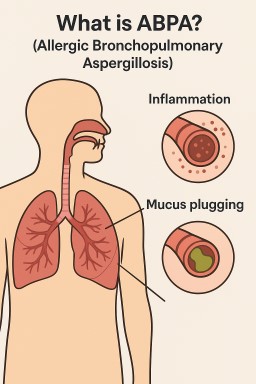
Many patients with ABPA,…
by GAtherton
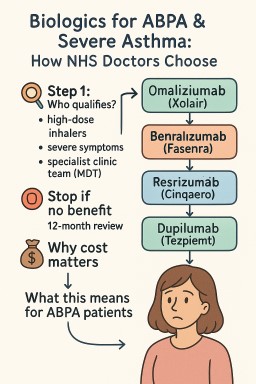
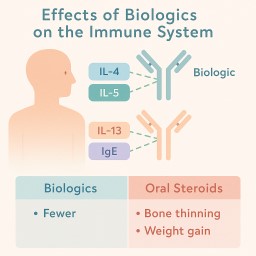
Biologics are modern…
Print out or share…
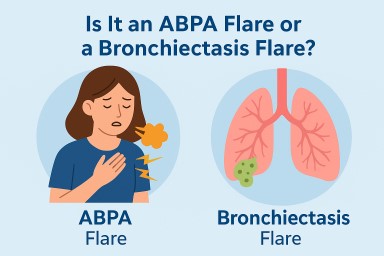
Patient handout for A&E…
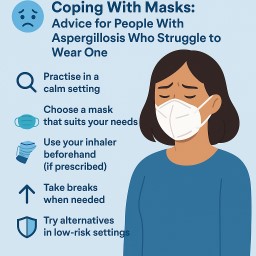
If you have aspergillosis,…
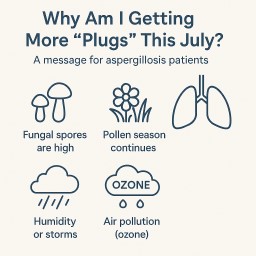
A message for aspergillosis…
✅ What Are Biologics?…
For people living with…
Mask Type Who Might Use……