Browse information
Latest Articles
Support
For Professionals
Search
Living with Aspergillosis
Home
Archive by Category "Living with Aspergillosis"
(
Page 2
)
Living with Aspergillosis
Preparing for a Disability Assessment: A Practical Guide for People Living with Aspergillosis in UK
Originally published: August…
by GAtherton
Choosing the Right Face Mask for Aspergillosis | FFP2, FFP3 & Mould Protection
by GAtherton
Trying a New Diet? A Guide for People with Aspergillosis
by GAtherton
Loosen and Clear Mucus: Practical Self-Help Techniques for People with Aspergillosis
by GAtherton
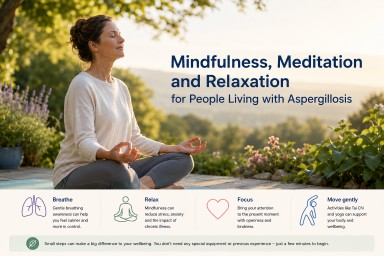
Mindfulness, Meditation and Relaxation for People Living with Aspergillosis
by GAtherton
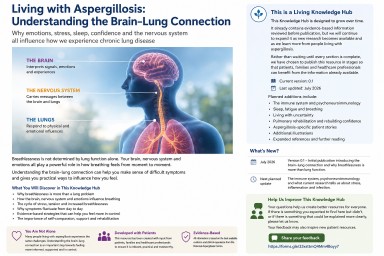
Living with Aspergillosis: Understanding the Brain–Lung Connection
by GAtherton
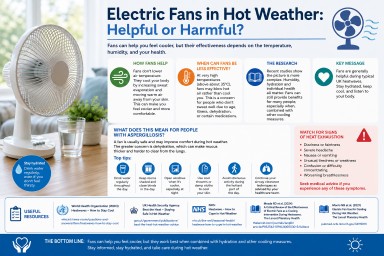
Electric Fans in Hot Weather: Helpful or Harmful?
by GAtherton
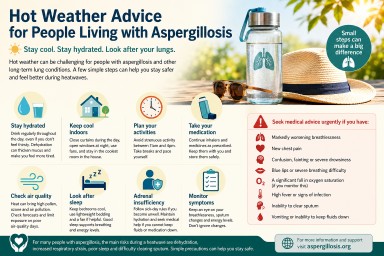
Hot Weather Advice for People Living with Aspergillosis
by GAtherton
The Hidden Job Nobody Talks About: Living with Chronic Illness
by GAtherton
Living Safely with Pets When You Have Aspergillosis
by GAtherton
1
2
3
4
…
43