung disease
❌ Misunderstanding of immunology
❌ Misuse of lab dish studies
❌ Incorrect interpretation of “toxins”
❌ Selling supplements with no evidence
❌ Recommending dangerous inhaled substances (e.g., oils, peroxide)
❌ Relying on anecdotes, not data
Even well-meaning practitioners can unintentionally cause:
-
lung irritation
-
drug interactions
-
adrenal effects
-
delays in proper NHS treatment
-
unnecessary fear
🧪 6. Private test companies — why their results look real but mean nothing
Common private tests include:
-
mycotoxin urine tests
-
“mould illness panels”
-
detox pathway testing
-
food IgG tests
-
fungal metabolite tests
-
heavy metal hair analysis
-
“immune balance” panels
-
testosterone finger-prick kits
These results are presented with:
-
charts
-
colour-coded ranges
-
expert-sounding commentary
But the key issue is:
⭐ The reference ranges are invented by the company.
Often “high” simply means:
-
“higher than the average of people who bought this test”
Not:
-
higher than healthy people
-
higher than unwell people
-
linked to disease
GPs and consultants cannot act on these results because they are not medically interpretable.
👨⚕️ 7. Testosterone tests — a perfect illustration of misleading health screening
Companies advertise:
-
“Tired? Low mood? Low motivation?”
-
“Check your testosterone at home”
-
“Feel younger again”
They use US-style messaging that implies easy treatment.
But in the UK, testosterone treatment requires:
-
symptoms consistent with hypogonadism
-
two morning venous blood tests
-
validated hospital labs
-
endocrine specialist interpretation
-
ruling out multiple other causes
- testosterone levels fall slowly as part of ageing - it is normal
Finger-prick tests do not meet NHS criteria,
so patients end up:
-
anxious
-
misinformed
-
sold supplements
-
not eligible for NHS treatment
This perfectly mirrors the broader pattern of private testing.
🔍 8. The “curiosity gap”: why people buy tests that GPs won’t order
Patients understandably feel:
-
frustrated
-
curious
-
confused
-
not listened to
-
desperate for answers
When a GP says “That test won’t help,” it can feel like:
-
rejection
-
dismissal
-
obstruction
But the reality is:
⭐ GPs are following evidence-based pathways to protect you.
Most private tests:
-
do not answer a clinical question
-
have false positives
-
trigger unnecessary follow-up scans
-
cause anxiety
-
cannot be interpreted
-
do not influence treatment
Private companies exploit:
-
curiosity
-
frustration
-
the desire for answers
-
the emotional gap left by long waits or unexplained symptoms
But a meaningless test result is worse than no test at all.
🧾 9. Real-world examples: 15 common traps to avoid
1. Mould settle plates
All rooms grow mould on plates — totally meaningless for health.
2. IgG food sensitivity tests
Measure normal immune exposure, not allergies.
3. Finger-prick vitamin tests
Often inaccurate and label normal levels as “borderline”.
4. Lung detox drinks
Nothing you drink detoxes the lungs.
5. Hydrogen peroxide / silver nebulisers
Dangerous. Irritate lungs. Risk chemical burns and pneumonitis.
6. Essential oil diffusers marketed as “antifungal”
Irritate airways; no delivery to lung tissue.
7. Mycotoxin detox programmes
Based on non-diagnoses; push expensive supplements.
8. Immune-boosting products
No supplement boosts immunity in a useful way for aspergillosis.
9. “Black mould blood tests”
No such test exists; ranges are invented.
10. Ozone machines and air ionisers
Harmful to lungs; zero evidence.
11. Anti-mould paint additives
Mask damp; do not impact indoor fungal counts long term.
12. Red-light therapy devices
Cannot penetrate tissue; no lung benefit.
13. Detox foot patches
Turn brown from sweat; total scam.
14. Anti-mould laundry boosters
Irrelevant to aspergillus exposure.
15. Humidifiers sold for “lung support”
Raise humidity → increase mould risk.
🛡️ 10. The Anti-Fooling Checklist
Before you buy anything, ask:
✔ Has this been tested in people with aspergillosis?
✔ Can it physically reach the lungs?
✔ Does NHS medicine recognise or use it?
✔ Are the claims vague? (“supports immunity”)
✔ Are the reference ranges medically valid?
✔ Would my consultant recommend this?
✔ Is this a simple answer to a complex condition?
If any answer is no, it’s a red flag.
⭐ 11. Golden rule
If a treatment or test genuinely helped aspergillosis, your consultant would already be using it —
not influencers, Amazon sellers, or unregulated US labs.
🌟 12. Final message: It’s not foolishness — it’s human
You are not being “tricked” because you’re naïve.
These products are engineered to be emotionally irresistible.
People with chronic illness are targeted because they are thoughtful, curious, and trying hard to get better.
If you are ever unsure about a product or test:
-
ask NAC/CARES
-
ask your specialist
-
or bring it to your next appointment
You deserve real answers — not false hope.

Understanding Risk: How Common Is “Rare”?
When doctors talk about risk, it can sound worrying — especially when you’re already living with a lung condition.
But every day, we all take small, managed risks without realising it.
Understanding how everyday risks compare with medical or vaccine risks helps put the numbers into perspective — and shows why treatment is almost always worth it.
🚶♀️ Everyday activities carry small risks
Everyday life is full of tiny risks we accept because the benefits are clear — exercise, travel, independence, and social connection.
| Activity | Estimated risk of serious harm | Equivalent comparison |
|---|---|---|
| Driving a car for 250 miles | About 1 in 1 million chance of fatal accident | Roughly the same as the risk of a severe vaccine reaction |
| Cycling for 30 minutes | About 1 in 3 million | Similar to being struck by lightning in your lifetime |
| Walking near traffic for a day | Around 1 in 15 million | Negligible, but not zero |
| Taking a domestic flight (UK) | Less than 1 in 10 million chance of fatal accident | Far safer than most road journeys |
| Catching flu during winter | Around 1 in 10 chance of getting ill | Much higher risk than most medicine side effects |
We don’t think of these activities as “dangerous” because the benefit far outweighs the risk — just as it does with most treatments.
💊 Medicines and vaccines we take safely every day
Most common medicines have mild, short-lived side effects. Serious reactions are possible but extremely rare.
| Medicine | Typical mild effects | Serious reactions (approx. frequency) | Comment |
|---|---|---|---|
| Paracetamol (acetaminophen) | Nausea, rash | Serious liver injury ≈ 1 in 100,000 (usually after overdose) | Very safe when taken correctly |
| Ibuprofen | Heartburn, upset stomach | Ulcer or stomach bleed ≈ 1 in 1,000 if used long term | Safer when taken with food |
| Amoxicillin | Diarrhoea, mild rash | Severe allergic reaction ≈ 1 in 5,000–10,000 | Rare but recognised |
| Influenza vaccine | Sore arm, tiredness | Severe allergic reaction ≈ 1 in 1 million | Prevents thousands of serious infections yearly |
| COVID-19 vaccine | Mild flu-like symptoms (≈ 1 in 10) | Severe allergic reaction ≈ 1 in 100,000 | Benefits far outweigh risks |
| Oral steroids (short course) | Increased appetite, insomnia | Major side effects only with prolonged use | Vital during ABPA or asthma flares |
⚕️ What does “serious side effect” really mean?
When you read about serious reactions in medical leaflets or vaccine information, it doesn’t necessarily mean life-changing.
The term “serious” has a specific medical meaning, used by the MHRA, EMA, and WHO.
A reaction is called serious if it:
-
leads to hospitalisation,
-
is life-threatening at the time,
-
causes temporary disability or incapacity,
-
results in death, or
-
causes a birth defect.
👉 It’s about medical urgency, not always long-term harm.
In reality, most serious reactions are short-lived and fully reversible with prompt treatment.
For example:
-
An anaphylactic reaction to a vaccine is medically serious because it needs immediate care — but nearly everyone recovers completely once treated.
-
A high fever or rash that requires a day in hospital may be serious in reporting terms, but causes no permanent damage.
By contrast, life-changing reactions (such as nerve injury or organ failure) are extraordinarily rare — far rarer than being struck by lightning.
“When doctors say ‘serious reaction’, they mean something that needs urgent medical attention — not something that will leave you permanently unwell.”
🩺 More common health risks we all face
While medicine risks are very small, the everyday risks to life and health are much higher — especially if conditions go untreated.
| Health event or cause | Approximate annual risk (UK adult) | Lifetime risk | Notes |
|---|---|---|---|
| Heart attack | Around 1 in 200–300 per year | 1 in 4 men, 1 in 6 women | Increases with age, smoking, and high blood pressure |
| Stroke | Around 1 in 250 per year | About 1 in 5 adults | Preventable with healthy lifestyle and medication |
| Cancer (any type) | Around 1 in 125 per year | Around 1 in 2 people in their lifetime | Most treatable when found early |
| Serious road accident | About 1 in 15,000 per year | Around 1 in 100 lifetime | Far higher than a vaccine reaction |
| Severe flu needing hospital care | Around 1 in 500 per winter | Higher for people with lung disease | Preventable by flu vaccination |
| Fatal asthma attack | About 1 in 100,000 per year | Higher in uncontrolled asthma | Preventable with good management |
| COVID-19 death (current UK levels) | Around 1 in 2,000–5,000 per year for older/vulnerable adults | Major reason vaccination still matters | |
| Lightning strike | About 1 in 15 million per year | Around 1 in 300,000 lifetime | Benchmark for “extremely rare” risk |
⚖️ Making sense of the numbers
-
A 1 in 1,000 risk means one person in a large GP practice might experience it.
-
A 1 in 100,000 risk means one person in a football stadium crowd.
-
A 1 in 1 million risk is so rare that most doctors never see it in their career.
So when you hear that a serious vaccine reaction occurs in one in a million people, that’s about the same as:
-
being struck by lightning once in your life, or
-
winning a small lottery prize several times in a row.
❤️ The real takeaway
The greatest risks to life and health are the common diseases we can prevent or treat — not the rare side effects of treatment.
Every vaccine or medicine is carefully assessed so that its benefits far outweigh its risks, especially for people with asthma, ABPA, bronchiectasis, or weakened immunity.
Treatments don’t add danger — they reduce the much bigger risks from infection, inflammation, and lung damage.
🧭 Key message
We all live with risk, but:
-
Most everyday and health-related risks are far greater than the tiny chance of a medicine reaction.
-
Managing your lung condition well — with the right treatment, vaccines, and follow-up — protects your lungs and lengthens your life.
-
The safest path is always informed care, not avoidance through fear.

🧠 Article 2: Why Awareness Matters – Staying Safe and Confident on Aspergillosis Treatment
Subtitle: How understanding your medicines can protect you and improve your quality of life.
💬 Awareness Means Safety
For people managing aspergillosis or related lung conditions, awareness isn’t just about learning facts — it’s about staying safe.
Knowing how your treatment works, what to expect, and who to ask for help gives you control and confidence.
1️⃣ Awareness Builds Understanding
Understanding each medicine’s purpose helps you:
-
Recognise genuine warning signs early.
-
Avoid anxiety over mild or harmless side effects.
-
Know when something needs professional advice.
Example: a patient who knows voriconazole can cause brief light sensitivity won’t panic, but they will report a new rash or jaundice straight away.
2️⃣ Awareness Improves Communication
Informed patients are better partners in care.
You can explain symptoms clearly, ask the right questions, and notice how medicines affect you.
This helps doctors and nurses tailor treatment quickly and safely.
3️⃣ Awareness Supports Safer Treatment
Many aspergillosis patients take multiple interacting medicines — antifungals, steroids, antibiotics, and sometimes biologics.
Being aware of potential interactions means you can prevent problems before they happen.
You can check interactions using the official
👉 BNF Interactions Checker – NICE Medicines Guidance
(Free, reliable, and used by UK healthcare professionals.)
💡 Tip: If you find a possible interaction online, don’t stop any medicine yourself. Take a screenshot or note and discuss it with your pharmacist or specialist.
🧴 Awareness Includes Working With Your Pharmacist
Pharmacists — both hospital and community — are a vital part of your care team.
They are medicine specialists who can:
-
Review your prescriptions for clashes between antifungals, steroids, and other drugs.
-
Advise how to take medicines for best absorption (for example, itraconazole with food, not with omeprazole).
-
Explain potential side effects and how to manage them safely.
-
Contact your GP or hospital consultant if adjustments are needed.
Whenever you start or stop a medicine — even an over-the-counter painkiller or herbal supplement — let your pharmacist know.
They can quickly check your full medication list using the same professional databases doctors use.
🧭 Remember: Your pharmacist is your first safety checkpoint.
They’re there to protect you, clarify confusion, and help your medicines work safely together.
4️⃣ Awareness Builds Confidence and Control
Long-term illness can feel unpredictable.
Understanding your medicines helps you:
-
Manage flare-ups calmly.
-
Recognise early changes and act quickly.
-
Feel more confident talking with your care team.
Research shows that informed patients have fewer hospital admissions, better symptom control, and improved wellbeing.
⚖️ Balanced Information
Awareness is only helpful if it’s accurate.
Stick to trusted sources such as:
-
aspergillosis.org
-
Your hospital’s patient information leaflets
-
Local or hospital pharmacists who can explain details clearly
Avoid social-media “miracle cures” or alarming headlines that lack evidence.
🌱 The Bottom Line
Awareness doesn’t just make you more knowledgeable — it makes you safer.
Learn what each medicine does, recognise early warning signs, and use trusted resources like the BNF Interactions Checker and your pharmacist to keep your treatment on track.
Awareness turns uncertainty into confidence — and confidence into better health.
🔗 Related Resource
Managing Side Effects of Aspergillosis Treatments » — detailed guide to medicines, monitoring, and how pharmacists and doctors work together to keep you safe.

🩺 Article 1: Managing Side Effects of Aspergillosis Treatments
Subtitle: What to expect, how to recognise problems early, and when to ask for help.
💊 Why This Matters
People living with aspergillosis, bronchiectasis, or Primary Ciliary Dyskinesia (PCD) often take several medicines for months or even years.
These drugs are vital for controlling infection, inflammation, and allergic reactions — but they can also cause side effects or drug interactions.
Being aware of what’s normal, what’s not, and when to seek help helps you stay safe while getting the most from treatment.
⚗️ Antifungal Medicines
Antifungal (azole) drugs are the backbone of treatment for Chronic Pulmonary Aspergillosis (CPA) and Allergic Bronchopulmonary Aspergillosis (ABPA).
They control infection but can affect the liver, heart, or skin, so regular blood monitoring is essential.
Itraconazole (Sporanox® / generic)
Used for long-term control in CPA and ABPA.
-
Common: tiredness, nausea, ankle swelling, blurred vision.
-
Serious: yellowing skin/eyes, dark urine, shortness of breath.
-
Tips:
-
Take with a main meal or fizzy drink (acidic stomach aids absorption).
-
Avoid taking it with omeprazole or similar acid-reducing drugs, as these block absorption.
-
Have regular liver-function and drug-level blood tests.
-
Report ankle swelling or jaundice immediately.
-
Voriconazole (Vfend®)
Used when itraconazole isn’t effective or tolerated.
-
Common: temporary visual flashes or blurred vision, sunlight sensitivity, mild headache.
-
Serious: severe rash, blistering, or long-term skin-cancer risk from sunlight.
-
Tips:
-
Always use SPF 30+ sun cream, even in winter.
-
Avoid prolonged sun exposure.
-
Report any visual change, rash, or fatigue promptly.
-
Blood monitoring checks for safe drug levels.
-
Posaconazole (Noxafil®)
Used for resistant infections or as a second-line therapy.
-
Common: nausea, diarrhoea, fatigue.
-
Serious: liver inflammation, low potassium (causing muscle cramps or irregular heartbeat).
-
Tips:
-
Take with a main meal or full-fat snack.
-
Report unexplained muscle weakness or palpitations.
-
Keep up with blood tests.
-
Isavuconazole (Cresemba®)
A newer antifungal option that may cause fewer interactions.
-
Common: headache, mild nausea, ankle swelling.
-
Tips:
-
Continue regular liver and kidney checks.
-
Report any new swelling, fatigue, or breathlessness.
-
💨 Corticosteroids
(Prednisolone, Methylprednisolone, Hydrocortisone)
These reduce inflammation and allergic response in ABPA and asthma.
They are powerful — but long-term use can affect weight, mood, bones, and hormone balance.
-
Common: increased appetite, fluid retention, mood swings, difficulty sleeping.
-
Long-term: thinning bones, higher blood sugar, adrenal suppression.
-
Tips:
-
Never stop suddenly — always taper under medical advice.
-
Carry a Steroid Emergency Card.
-
Ask about bone protection (vitamin D, calcium, bisphosphonates).
-
See your GP if you feel very tired, dizzy, or unwell.
-
🧬 Biologic Treatments
(Mepolizumab, Benralizumab, Omalizumab)
These injection-based medicines target inflammation or allergic responses in severe asthma or ABPA.
-
Common: mild injection-site soreness, tiredness, headache.
-
Occasional: mild fever or muscle aches.
-
Serious: allergic swelling of lips, tongue, or throat.
-
Tips:
-
Record any mild reactions.
-
If you develop swelling or difficulty breathing, call 999 immediately.
-
💊 Long-Term Antibiotics
(Azithromycin, inhaled colomycin, tobramycin)
Used to reduce bacterial infections in bronchiectasis or PCD.
-
Common: stomach upset, diarrhoea, mild throat irritation.
-
Long-term: tinnitus or hearing loss (especially with azithromycin).
-
Tips:
-
Have periodic hearing checks.
-
Rinse mouth and nebuliser after inhaled antibiotics.
-
Report ringing in the ears, severe diarrhoea, or rash.
-
⚠️ Drug Interactions
Antifungal medicines (especially azoles) can interfere with many common drugs, including:
-
Steroids (e.g., prednisolone, fluticasone) — may increase steroid levels.
-
Reflux medicines (e.g., omeprazole, lansoprazole) — reduce antifungal absorption.
-
Statins and warfarin — increase risk of side effects or bleeding.
-
Some antihistamines and antibiotics — can affect heart rhythm.
These interactions can be complex — always check before starting or stopping any medication.
✅ Check it yourself:
You can use the official BNF Interactions Checker (NICE Medicines Guidance) to see if two medicines are known to interact.
Simply type the names (e.g., itraconazole and prednisolone) and it will show the risk level, what the interaction does, and what clinicians usually recommend.
If unsure, show the result to your GP, pharmacist, or hospital team — they can interpret it for your situation.
🚨 When to Seek Help
Call your specialist or GP urgently if you notice:
-
Yellowing of skin or eyes
-
Severe rash, blistering, or peeling
-
New ankle swelling or breathlessness
-
Sudden fatigue or dark urine
-
Visual changes or increased photosensitivity
-
Ringing in the ears or hearing loss
If you feel acutely unwell, do not stop your medication abruptly — contact your hospital team or emergency services.
🔗 Next read: Why Awareness Matters – Staying Safe and Confident on Aspergillosis Treatment »
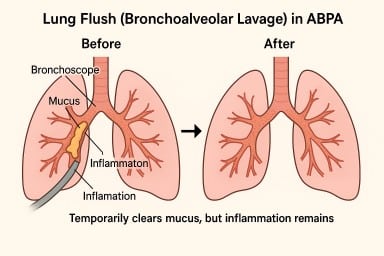
🫁 “Lung Flush” (Bronchoalveolar Lavage) in ABPA – What It Is and Why It Brings Only Short-Term Relief
A lung flush (also called a bronchoalveolar lavage, or BAL) isn’t a regular treatment for Allergic Bronchopulmonary Aspergillosis (ABPA), but it’s sometimes used selectively in NHS hospitals.
💧 What Happens During a Lung Flush
It’s done during a bronchoscopy, where a thin, flexible tube is passed through the nose or mouth into the lungs.
A small amount of sterile saline is washed into part of the lung and then gently suctioned back out.
The fluid is tested for:
-
Aspergillus growth or DNA
-
Other infections (bacteria, fungi, viruses)
-
Signs of inflammation or allergic activity
You’re given local anaesthetic and light sedation, so you stay comfortable but sleepy. Most people go home the same day.
🧪 Main Purpose – Diagnosis
In most ABPA cases, a lavage is done to find out what’s causing symptoms – whether they’re due to Aspergillus, another infection, or ongoing inflammation.
The results help doctors fine-tune treatment, such as adjusting antifungal doses or deciding if a biologic drug might help.
🫁 Sometimes Used to Clear Mucus
In certain situations – especially when thick mucus plugs are blocking airways or causing part of a lung to collapse – doctors may use lavage as a therapeutic “flush.”
This can wash out sticky secretions and temporarily improve airflow, helping physiotherapy and medication work more effectively.
It’s usually a short, day-case procedure, and most people feel back to normal after a day or two.
⚠️ Why It’s Only Short-Term Relief
Although lavage can clear mucus, ABPA is caused by an allergic immune reaction, not by the mucus itself.
Unless that reaction is controlled with:
-
Corticosteroids (to reduce inflammation),
-
Antifungal drugs (to lower the fungal load), or
-
Biologic injections (to block allergy pathways),
…the lungs will continue to produce thick, sticky mucus, which can re-accumulate within days or weeks.
So while a “lung flush” can make breathing easier in the short term, the effect is temporary – like clearing a blocked drain while the tap is still running.
⚠️ Risks and After-Effects
A bronchoscopy with lavage is generally safe, but it is still an invasive procedure. Possible effects include:
-
Temporary sore throat, cough, or hoarseness (common)
-
Mild bleeding or streaks of blood in sputum for a short time
-
Low oxygen levels during or after the procedure (monitored carefully)
-
Chest tightness, infection, or fever – uncommon but possible
-
Bronchospasm (airway narrowing) in people with very sensitive lungs, which is why it’s done in a hospital with respiratory support available
Because of these small but real risks, the NHS uses lavage only when the benefits outweigh the downsides – for example, when mucus is causing serious blockage or when test results will change management.
💬 In Summary
A “lung flush” can temporarily clear mucus and ease breathing, but it doesn’t stop ABPA’s underlying allergic inflammation.
The mucus often returns unless that inflammation is brought under control with long-term medical treatment.
It’s a useful tool when needed, but not something done regularly or lightly.

🏥 NHS Neighbourhood Health Hubs: How Community Care Will Work for People with Aspergillosis and Asthma
The NHS is changing how healthcare is delivered — with more care moving closer to home and fewer hospital visits.
A new model called Neighbourhood Health Services (or Neighbourhood Health Hubs) is being rolled out across England from late 2025, and it could make a real difference for people living with aspergillosis, asthma, bronchiectasis, and other long-term respiratory conditions.
🌍 Why care is moving into the community
The goal is to:
-
Bring care to where people live, not just in large hospitals
-
Reduce waiting times by shifting routine tests and reviews out of hospital clinics
-
Join up GPs, nurses, pharmacists, and hospital specialists into one local team
-
Focus on prevention, self-management, and early support
These reforms come from the government’s Healthcare on Your Doorstep announcement (September 2025), supported initially by £10 million across 43 pilot areas in England.
🧑⚕️ What a “Neighbourhood Health Hub” looks like
A one-stop local health centre bringing together:
-
GPs and practice nurses
-
Respiratory nurses, physiotherapists, and pharmacists
-
Mental-health and wellbeing workers
-
Dietitians, occupational therapists, and social-prescribing link staff
-
Voluntary and community organisations (e.g. NAC CARES, Asthma + Lung UK)
Some hubs will connect directly to Community Diagnostic Centres (CDCs) – local sites providing CT, MRI, X-ray, lung-function and blood tests through the NHS England diagnostics programme.
The aim is for one joined-up team to share your records and plan your care locally.
🩺 How hubs work with your GP and A&E
The new hubs are designed to fill the gap between GP surgeries and hospitals – giving extra support when you’re too unwell to manage alone but don’t need emergency care.
🏠 Your GP surgery
You’ll stay registered with your usual GP. They remain in charge of your prescriptions, results, and overall care.
Your GP can now refer you to a Neighbourhood Health Hub for things that need a wider team – for example:
-
Antifungal monitoring or blood tests
-
Lung-function or CT scans
-
Flare-up review by respiratory nurses
-
Fatigue or wellbeing support
🧑⚕️ The Neighbourhood Health Hub
You might go here instead of hospital for:
-
Same-day assessment of an infection or flare-up
-
Bloods, ECGs, or scans ordered by your GP
-
Physiotherapy, airway-clearance or rehabilitation
-
Medication reviews with a pharmacist
-
Appointments with dietitians or mental-health staff
-
Practical help from link workers (see below)
🚨 A&E (Emergency Department)
Still essential for serious problems such as:
-
Sudden or severe breathlessness not relieved by treatment
-
Coughing up blood
-
Chest pain, fainting, or collapse
-
High fever with confusion
If unsure, call NHS 111 or 999 in an emergency.
🔁 When to use which service
| Situation | Who decides | Where you’ll be seen |
|---|---|---|
| Routine check-up or repeat prescription | You / GP | GP surgery |
| Specialist review or complex medication | GP / consultant | Neighbourhood Hub |
| Mild flare-up needing same-day care | NHS 111 / GP | Hub or GP |
| Emergency or life-threatening symptoms | NHS 111 / 999 | A&E / hospital |
| Diagnostic tests | GP / hospital referral | Community Diagnostic Centre |
All sites will share your digital care record so results and updates reach your GP and hospital team automatically.
🧑🤝🧑 Link workers and care coordinators – local help through your GP
Every GP practice and neighbourhood team now has link workers (also called care coordinators or social prescribers).
They’re there to help you navigate healthcare and community support. They can:
-
Arrange or advise on transport for appointments
-
Help complete travel cost reimbursement or benefit forms
-
Connect you with volunteer driver schemes or local charities
-
Find exercise, wellbeing, or peer-support groups
-
Support with fatigue, isolation, or anxiety
Ask your GP reception or Neighbourhood Hub to refer you to the link worker, or request a call-back via the NHS App.
🚗 Transport and accessibility
🚐 NHS Patient Transport Service (PTS)
If you can’t use public transport for medical reasons (for example, oxygen use, mobility difficulties, or severe fatigue), you may qualify for free NHS transport.
Your GP, link worker, or hospital can book this for you through the regional PTS (for example, NWAS in the North West).
💷 Healthcare Travel Costs Scheme (HTCS)
If you’re on a low income or certain benefits, you can reclaim travel expenses under the HTCS.
Bring your appointment letter and proof of eligibility, or ask your link worker to help with the form.
🚙 Community & volunteer transport
Each Integrated Care System (ICS) works with local councils and charities such as Age UK, Mind, or Good Neighbour schemes to run community minibuses and volunteer driver services.
Ask your link worker or hub team for local options.
🅿️ Accessibility
All new and refurbished hubs must include:
-
Blue Badge parking and drop-off zones
-
Wheelchair-friendly entrances and toilets
-
Seating and oxygen-safe waiting areas
-
Negotiated free or reduced parking in shared sites
🧭 At a glance
| Issue | What’s planned | What to do now |
|---|---|---|
| Public transport | Sites chosen to be local, but not always central | Check routes before your visit |
| NHS Patient Transport | Still available for medical need | Ask GP or link worker to book |
| Travel-cost reimbursement | Continue via HTCS | Keep proof of benefit |
| Community / volunteer drivers | Expanding under ICB–VCS partnerships | Request info via link worker |
| Disabled parking / drop-off | Required at new sites | Confirm when booking |
🪶 A message from the aspergillosis community
For many people with lung disease, “local care” only works if it’s accessible care.
Groups such as NAC CARES, Asthma + Lung UK, and Healthwatch are urging NHS leaders to:
-
Design transport and parking into every new site
-
Ask about mobility and oxygen needs when booking
-
Fund local volunteer schemes
-
Provide dedicated link workers at every hub and GP practice
If you struggle to reach appointments, tell your clinic or Healthwatch — your feedback shapes how services develop.
🧾 Questions to ask before your first visit
-
🚗 Is there Blue Badge or patient parking on site?
-
🚌 What public-transport links serve the hub?
-
🚐 Can the clinic arrange NHS Patient Transport?
-
💷 Can I claim travel costs under the HTCS scheme?
-
♿ Is the building accessible for wheelchairs or oxygen users?
-
💨 Are there rest areas for people who get breathless?
-
🧑🤝🧑 Can my carer or partner attend with me?
-
👩💼 Is there a link worker who can help with transport or forms?
-
🕓 Are there quiet waiting spaces to reduce infection risk?
Having these answers before your appointment makes your visit smoother and safer.
💬 Final thought
“Neighbourhood care” isn’t about replacing your GP or A&E — it’s about bridging the gap.
The new hubs aim to bring together your GP, hospital specialists, and community teams in one local setting, providing earlier help, fewer hospital journeys, and care designed around your life, not your postcode.
🔎 Behind the Headlines: Is this an NHS Expansion or a Shift?
Many people wonder whether this is new investment or a reshuffle of existing NHS services.
🧱 What’s really happening
-
The Neighbourhood Health Service is not a new tier of the NHS, but a redesign of how GP, hospital, and community teams work together.
-
The focus is on moving care out of hospitals and into local clinics, using the same staff and budgets more effectively.
-
Hospitals will still handle emergencies and complex cases, but routine tests, reviews, and education will move into the hubs.
⚖️ Expansion or movement?
| Area | Expansion | Reorganisation |
|---|---|---|
| Buildings | Some new or refurbished hubs and diagnostics centres | Many reusing existing GP or community facilities |
| Staffing | Some new link workers, pharmacists, and AHPs | Most existing NHS staff redeployed across neighbourhoods |
| Funding | £10m pilot investment + diagnostic capital | No major long-term new funding yet announced |
| Patient benefit | Easier access, joined-up records | May reduce hospital appointments rather than add capacity |
💬 What this means
For patients, it should feel like an expansion — more care, closer to home —
but in reality it’s a shift of where and how NHS services are delivered, not a large-scale increase in total NHS resources.
⚠️ Risks and opportunities
| Opportunities | Risks |
|---|---|
| Easier local access | Risk of hospital clinics closing before hubs fully staffed |
| Joined-up records | Depends on IT integration |
| Focus on prevention | May feel like hospital services are being reduced |
| Better continuity | Needs clear accountability (GP vs hub) |
🧩 Summary
The new neighbourhood model is a reorganisation within the NHS, not a separate expansion.
It aims to use existing staff, buildings, and budgets more efficiently — giving patients with chronic conditions like aspergillosis and asthma easier access to care and support in their own communities.

Mannose-Binding Lectin (MBL) Deficiency and Aspergillosis
What is MBL?
Mannose-binding lectin (MBL) is a natural protein made by the immune system. Its job is to help the body recognise and fight off germs, including fungi like Aspergillus. It’s part of the “innate” immune system – the first line of defence you’re born with.
How common is MBL deficiency?
MBL deficiency is surprisingly common.
-
Around 5–10% of people have very low or absent levels.
-
If you include milder reductions, as many as 20–30% of people carry genetic changes that lower MBL activity.
For most, this causes no problems because the immune system has other pathways to fall back on. People often never know they have it.
Why do MBL levels vary?
-
Genetics: The MBL2 gene comes in different versions, some producing plenty of MBL and others producing little or none.
-
Inheritance: The combination of gene copies from each parent determines your level.
-
Normal diversity: Low levels are common and often harmless, showing the immune system has strong backup pathways.
Are some people born more vulnerable to infection?
Yes – but it depends on the situation.
-
Children with very low MBL may get more ear, chest, or sinus infections while their immune systems are developing.
-
In adults, MBL deficiency usually only matters if there are other risks, such as chronic lung disease, immune suppression, or another immune problem.
-
Many people with low MBL live their whole lives without extra infections.
MBL deficiency and aspergillosis
On its own, MBL deficiency rarely causes illness. But in people who already have other risks – such as lung disease (COPD, asthma, bronchiectasis, or TB damage) or a weakened immune system – it may make infections more likely.
Research suggests MBL deficiency can be linked to:
-
Chronic pulmonary aspergillosis (CPA)
-
Allergic bronchopulmonary aspergillosis (ABPA)
-
Invasive aspergillosis in people with suppressed immunity
In these cases, MBL deficiency is not the single cause of aspergillosis, but it may be one of several factors that increase vulnerability.
Can MBL deficiency be treated?
At present, there is no routine treatment to replace MBL itself. Research has explored giving purified MBL, but it hasn’t become a standard therapy – largely because deficiency is so common and most people remain healthy without intervention.
Instead, management focuses on:
-
Treating infections promptly with antibiotics or antifungals
-
Sometimes using preventive (prophylactic) antibiotics or antifungals in people with frequent or severe infections
-
Using immunoglobulin replacement therapy if there are additional immune problems
-
Supporting lung health and reducing risks with vaccinations, good self-care, and specialist monitoring
Why measure MBL if it can’t be treated directly?
Even without a direct treatment, measuring MBL can still be useful:
-
Helps explain recurrent infections – finding a low MBL level can give part of the reason why someone is more prone to infections.
-
Part of a bigger immune work-up – it’s often checked alongside other immune tests, and the overall pattern may guide treatment decisions.
-
Risk awareness – knowing about low MBL can make doctors more proactive with antibiotics, antifungals, or vaccinations, and encourage earlier treatment at the first sign of infection.
-
Research value – helps specialists understand why some people develop aspergillosis while others don’t.
Why hasn’t evolution eliminated low MBL?
-
Common worldwide: 5–10% of people have very little MBL, and up to 30% have reduced levels. If this were a major disadvantage, numbers would be lower.
-
Other immune pathways compensate: The body has strong backup systems, so many people stay healthy even with low MBL.
-
Possible advantage: In some infections, high MBL may drive too much inflammation. Lower MBL might have protected against diseases like leprosy or TB.
-
Changing disease patterns: In the past, people rarely lived long enough for chronic lung disease to show the effects of low MBL. Today, with longer lives and modern medicine, its role is more visible.
👉 In short: low MBL has not been “selected out” by evolution because it usually isn’t harmful on its own, and in some situations it may even have been protective.
What this means for patients
-
Having MBL deficiency is quite common and usually harmless.
-
It may become more relevant if you also have underlying lung disease or are on treatments that suppress the immune system.
-
If MBL deficiency is suspected, doctors may check for it as part of a wider immune work-up.
-
The key point: treatment is aimed at managing infections and lung health, not the MBL level itself.
👉 In short: MBL deficiency is common in the general population. Most people never notice it, but for some with lung disease or weakened immunity, it may add to the risk of aspergillosis. While there’s no direct treatment for the deficiency, testing can help explain recurrent infections, guide wider immune checks, and shape preventive care.
Why the NHS doesn’t use unvalidated tests (and why that’s not just being awkward)
It can feel frustrating when the NHS won’t accept private tests like mycotoxin panels, IgG food intolerance kits, or home mould testing. But this isn’t about being difficult — it’s about protecting patients and making sure care is fair, safe, and effective.
-
Safety first
Unvalidated tests can give false positives (saying you have a problem when you don’t) or false negatives (missing something important). Acting on the wrong result could lead to unnecessary medication, restrictive diets, or missed diagnoses. -
Evidence matters
NHS doctors can only use tests that have been proven in research to give accurate, meaningful results. That way, they can be confident the result will actually help guide treatment. -
Protecting patients from harm
Many private tests are expensive and may push people toward costly supplements, detox regimes, or antifungals they don’t need. The NHS avoids recommending anything that risks harm or waste. -
Fairness and trust
The NHS has to provide care that is fair for everyone. That means sticking to tests and treatments that have passed strict checks for accuracy, safety, and usefulness.
💙 Key message: When the NHS says “we can’t use that test,” it’s not about being awkward or dismissive — it’s about making sure that what’s offered is safe, reliable, and genuinely helps patients.
Private companies that sell mycotoxin or food intolerance tests will naturally try to justify their services — it’s their business, after all. But before you spend money, it’s worth asking one key question: ‘Will my NHS doctor be able to use these results to guide my treatment?’ If the answer is no (and in most cases it is), then you may just be spending a lot of money without getting anything useful for your care.
That doesn’t mean your symptoms aren’t real — it just means these particular tests aren’t the right tool. NHS doctors can only act on validated results (like CT scans, Aspergillus antibody blood tests, or sputum cultures) because those are proven to be accurate and safe.

🩺 Monitoring your health at home with aspergillosis
Many people with aspergillosis (ABPA, CPA, SAFS, aspergillus bronchitis) now use home devices such as pulse oximeters, blood pressure monitors, and thermometers. These are very useful tools — but only if you know how to take reliable measurements and when to act on them.
⚠️ Important: These devices are only guides. If you feel unwell, worsening, or unsafe — seek help, even if the numbers look “normal.” How you feel is always more important than a single reading.
This guide explains:
-
✅ How to measure correctly
-
🟢 When to relax, 🟠 when to monitor, 🔴 when to seek help
-
⚠️ What’s different if you have other health conditions
📏 How to take reliable measurements
🌡 Temperature
-
Use a digital thermometer (ear, mouth, or underarm).
-
Take your temperature at the same time each day when well, to learn your baseline.
-
Avoid measuring straight after a hot drink, bath, or exercise.
-
Always use the same device and method for consistency.
-
⚠️ Normal isn’t the same for everyone:
-
Typical range is 36.1–37.2 °C.
-
Some people naturally run a little “cooler” or “warmer.”
-
Temperature changes with time of day, age, hormones, and medicines (e.g. steroids, paracetamol).
-
Your personal baseline is most important.
-
💨 Oxygen saturation (SpO₂)
-
Sit quietly and rest for 5 minutes before checking.
-
Warm your hands — cold fingers reduce accuracy.
-
Remove nail polish, gel nails, or false nails.
-
Place the oximeter on your index or middle finger.
-
Keep your hand still, relaxed, and at heart level.
-
Wait 30–60 seconds until numbers settle, then record both SpO₂ and pulse.
❤️ Pulse rate
-
Normally shown on your oximeter.
-
Measure when sitting calmly.
-
If irregular, double-check manually by counting your pulse at the wrist or neck for 30 seconds ×2.
-
Record alongside oxygen reading.
🔹 Blood pressure (BP)
-
Rest for 5 minutes before measuring.
-
Use the same arm each time (usually left).
-
Keep your arm supported at heart level.
-
Sit with feet flat on the floor, legs uncrossed.
-
Avoid caffeine, smoking, or exercise for 30 minutes before.
-
Take two readings, 1–2 minutes apart, and record the average.
📝 Recording results
-
Note date, time, reading, and how you feel.
-
Keep a diary or use an app to spot trends over time.
-
Share with your GP or specialist, especially if you reach “amber” or “red” zones.
📊 When to seek help — traffic light system
⚠️ Don’t rely on numbers alone. If you feel unwell, dizzy, very breathless, confused, or unsafe, seek medical help — even if your readings are in the “green” zone.
🌡 Temperature
-
Green (OK): Within your baseline range.
-
Amber (monitor/GP): ≥37.5 °C repeatedly, or ≥1 °C above your baseline.
-
Red (urgent help): ≥38 °C once with feeling unwell; any fever with severe breathlessness, chest pain, or confusion.
💨 Oxygen saturation (SpO₂)
-
Green (OK): 93–100% (or your personal baseline).
-
Amber (monitor/GP): Drop of ≥3% from normal; persistent 89–92% at rest; dips after mild exertion that recover slowly.
-
Red (urgent help): ≤88% at rest, or sudden fall with confusion, blue lips/fingers, severe breathlessness.
❤️ Pulse rate
-
Green (OK): 60–100 bpm at rest, regular.
-
Amber (monitor/GP): >100 but <120 bpm; <50 bpm with fatigue/dizziness; irregular pulse.
-
Red (urgent help): >120 bpm at rest; chest pain, collapse, or fainting.
🔹 Blood pressure (BP)
-
Green (OK): 100/60 – 140/90 (unless advised otherwise).
-
Amber (monitor/GP): Systolic >150 or <95; diastolic >95 or <60 on repeated readings.
-
Red (urgent help): ≥180/110, or systolic <80 with dizziness, fainting, or collapse.
⚠️ Comorbidities: special considerations
If you have other health conditions, your safe ranges may be different:
-
COPD or severe chronic lung disease → Oxygen targets are usually 88–92% (not higher).
-
Heart disease or pulmonary hypertension → Leg swelling + falling oxygen may need urgent review.
-
Atrial fibrillation / irregular heart rhythm → Oximeters may give unreliable pulse readings. Confirm with your GP or specialist.
-
Diabetes or thyroid problems → Can affect pulse rate and blood pressure; your “green” zone may differ.
-
Kidney disease, diabetes, cardiovascular disease → Stricter BP targets may apply (often <130/80).
-
Older age or steroid/immune-suppressing treatment → You may not get a high fever with infection. Even a small rise above your baseline could be important.
👉 Always ask your clinician:
-
“What’s my personal safe oxygen range?”
-
“What blood pressure or pulse numbers should trigger a call for me?”
⚠️ Other warning signs to act on
-
Sudden increase in sputum (more volume, colour change, or blood-streaked)
-
Fever with worsening cough or breathlessness
-
Rapid swelling of legs, ankles, or abdomen
-
New confusion, drowsiness, or severe fatigue
🟢 AMBER RED system
-
Green: Stay calm, record readings.
-
Amber: If new or persisting >24–48 hours, contact your GP or specialist.
-
Red: Seek urgent medical help (999 / A&E).
✅ Key message:
Home monitors are helpful, but they don’t replace how you feel. Always act on symptoms first — numbers are just part of the picture. If in doubt, seek medical advice.