Many people living with…
by GAtherton
What the latest British…
Understanding why everyday…
Recently, several newspapers…
Awaab’s Law is one of the…
It’s quite possible for…
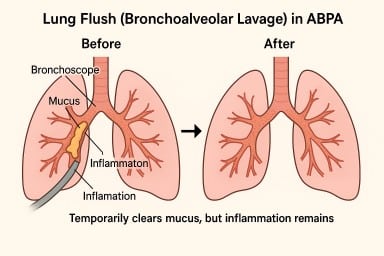
A lung flush (also called a…
Many people with asthma, ABPA…