
🌿 Why We All Need to Advocate for Ourselves as the NHS Faces Change and Pressure
A patient-friendly guide to staying safe and getting the care you need
The NHS is going through one of the most challenging periods in its history. Services are under pressure, staff are stretched, and backlogs remain high across nearly every speciality. None of this is the fault of patients or staff — it’s the reality of a system trying to do too much with too little.
In times like this, one thing becomes more important than ever:
⭐ Advocating for your own health.
Advocacy simply means speaking up when you need help, asking questions, and making sure your concerns are heard. It’s not about complaining or demanding; it’s about ensuring you get the support, information, and care you deserve.
Here’s why it matters — and how to do it safely and confidently.
🔍 1. Some things no longer happen automatically
With so many clinics running over capacity, routine tasks can be delayed or missed:
-
Follow-up appointments don’t always get booked
-
Test results aren’t always communicated quickly
-
Reviews may slip off the system
-
New medications sometimes aren’t monitored as closely as they should be
This isn’t because your team doesn’t care.
It’s because the system is stretched.
Advocating for yourself helps fill the gaps.
💬 2. Asking questions keeps you safer
If something is unclear — a result, a new medication, a change in symptoms, or a delay — asking for clarification is not only reasonable, it’s sensible.
Good questions to ask:
-
“When should my next review be?”
-
“Who do I contact if I have a problem?”
-
“What symptoms should I watch for?”
-
“Is there a plan for monitoring?”
Healthcare teams want patients to feel informed.
They would rather you ask than worry in silence.
📞 3. The NHS wants patients to raise concerns early
Early contact helps prevent:
-
deteriorations
-
emergency admissions
-
medication complications
-
worsening long-term conditions
Services rely on patients saying, “Something isn’t right.”
It’s an essential part of safe care, not an inconvenience.
🧭 4. The NHS is changing — and patients play a role in shaping care
Integrated Care Systems (ICS), value-based care, and new digital pathways are all evolving.
These changes aim to make care:
-
more personalised
-
more consistent
-
more focused on real outcomes
But during transitions, there are bumps in the road.
Patient feedback — including when something hasn’t worked — helps services identify where improvements are needed.
You are part of shaping that improvement.
❤️ 5. You deserve to be heard
Many patients worry about “bothering” the NHS.
But advocating for yourself is:
-
responsible
-
appropriate
-
encouraged
-
part of keeping long-term conditions well-managed
You are not asking for anything unreasonable.
You are simply making sure your health is looked after.
🌼 6. How to advocate confidently
Here are gentle, effective ways to speak up:
Be clear
“I haven’t had a review since starting this treatment — can we arrange one?”
Be specific
“I’m unsure who to contact if I worsen. Could you give me the correct number?”
Be persistent if needed
“It’s been a few weeks since I asked — could you update me on the appointment?”
Keep records
Dates, names, symptoms, and messages help everything run more smoothly.
Ask for your named clinician or team
Every patient is entitled to know who oversees their care.
🌟 7. You are not alone — and it’s OK to ask for help
Advocacy doesn’t mean you carry the burden alone.
Groups like NAC, patient communities, and charities can help you:
-
understand the system
-
find the right contacts
-
prepare questions
-
know what to expect
-
get support if you’re struggling to be heard
Empowering yourself helps others too — the more patients speak up, the more the system adapts.
💚 In summary
The NHS is still full of dedicated people who care deeply about their patients.
But the reality of high demand and limited capacity means:
We all have to be a little more active in asking for what we need.
Advocating for your own health is:
-
responsible
-
protective
-
empowering
-
part of modern healthcare
It ensures you get the right care at the right time — and it helps the NHS deliver safer, more responsive services.

⚠️ Flu Season Warning: UK Flu Cases Are Now Surging — Dominated by a Drifted H3N2 Strain
The UK flu season has begun much earlier and much faster than usual, and cases are now surging across the country. The UK Health Security Agency (UKHSA) confirms that the dominant strain this year is a drifted influenza A(H3N2) variant (sub-clade K). This strain now accounts for the vast majority of flu cases in people tested.
🔥 Why this flu season is different
-
Almost all flu cases are influenza A, and around 84% of typed cases are H3N2.
This pattern is consistent across community, GP and hospital surveillance. -
The H3N2 strain circulating is genetically drifted, meaning it has evolved away somewhat from the reference vaccine strain.
UKHSA has publicly confirmed this drift. -
This increases the risk of infection spreading rapidly — which is exactly what is happening now.
🛡️ Does the flu vaccine still work?
Yes — despite the drift, UKHSA reports that the 2025–26 flu vaccine still provides important protection, including:
-
~70–75% effectiveness in children
-
~30–40% effectiveness in adults
This means vaccination dramatically reduces severity, even if it does not fully prevent infection.
⚠️ Why this matters for people with lung conditions
If you have:
-
ABPA (Allergic Bronchopulmonary Aspergillosis)
-
Bronchiectasis
-
Asthma
-
Chronic lung disease
…you are at higher risk of: -
pneumonia
-
severe chest infections
-
hospitalisation
-
long recovery times
H3N2 seasons are historically worse for adults and people with underlying respiratory disease.
🔺 What you should do now
1. Get vaccinated immediately
If you haven’t had your flu jab yet, do not wait.
The season is already surging and accelerating earlier than usual.
2. Be extremely cautious in high-risk environments
-
Schools
-
Public transport
-
Healthcare settings
-
Large indoor gatherings
-
Poorly ventilated rooms
3. Use winter protection behaviours
-
Ventilate indoor spaces
-
Consider wearing a mask in crowded indoor areas
-
Wash hands frequently
-
Avoid contact with people who are unwell
4. If you become ill — act fast
For anyone with ABPA, bronchiectasis or asthma:
-
A sudden fever
-
A sharp rise in cough
-
Change in sputum
-
Chest tightness
-
Breathing changes
…should be treated as early warning signs.
Contact your GP or respiratory team quickly, as secondary pneumonia is more likely in H3N2 seasons.
Summary
Flu is now surging across the UK, driven by a drifted H3N2 strain, and people with underlying lung disease should take this season particularly seriously.
Vaccination remains strongly protective, but additional precautions are vital during this rapid upswing in cases.

💙 The NHS Is Changing: What “Value-Based Healthcare” Means for People with Aspergillosis
The NHS is beginning to look not just at how many people it treats, but how well those treatments work — and whether every pound spent makes the biggest difference to patients’ lives.
This idea is called value-based healthcare (VBHC).
🧭 What “value” means
In simple terms, value =
Better health and quality of life for patients ➗ the resources and effort used to achieve it.
It’s not about cutting care.
It’s about making sure time, money, and medicines are used where they bring the greatest benefit — especially for people with long-term or complex conditions like aspergillosis.
⚙️ From “productivity” to “value”
Until now, the NHS has mostly measured productivity — how many people are seen, how many tests or treatments are delivered, and how quickly.
That approach works for short-term or simple care (like hip replacements or cataract surgery), but it doesn’t tell the full story for complex, long-term conditions such as aspergillosis, where the real goal is to stay well, avoid hospital admissions, and maintain a good quality of life.
So, over the next few years, these older productivity measures will gradually be replaced or balanced with value-based measures that ask:
“Did this care actually help patients live better and longer — and was it a good use of NHS resources?”
This means success will be judged more on outcomes and experience than on numbers and speed.
🌿 Why this matters for people with aspergillosis
Aspergillosis, whether Allergic Bronchopulmonary Aspergillosis (ABPA) or Chronic Pulmonary Aspergillosis (CPA), is often complicated and different for every patient.
Traditional NHS targets — such as waiting times or the number of appointments — don’t always show whether patients are breathing easier, feeling stronger, or coping better at home.
Value-based care changes that by focusing on:
-
Real health outcomes – fewer flare-ups, better lung function, reduced fatigue
-
Patient experience – how well care fits your needs, and how supported you feel
-
Sensible use of treatments – balancing benefit, side effects, and cost
-
Joined-up care – making sure specialists, GPs, and community teams work together smoothly
🏥 How the National Aspergillosis Centre (NAC) fits in
The National Aspergillosis Centre (NAC) already works in a value-based way:
-
It tracks outcomes such as infection control, hospital admissions, and steroid use
-
It listens to patients through groups, surveys, and education sessions
-
It combines research, expert treatment, and patient partnership to improve care
-
It shares learning with hospitals across the UK
As the NHS moves further toward value-based care, NAC’s approach — measuring what really matters to patients — is exactly the kind of model the health service wants to grow.
🔄 What might change over the next few years
You may start to notice:
-
More focus on your experience and progress: you might be asked to fill in short questionnaires about symptoms and quality of life (called Patient-Reported Outcome Measures or PROMs).
-
Better coordination between hospital, GP, and community teams — digital health records will help your care stay connected.
-
New measures of success: NAC may report things like “flare-ups prevented” or “improvement in wellbeing” rather than only how many people were seen.
-
More evidence about what works: shared data will help identify which treatments or combinations give the most benefit.
⚠️ What it does not mean
-
It doesn’t mean fewer services or reduced access for people with complex lung disease.
-
Rare conditions like aspergillosis will continue to need specialist national centres because they provide expert care that general services can’t.
-
The goal is to show that centres like NAC deliver high value — preventing complications, reducing hospital stays, and improving lives.
💬 What you can do
-
Give feedback about your health and care — this helps measure real outcomes.
-
Take part in surveys or PROMs if asked — these are how value is proven.
-
Stay involved in patient groups and discussions — your voice helps shape what “value” means for people living with aspergillosis.
🌱 In summary
The NHS is moving from counting treatments to counting outcomes.
For people with aspergillosis, that means care that’s more personalised, joined-up, and focused on what really matters — your health, comfort, and quality of life.
The National Aspergillosis Centre is well placed to lead this change and to show how specialist, patient-centred care can deliver real value for people with complex lung disease.

🌧️ Damp Homes and Aspergillosis: Why This Matters
If you live with aspergillosis, asthma, or other chronic lung conditions, your home environment plays a vital role in how well you stay.
Dampness, mould, and poor ventilation allow fungi — including Aspergillus — to grow and release spores into the air. Breathing in these spores can irritate airways, trigger allergic reactions, or worsen infection risk.
That’s why the NAC CARES team has gathered the latest UK policy, research, and practical guidance on this issue — all now available on our new information hub:
👉 Damp Homes – UK Policy and Research
🏠 What’s New on the Aspergillosis.org Damp Homes Page
Over the past week, the NAC CARES team has published a series of new articles and updates that help you:
1. Understand the Health Risks
-
How damp and mould can worsen breathing symptoms or trigger flare-ups in conditions like Chronic Pulmonary Aspergillosis (CPA) and Allergic Bronchopulmonary Aspergillosis (ABPA).
-
Why people with weakened lungs or immune systems are especially at risk.
-
The hidden signs of mould exposure — condensation, musty odours, or discoloured walls — even when no visible black mould is seen.
2. Learn About Your Rights and What to Do
-
What to check if you rent your home and find damp or mould.
-
Step-by-step guidance on how to report problems, who is responsible for fixing them, and what help is available if landlords or councils don’t act.
-
Links to official UK guidance, including the Awaab’s Law updates, which strengthen tenants’ rights to safe housing.
3. Keep Up with the Latest Research and Policy
-
Summaries of recent UK housing and health studies connecting damp homes to respiratory illness.
-
Insights into national policy changes — including new housing safety standards and public health responses.
-
Easy-to-read summaries of scientific studies showing how mould affects airways and immune response in vulnerable patients.
🧰 How to Use the New Page
-
Start with the main hub: Damp Homes – UK Policy and Research.
This gathers all the latest NAC CARES articles, research links, and resources in one place. -
Explore by topic:
-
Health & Risk – what damp means for your lungs.
-
Practical Advice – how to spot and deal with mould.
-
Policy & Research – what the UK government and researchers are doing to address the problem.
-
-
Take action:
Use the linked materials when talking with your GP, local council, or housing officer. Having official NHS and government evidence can help you get faster results.
💬 Key Takeaways for Aspergillosis Patients
-
Keep your home dry, warm, and well-ventilated.
-
Report damp or mould promptly to landlords or housing providers — and keep written records.
-
If your symptoms worsen and you suspect environmental triggers, speak with your care team at NAC or your respiratory specialist.
-
Use the NAC CARES Damp Homes page as a trusted, evidence-based guide to understanding your risks and your rights.

Share your feedback about your care at the National Aspergillosis Centre
There’s now a new way to read and share patient feedback about local NHS hospitals online. All comments come directly from patients and carers.
That’s because NAC sits within the Infectious Diseases service, which is managed through North Manchester as part of the new Manchester University NHS Foundation Trust (MFT) structure.

💬 Healthwatch: Your Local Voice in the NHS
Living with a long-term lung condition such as aspergillosis, asthma, or bronchiectasis often means regular contact with hospitals, GPs, and community clinics.
Sometimes things work well — and sometimes they don’t.
That’s where Healthwatch comes in.
Healthwatch is an independent organisation that represents patients and the public.
It exists to make sure your experiences help shape the way NHS and social-care services are delivered.
🏛️ What is Healthwatch?
Healthwatch was set up by law to be the official voice of patients and the public in health and social care.
There are two levels:
-
Healthwatch England – works nationally to influence NHS and government policy
-
Local Healthwatch – works in every local authority area across England, gathering feedback from people using local services
Healthwatch is not part of the NHS, and it’s not a complaints service, but it does have statutory powers to:
-
Listen to people’s experiences of care
-
Report issues and make recommendations to the NHS, local councils, and care providers
-
Request responses from organisations it investigates
-
Escalate serious concerns to the Care Quality Commission (CQC)
Learn more on the Healthwatch website.
🌿 Why Healthwatch matters to aspergillosis patients
People living with chronic lung disease often face delays, limited understanding, or difficulties accessing ongoing support.
Healthwatch helps make sure those experiences aren’t ignored.
1. Raising the patient voice
You can share your experience of healthcare — good or bad — with your local Healthwatch.
They collect stories from across the community and use them to:
-
Identify patterns (for example, problems with accessing respiratory clinics or antifungal monitoring)
-
Produce reports and recommendations for local NHS decision-makers
-
Push for improvements to long-term care pathways and community support
2. Helping to improve new neighbourhood health hubs
As NHS care moves into the community, Healthwatch plays a key role in making sure new Neighbourhood Health Hubs are:
-
Accessible for people with limited mobility or oxygen needs
-
Located where public transport and parking work for patients
-
Designed with chronic-illness patients in mind, not just short-term care
You can feed in your ideas through Healthwatch about what’s working and what isn’t in new NHS community models.
3. Providing information and signposting
If you’re unsure where to go for care — GP, hospital, or new health hub — or how to complain or appeal a service decision, Healthwatch can point you in the right direction.
They offer clear, local information about:
-
NHS patient transport
-
The Healthcare Travel Costs Scheme (HTCS)
-
Local support groups and community services
4. Supporting patient involvement
Healthwatch works with NHS organisations to include patients and carers in planning and reviewing services.
If you’d like to get involved as a patient representative or share your experience of aspergillosis services, Healthwatch can help you join local working groups or consultations.
5. Spotlighting inequalities
Healthwatch highlights where certain groups are left behind — for example:
-
People with rare or complex conditions
-
Patients in rural or deprived areas
-
Those unable to use digital appointment systems
This helps ensure people with chronic lung conditions are not overlooked when new community-care models are designed.
⚖️ What Healthwatch can — and can’t — do
| ✅ Healthwatch can | 🚫 Healthwatch can’t |
|---|---|
| Collect and report your experience to NHS leaders | Fix individual clinical problems directly |
| Influence NHS and council decisions | Guarantee faster treatment or appointments |
| Provide advice on local services and support | Replace legal or complaints services |
| Escalate major safety concerns to the CQC | Act as your personal advocate in disputes |
Even so, their influence can be powerful — many improvements in NHS access and transport have started with patient stories collected by Healthwatch.
📍 How to contact your local Healthwatch
Every local area has its own Healthwatch website and phone number.
You can find yours at:
👉 Find your local Healthwatch
When you contact them, you can:
-
Fill in a short online form to share your story
-
Ask to join a focus group or consultation
-
Request accessible information or help finding services
-
Subscribe to local updates and reports
If you’d like support from the aspergillosis community, NAC CARES can also help you write or submit your feedback.
💬 Why this matters
“Nothing about us without us.”
Healthwatch exists so that patients — including those with rare and chronic conditions like aspergillosis — can make their experiences count.
By telling your story and feeding back to Healthwatch, you help shape better care for yourself and for others who will face similar challenges in future.

🏥 NHS Neighbourhood Health Hubs: How Community Care Will Work for People with Aspergillosis and Asthma
The NHS is changing how healthcare is delivered — with more care moving closer to home and fewer hospital visits.
A new model called Neighbourhood Health Services (or Neighbourhood Health Hubs) is being rolled out across England from late 2025, and it could make a real difference for people living with aspergillosis, asthma, bronchiectasis, and other long-term respiratory conditions.
🌍 Why care is moving into the community
The goal is to:
-
Bring care to where people live, not just in large hospitals
-
Reduce waiting times by shifting routine tests and reviews out of hospital clinics
-
Join up GPs, nurses, pharmacists, and hospital specialists into one local team
-
Focus on prevention, self-management, and early support
These reforms come from the government’s Healthcare on Your Doorstep announcement (September 2025), supported initially by £10 million across 43 pilot areas in England.
🧑⚕️ What a “Neighbourhood Health Hub” looks like
A one-stop local health centre bringing together:
-
GPs and practice nurses
-
Respiratory nurses, physiotherapists, and pharmacists
-
Mental-health and wellbeing workers
-
Dietitians, occupational therapists, and social-prescribing link staff
-
Voluntary and community organisations (e.g. NAC CARES, Asthma + Lung UK)
Some hubs will connect directly to Community Diagnostic Centres (CDCs) – local sites providing CT, MRI, X-ray, lung-function and blood tests through the NHS England diagnostics programme.
The aim is for one joined-up team to share your records and plan your care locally.
🩺 How hubs work with your GP and A&E
The new hubs are designed to fill the gap between GP surgeries and hospitals – giving extra support when you’re too unwell to manage alone but don’t need emergency care.
🏠 Your GP surgery
You’ll stay registered with your usual GP. They remain in charge of your prescriptions, results, and overall care.
Your GP can now refer you to a Neighbourhood Health Hub for things that need a wider team – for example:
-
Antifungal monitoring or blood tests
-
Lung-function or CT scans
-
Flare-up review by respiratory nurses
-
Fatigue or wellbeing support
🧑⚕️ The Neighbourhood Health Hub
You might go here instead of hospital for:
-
Same-day assessment of an infection or flare-up
-
Bloods, ECGs, or scans ordered by your GP
-
Physiotherapy, airway-clearance or rehabilitation
-
Medication reviews with a pharmacist
-
Appointments with dietitians or mental-health staff
-
Practical help from link workers (see below)
🚨 A&E (Emergency Department)
Still essential for serious problems such as:
-
Sudden or severe breathlessness not relieved by treatment
-
Coughing up blood
-
Chest pain, fainting, or collapse
-
High fever with confusion
If unsure, call NHS 111 or 999 in an emergency.
🔁 When to use which service
| Situation | Who decides | Where you’ll be seen |
|---|---|---|
| Routine check-up or repeat prescription | You / GP | GP surgery |
| Specialist review or complex medication | GP / consultant | Neighbourhood Hub |
| Mild flare-up needing same-day care | NHS 111 / GP | Hub or GP |
| Emergency or life-threatening symptoms | NHS 111 / 999 | A&E / hospital |
| Diagnostic tests | GP / hospital referral | Community Diagnostic Centre |
All sites will share your digital care record so results and updates reach your GP and hospital team automatically.
🧑🤝🧑 Link workers and care coordinators – local help through your GP
Every GP practice and neighbourhood team now has link workers (also called care coordinators or social prescribers).
They’re there to help you navigate healthcare and community support. They can:
-
Arrange or advise on transport for appointments
-
Help complete travel cost reimbursement or benefit forms
-
Connect you with volunteer driver schemes or local charities
-
Find exercise, wellbeing, or peer-support groups
-
Support with fatigue, isolation, or anxiety
Ask your GP reception or Neighbourhood Hub to refer you to the link worker, or request a call-back via the NHS App.
🚗 Transport and accessibility
🚐 NHS Patient Transport Service (PTS)
If you can’t use public transport for medical reasons (for example, oxygen use, mobility difficulties, or severe fatigue), you may qualify for free NHS transport.
Your GP, link worker, or hospital can book this for you through the regional PTS (for example, NWAS in the North West).
💷 Healthcare Travel Costs Scheme (HTCS)
If you’re on a low income or certain benefits, you can reclaim travel expenses under the HTCS.
Bring your appointment letter and proof of eligibility, or ask your link worker to help with the form.
🚙 Community & volunteer transport
Each Integrated Care System (ICS) works with local councils and charities such as Age UK, Mind, or Good Neighbour schemes to run community minibuses and volunteer driver services.
Ask your link worker or hub team for local options.
🅿️ Accessibility
All new and refurbished hubs must include:
-
Blue Badge parking and drop-off zones
-
Wheelchair-friendly entrances and toilets
-
Seating and oxygen-safe waiting areas
-
Negotiated free or reduced parking in shared sites
🧭 At a glance
| Issue | What’s planned | What to do now |
|---|---|---|
| Public transport | Sites chosen to be local, but not always central | Check routes before your visit |
| NHS Patient Transport | Still available for medical need | Ask GP or link worker to book |
| Travel-cost reimbursement | Continue via HTCS | Keep proof of benefit |
| Community / volunteer drivers | Expanding under ICB–VCS partnerships | Request info via link worker |
| Disabled parking / drop-off | Required at new sites | Confirm when booking |
🪶 A message from the aspergillosis community
For many people with lung disease, “local care” only works if it’s accessible care.
Groups such as NAC CARES, Asthma + Lung UK, and Healthwatch are urging NHS leaders to:
-
Design transport and parking into every new site
-
Ask about mobility and oxygen needs when booking
-
Fund local volunteer schemes
-
Provide dedicated link workers at every hub and GP practice
If you struggle to reach appointments, tell your clinic or Healthwatch — your feedback shapes how services develop.
🧾 Questions to ask before your first visit
-
🚗 Is there Blue Badge or patient parking on site?
-
🚌 What public-transport links serve the hub?
-
🚐 Can the clinic arrange NHS Patient Transport?
-
💷 Can I claim travel costs under the HTCS scheme?
-
♿ Is the building accessible for wheelchairs or oxygen users?
-
💨 Are there rest areas for people who get breathless?
-
🧑🤝🧑 Can my carer or partner attend with me?
-
👩💼 Is there a link worker who can help with transport or forms?
-
🕓 Are there quiet waiting spaces to reduce infection risk?
Having these answers before your appointment makes your visit smoother and safer.
💬 Final thought
“Neighbourhood care” isn’t about replacing your GP or A&E — it’s about bridging the gap.
The new hubs aim to bring together your GP, hospital specialists, and community teams in one local setting, providing earlier help, fewer hospital journeys, and care designed around your life, not your postcode.
🔎 Behind the Headlines: Is this an NHS Expansion or a Shift?
Many people wonder whether this is new investment or a reshuffle of existing NHS services.
🧱 What’s really happening
-
The Neighbourhood Health Service is not a new tier of the NHS, but a redesign of how GP, hospital, and community teams work together.
-
The focus is on moving care out of hospitals and into local clinics, using the same staff and budgets more effectively.
-
Hospitals will still handle emergencies and complex cases, but routine tests, reviews, and education will move into the hubs.
⚖️ Expansion or movement?
| Area | Expansion | Reorganisation |
|---|---|---|
| Buildings | Some new or refurbished hubs and diagnostics centres | Many reusing existing GP or community facilities |
| Staffing | Some new link workers, pharmacists, and AHPs | Most existing NHS staff redeployed across neighbourhoods |
| Funding | £10m pilot investment + diagnostic capital | No major long-term new funding yet announced |
| Patient benefit | Easier access, joined-up records | May reduce hospital appointments rather than add capacity |
💬 What this means
For patients, it should feel like an expansion — more care, closer to home —
but in reality it’s a shift of where and how NHS services are delivered, not a large-scale increase in total NHS resources.
⚠️ Risks and opportunities
| Opportunities | Risks |
|---|---|
| Easier local access | Risk of hospital clinics closing before hubs fully staffed |
| Joined-up records | Depends on IT integration |
| Focus on prevention | May feel like hospital services are being reduced |
| Better continuity | Needs clear accountability (GP vs hub) |
🧩 Summary
The new neighbourhood model is a reorganisation within the NHS, not a separate expansion.
It aims to use existing staff, buildings, and budgets more efficiently — giving patients with chronic conditions like aspergillosis and asthma easier access to care and support in their own communities.
Integrated Care Boards (ICBs): What They Are and How Patients Can Contact Them

What is an ICB?
-
An Integrated Care Board (ICB) is the NHS organisation that replaced Clinical Commissioning Groups (CCGs) in July 2022.
-
Each ICB plans and funds NHS services across a large region (1–3 million people).
-
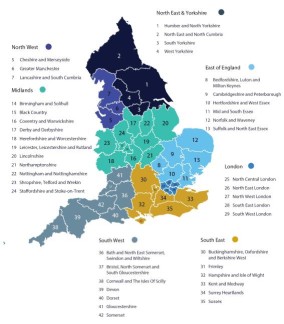
England has 42 ICBs, covering the whole country (see full list plus contact details here).
-
They hold the NHS budget locally, decide which services are provided, and work with councils and community organisations.
- Scotland, Wales and Northern Ireland have a different system
Why might a patient need to contact an ICB?
Patients don’t normally deal with ICBs day-to-day (you’ll usually go to your GP, hospital, or local Patient Advice and Liaison Service). But there are situations where you may want or need to reach out:
-
Feedback or complaints about NHS services that can’t be resolved at GP or hospital level.
-
Service changes – ICBs must consult the public when they change how services are delivered (e.g. reorganising clinics, closing or merging hospital departments).
-
Patient voice – ICBs have teams dedicated to patient and public involvement. You can join forums, respond to surveys, or attend public meetings.
-
Access to care – if you are struggling to access a specialist service or want to know what’s available in your area, ICBs can advise.
-
Equality of access – raising concerns if a particular group or community is being left behind.
How can a patient contact an ICB?
-
Patient Experience / Engagement Teams: Every ICB has an email and phone number for patients. Look for “Get Involved” or “Contact Us” on their website.
-
PALS escalation: If PALS (Patient Advice and Liaison Service) can’t resolve your concern, they can refer it up to the ICB.
-
Public board meetings: ICBs must hold regular meetings in public where patients can submit questions.
-
Healthwatch: Your local Healthwatch can raise issues directly with the ICB on your behalf.
✅ In summary:
Patients usually don’t need to contact an ICB for routine issues, but if you want your voice heard about service changes, access problems, or unresolved complaints, the ICB is the organisation responsible for commissioning services in your area.

Comparing Health Systems: NHS vs Insurance-Based Models

Healthcare looks very different depending on where you live, and it can be informative to look at the pros and cons of each system.
The UK’s NHS model is often contrasted with insurance-based systems such as those in the US and Germany. All aim to look after patients, but they differ in cost, access, caution with new medicines, and their contribution to research.
1. Funding and Access
NHS (UK)
-
Publicly funded through taxation.
-
Care is free at the point of use.
-
Limited co-payments (e.g. prescriptions in England, but free in Scotland/Wales/NI).
Insurance-Based (US, Germany)
-
US: Mix of private insurance, employer-based plans, and public programs (Medicare/Medicaid). Patients often pay premiums, deductibles, and co-pays.
-
Germany: Statutory health insurance (public) plus private options. Patients contribute through payroll and some co-payments.
✅ Equity difference: The NHS ensures universal coverage. Insurance systems can create gaps — in the US, uninsured or underinsured patients face very high bills.
2. Cost
-
United States: ~16–17% of GDP, >$12,000 per person per year.
-
Germany: ~11–12% of GDP, ~$6,000–7,000 per person.
-
United Kingdom: ~10% of GDP, ~$4,500 per person.
✅ Insurance-based systems are much more expensive overall. The NHS achieves lower cost per head but sometimes with tighter rationing.
3. Approach to New Medicines
NHS (cautious, evidence-driven)
-
Drugs are appraised by NICE (National Institute for Health and Care Excellence).
-
Only those proven clinically effective and cost-effective are routinely available.
-
Access can be slower, but ensures sustainability and safety.
Insurance-Based (faster, autonomy-driven)
-
Once a drug is licensed (FDA in US, EMA in EU), doctors may prescribe it, often off-label.
-
Patients may be offered newer or experimental options earlier.
-
Shared decision-making: “This might help, here are the risks, do you want to try it?”
✅ Trade-off: Insurance systems offer earlier access, but higher risk of side effects, wasted cost, and overuse. NHS offers more consistency but less flexibility.
4. Risks of Wide Access
Allowing rapid use of new drugs can lead to:
-
Harm to patients:
-
US:
-
Vioxx (rofecoxib) was widely prescribed for arthritis before long-term data was available → later linked to tens of thousands of excess heart attacks and strokes.
-
Opioid overprescribing (encouraged by drug companies, reimbursed by insurers) fuelled a public health crisis, with millions addicted and >500,000 deaths.
-
-
Germany: Wider acceptance of MCAS and other “working diagnoses” sometimes leads to long-term medication without solid evidence, exposing patients to risks without clear benefit.
-
-
Harm from NHS caution:
-
UK:
-
Cystic fibrosis drug Orkambi: available in the US and Germany years earlier, but withheld in the UK until 2019 due to cost-effectiveness debate → children and young adults missed out on years of treatment.
-
Cancer immunotherapies: delays in NICE approval have meant some patients only got access through special trials or not at all, potentially shortening survival.
-
-
5. Doctor–Patient Conversations
-
Insurance systems: “You may have this condition, and drug X or Y might help. It’s your choice.”
-
NHS: “We know you have this condition. X is proven and available. Y is unproven or not funded, so we cannot recommend it.”
✅ Insurance systems emphasise autonomy and options. The NHS emphasises evidence and fairness.
6. UK Private Healthcare vs US Healthcare
It’s tempting to think the UK private sector is equivalent to the US system, but they are very different.
UK Private Care
-
Covers about 10–12% of the population, mainly for elective surgery, scans, and faster consultant appointments.
-
Usually funded by employer insurance or self-pay.
-
Still relies on the NHS for emergencies and complex care.
-
New medicines still follow NICE approval — patients don’t usually get earlier access to unapproved drugs.
US Healthcare
-
Insurance-based and the default system, covering almost everyone.
-
Patients pay premiums, deductibles, and co-pays — bills can be catastrophic without good cover.
-
Emergencies are treated but still billed.
-
Patients may access new drugs and technology earlier, but often at very high cost.
✅ Bottom line: UK private care is an add-on to the NHS, giving faster access but within the same medical framework. The US system is entirely insurance-driven, with no NHS-style universal fallback.
7. Research Strengths
-
Insurance-based systems (esp. US):
-
Huge budgets (NIH + pharma).
-
Early adoption → more real-world data.
-
Specialist centres attract rare-disease patients.
-
-
NHS system:
-
Unified data across the whole population.
-
Ability to run massive pragmatic trials cheaply (e.g. RECOVERY during COVID: identified dexamethasone as life-saving within weeks).
-
More representative recruitment because care is universal.
-
✅ Together they complement each other:
-
New drugs are often developed and trialled first in the US/Germany.
-
Large-scale validation and population-level studies often happen in the UK.
8. Which System Is “Better”?
It depends what you value most:
-
Insurance-based systems:
-
More expensive
-
Faster access to innovation
-
More choice and autonomy
-
Higher risk of harm and inequality
-
-
NHS:
-
Less expensive
-
Slower, more cautious
-
Equitable and universal
-
Sometimes frustratingly restrictive
-
✅ Bottom Line
No system is perfect.
-
Insurance-based systems favour speed, choice, and innovation — but have caused harm through early adoption of unsafe drugs, opioid overuse, and inequitable access.
-
The NHS favours equity, safety, and sustainability — but has harmed patients by delaying access to life-saving treatments while cost-effectiveness was debated.
-
UK private healthcare is not a parallel US-style system: it is simply a faster lane within the NHS framework, not an alternative to universal coverage.
The reality is that both types of systems need each other: innovations often emerge in the US/Germany, while the NHS provides the gold standard for large-scale testing and equitable delivery.

Autumn 2025 COVID-19 Booster – What Aspergillosis Patients Need to Know
The UK Health Security Agency (UKHSA) has updated who will be offered the COVID-19 booster this autumn. The programme is now more limited than in 2024, so it’s important to know if you qualify.
Who will be offered the booster?
You can get a free COVID-19 booster this autumn if you are:
-
Aged 75 or over
-
Living in a care home for older adults
-
Aged 6 months or older and immunosuppressed
This is a change from 2024, when everyone aged 65+ and many other clinical risk groups were included.
What “immunosuppressed” means
Many people with aspergillosis fall into this category. You may be considered immunosuppressed if you are:
-
Taking systemic steroids for more than a month
-
Receiving biologic therapy or other immunomodulatory medication
-
Living with a condition that affects your immune system
-
Having had chemotherapy, radiotherapy, or a transplant
If you’re unsure whether this applies to you, check with your GP or hospital specialist.
Timing of the booster
-
Boosters are usually offered at least 6 months after your last dose, including the spring booster.
-
Even if you’ve never had a COVID-19 vaccine before, you can still get one this autumn if you are in one of the eligible groups.
Why this matters for aspergillosis patients
People with aspergillosis often have weaker lungs and higher risks from infections. If your immune system is also suppressed by medication or illness, COVID-19 can be more severe. The booster offers added protection during the winter months.
💙 Key advice:
-
If you are immunosuppressed or over 75, you should be offered the vaccine.
-
If you think you qualify but haven’t received an invitation, speak to your GP or specialist.
-
Don’t delay — protecting yourself against COVID-19 is especially important when living with aspergillosis.
📌 Full details from UKHSA: Who’s eligible for the 2025 COVID-19 vaccine or autumn booster