SAFS / Severe Asthma
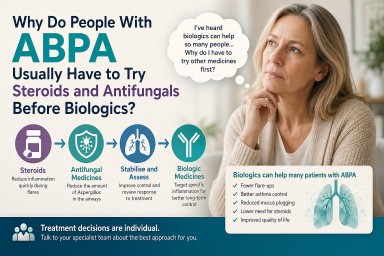
Why Do People With ABPA Usually Have to Try Steroids and Antifungals Before Biologics?
Last reviewed: June 2026…


⭐ Severe Asthma with Fungal Sensitisation (SAFS): The Hidden Burden Behind Difficult Asthma
Estimated prevalence: 15–30%…


🌬️ Breathing Easier: Keeping Your Air Clean at Home, Work and When Travelling
People with lung conditions…
