Living with Aspergillosis



Exercise and Aspergillosis: How Physical Activity Can Improve Breathing, Strength and Wellbeing
Last reviewed: June 2026 Key…

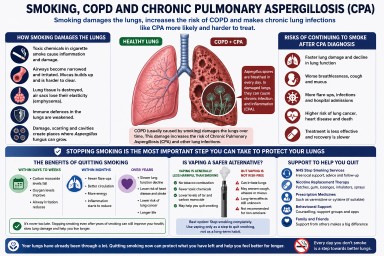

Blue inhalers, combination inhalers and aspergillosis: what patients need to know
Recent news about “blue…