Browse information
Latest Articles
Support
For Professionals
Search
Housing & Damp
Home
Environment
Archive by Category "Housing & Damp"
Housing & Damp
Damp, mould and health in 2026: what we know, what has changed and what people can do
by GAtherton
How to Remove Mould from Your Washing Machine and Stop It Coming Back
by GAtherton
Damp Homes
Damp homes Why are damp…
by GAtherton
Help Us Improve Our Damp Homes and Health Questionnaire
by GAtherton
Join our UK Citizen Science Project on Damp Homes and Health
by GAtherton
Damp, Mould and Aspergillosis: A Practical Guide for Patients Worried About Their Home
People with aspergillosis,…
by GAtherton
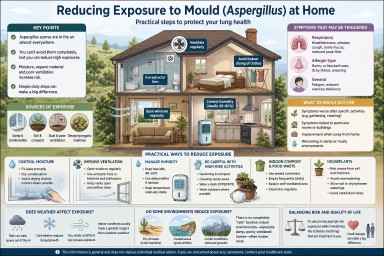
Reducing Exposure to Mould (Aspergillus) at Home
by GAtherton
Houseplants and Aspergillosis: Do You Need to Get Rid of Them?
by GAtherton
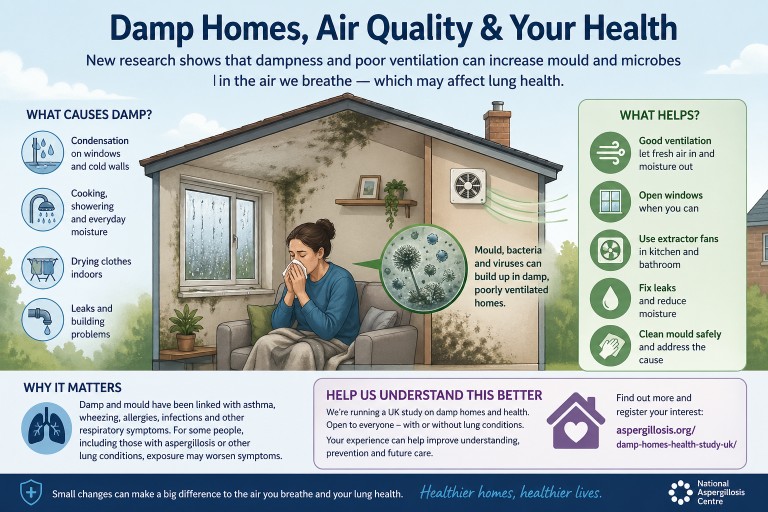
Damp Homes, Indoor Air and Health: What a Recent Evidence Review Tells Us
by GAtherton
Help us understand how damp homes affect health
by GAtherton
1
2
3
…
6