Browse information
Latest Articles
Support
For Professionals
Search
lung-function
Home
Posts Tagged "lung-function"
lung-function
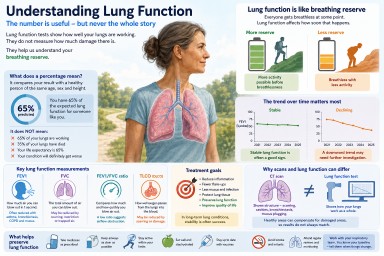
Understanding Lung Function in Aspergillosis and Asthma
by GAtherton
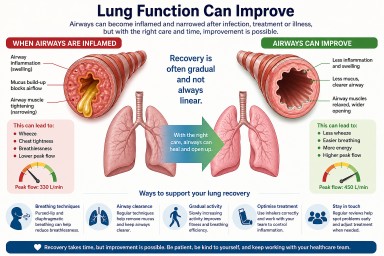
Can Lung Function Improve After Infection or Treatment?
by GAtherton